Antiparkinsonian drugs
•
5 likes•1,540 views

1. A 64-year-old architect presents with signs and symptoms consistent with Parkinson's disease, including a resting tremor, stooped posture, dragging of the left leg when walking, and slight unsteadiness. He remains independent in daily activities. 2. The clinical features suggest degeneration of dopaminergic neurons in the substantia nigra, resulting in dopamine deficiency in the basal ganglia and associated motor symptoms. 3. Pharmacological treatment options aim to restore dopamine levels or balance cholinergic and dopaminergic activity in the basal ganglia.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Antiparkinsonian drugs
Similar to Antiparkinsonian drugs (20)
More from Dr.Arka Mondal
More from Dr.Arka Mondal (20)
Recently uploaded
Recently uploaded (20)
Antiparkinsonian drugs
- 1. A 64-year-old architect complains of right-hand tremor at rest, which interferes with his writing and drawing. He also notes a stooped posture, a tendency to drag his left leg when walking, and slight unsteadiness on turning. He remains independent in all activities of daily living.
- 3. It is a Extrapyramidal motor disorder occurs due to degeneration of dopaminergic neurons in the substantia nigra pars compacta (SN-PC) result in dopamine deficiency It occur in 2% elderly population Classically disease of 7th decade of life An imbalance between dopaminergic(inhibitory neuron) and excitatory cholinergic neuron Cholinergic over activity
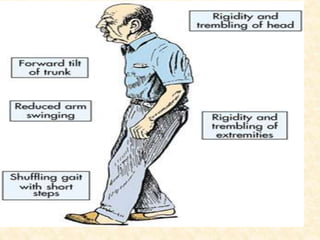
- 4. Characterized by:- Tremors:- Resting tremors Pill-rolling motion of hand Suppressed by-activity ,sleep Gait disturbances/postural instability:- Imbalance and loss of righting reflexes Rigidity-an increase in resistance to passive movement Bradykinesia- slow onset of movement/paucity of movement
- 5. Normal Parkinsonism Treatment In the basal ganglia, the dopaminergic activity is balanced by the cholinergic system Parkinsonism results due to depletion of dopamine in relation to cholinergic activity Also antidopaminergic drugs e.g. Phenothiazines, Haloperidol, methyldopa etc. cause Parkinsonism Pathophysiology & Treatment Pharmacological strategy:- • Restore normal dopamine • Ach activity at muscarinic receptor in the striatum Surgical:- Pallidotomy (lesion). Deep brain stimulation (subthalamic nucleus, globus pallidus internus). Neural transplantation.
- 6. 1.Degeneration of darkly pigmented dopaminergic neurons in substantia nigra.
- 7. 2.Dopamine Neuromelanin 3.Decrease dopamine in neostriatum oxidation Idiopathic Parkinsonism Secondary parkinsonism • Infection- Post-encephalitic parkinsonism • Toxins- Mn, co poisoning • Degenerative disease of CNS- Wilson’s disease • Drugs-Phenothiazines, Butyrophenones Metoclopramide, Haloperidol, Parkinson’s disease
- 8. Anti-parkinsonian Drugs Dopaminergic Drugs Anticholinergic Drugs Dopamine Precursor •Levodopa Dopamine Agonists •Bromocriptine •Pergolide •Premipexole Peripheral Decarboxylase Inhibitors •Carbidopa •Benserazide MAO-B Inhibitor •Selegiline (Deprenyl) •Rasagiline COMT Inhibitor •Entacapone •Tolcapone