Russian Call Girls in Pune Tanvi 9907093804 Short 1500 Night 6000 Best call g...
Intra-articular Distal Radius Fractures
1. P A R T N E R S O R T H O P A E D I C
Trauma Rounds
Case Reports from the Mass General Hospital and Brigham & Women’s Hospital
A Quarterly Case Study Volume 2, Winter 2011
Intra-articular Distal Radius Fractures
Brandon E Earp, MD (multiple plate) fixation, intramedullary
fixation, spanning internal fixation, and
Your patient comes in after volar locked plating.1 Fortunately for our
a mechanical fall onto an patients, a skilled surgeon familiar with
outstretched hand. A sig- these techniques can achieve a satisfactory
nificant deformity of the outcome by choosing any one of several
wrist and edema are noted treatment options for the particular frac-
clinically and the patient’s ture pattern.
discomfort is obvious. Radiographs demon- Increasingly, volar locked plating has
strate a displaced, dorsally angulated distal gained popularity for its reliability, low
radius fracture with loss of radial height, complication rate, and ability to allow
radial translation, and intra-articular in- more rapid return of motion and function.2
volvement. You see the patient, perform an Assuming appropriate reduction and posi-
appropriate clinical workup, reduce and tioning are achieved, the volar locked plate
splint the fracture. will allow early mobility even in osteo-
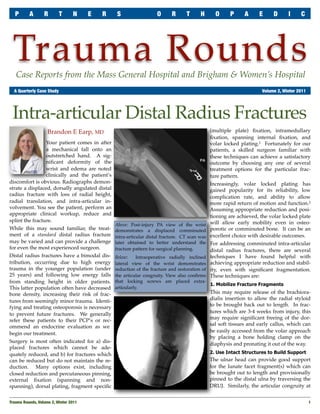
Above: Post-injury PA view of the wrist
While this may sound familiar, the treat- demonstrates a displaced comminuted porotic or comminuted bone. It can be an
ment of a standard distal radius fracture intra-articular distal fracture. CT scan was excellent choice with desirable outcomes.
may be varied and can provide a challenge later obtained to better understand the For addressing comminuted intra-articular
for even the most experienced surgeon. fracture pattern for surgical planning. distal radius fractures, there are several
Distal radius fractures have a bimodal dis- Below: Intraoperative radially inclined techniques I have found helpful with
tribution, occurring due to high energy lateral view of the wrist demonstrates achieving appropriate reduction and stabil-
trauma in the younger population (under reduction of the fracture and restoration of ity, even with significant fragmentation.
25 years) and following low energy falls the articular congruity. View also confirms These techniques are:
from standing height in older patients. that locking screws are placed extra-
1. Mobilize Fracture Fragments
This latter population often have decreased articularly.
bone density, increasing their risk of frac- This may require release of the brachiora-
dialis insertion to allow the radial styloid
tures from seemingly minor trauma. Identi-
to be brought back out to length. In frac-
fying and treating osteoporosis is necessary
tures which are 3-4 weeks from injury, this
to prevent future fractures. We generally
may require significant freeing of the dor-
refer these patients to their PCP’s or rec-
sal soft tissues and early callus, which can
ommend an endocrine evaluation as we
be easily accessed from the volar approach
begin our treatment.
by placing a bone holding clamp on the
Surgery is most often indicated for a) dis- diaphysis and pronating it out of the way.
placed fractures which cannot be ade-
quately reduced, and b) for fractures which 2. Use Intact Structures to Build Support
can be reduced but do not maintain the re- The ulnar head can provide good support
duction. Many options exist, including for the lunate facet fragment(s) which can
closed reduction and percutaneous pinning, be brought out to length and provisionally
external fixation (spanning and non- pinned to the distal ulna by traversing the
spanning), dorsal plating, fragment specific DRUJ. Similarly, the articular congruity at
Trauma Rounds, Volume 2, Winter 2011
1
2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S
the radiocarpal joint can be re-established using the intact tem- There are rare times when I use a provisional external fixator to
plate of the proximal articular surface of the proximal carpal provide longitudinal traction, which then frees my hands to
row. Any depressed segments can be tamped up to restore the manipulate and fix the articular segments.
joint. Occasionally a dorsal peek hole incision can be used to Important Considerations with Comminuted Fractures
visualize those segments; sometimes I find the use of a wrist
Try to position the plate such that the locking screws are just
scope helpful in seeing the segments arthroscopically.
under the subchondral bone. This allows for a better rafting or
3. Build the Fracture Back to the Plate supportive effect and minimizes settling of the fracture. This
A third technique is to use the plate to help you. If it is not pos- technique has the obvious risk that the hardware could be
sible to achieve provisional reduction with C-wires, you could placed too distal and the locking screws could broach the joints
place the plate on the volar aspect of the distal radius and se- (both radiocarpal and DRUJ). But this risk can be easily
cure it to the diaphysis with C-wires through the plate. This avoided with careful attention to screw placement through se-
allows for easy plate adjustment without making large drill rial intraoperative fluoro imaging. The view I depend on sub-
holes. The articular segments are then reassembled starting ul- stantially to determine my subchondral screw placement is the
narly. The surgeon can work through the fracture from the ra- lateral view taken with the forearm radially inclined (~ 23 de-
dial aspect and use a freer or other elevator to manipulate the grees), which allows a true tangential view of the articular sur-
volar lunate facet fragment into place. If there is a coronal split, face. Many volar plating systems have multidirectional locking
the dorsal ulnar piece will need to be reduced at the same time. screw capability allowing the surgeon greater flexibility to posi-
A C-wire is then placed through the plate into those segments. tion the plate more distally and still get locking capability,
It may be appropriate to then place the whereas the standard fixed angle lock-
locking screws into those fragments to ing screw trajectory would put those
achieve initial ulnar stability. Any in- screws into the joint.
tervening central fragments are reduced Summary
by tamping them up to restore the joint
Volar locked plating technique typically
surface if needed and then reducing
provides adequate stability to allow for
them to the lunate facet. By flexing the
an early range-of-motion rehabilitation
wrist and placing a rolled towel under-
protocol. With restoration of the frac-
neath, the fracture fragments are ma-
ture alignment and stabilization, most
nipulated to deliver them up to the
patients will have an excellent progno-
plate until they can be fixed there, al-
sis for healing and return of function.
lowing for restoration of the volar tilt,
which will be predetermined by the References
implant choice. The radial styloid is 1. Nana AD, et al, Plating of the Distal Radius. J Am
Acad Orthop Surg 2005; 13:159-171.
reduced last; the surgeon should be
2. Rozental TD, et al, Functional Outcomes for Un-
aware that if it is challenging to reduce,
stable Distal Radial Fractures Treated with ORIF and
there may be a rotatory component to Percutaneous Fixation. A Prospective Randomized
the malpositioning rather than just Trial. J Bone Joint Surg Am. 2009; 91(8):1837-46.
length and flexion/extension issues. Above: Post-operative PA view of the wrist shows
Sometimes, bone grafting is indicated reduction of the articular surface. The lunate facet
due to large voids in the metaphyseal is restored to its appropriate height and secured to
Read previous issues & download PDFs:
region. the plate with two locking screws. AchesAndJoints.org/Trauma
Please send correspondence to:
Trauma Faculty Michael Weaver, MD — 617-525-8088 Mark Vrahas, MD / Trauma Rounds
Mark Vrahas, MD — 617-726-2943 BWH Orthopedic Trauma Yawkey Center for Outpatient Care, Suite 3C
Partners Chief of Orthopaedic Trauma mjweaver@partners.org 55 Fruit Street, Boston, MA 02114
mvrahas@partners.org David Ring, MD — 617-724-3953
Mitchel B Harris, MD — 617-732-5385 MGH Hand & Upper Extremity Service Editor in Chief
Chief, BWH Orthopedic Trauma
dring@partners.org Mark Vrahas, MD
mbharris@partners.org Brandon E Earp, MD — 617-732-8064
BWH Hand & Upper Extremity Service Program Director
R Malcolm Smith, MD, FRCS — 617-726-2794
bearp@partners.org Suzanne Morrison, MPH
Chief, MGH Orthopaedic Trauma
(617) 525-8876
rmsmith1@partners.org George Dyer, MD — 617-732-6607 smmorrison@partners.org
BWH Hand & Upper Extremity Service
David Lhowe, MD — 617-724-2800
MGH Orthopaedic Trauma
gdyer@partners.org Editor, Publisher
dlhowe@partners.org www.MassGeneral.org/ortho Arun Shanbhag, PhD, MBA
www.BrighamAndWomens.org/orthopedics
2
Trauma Rounds, Volume 2, Winter 2011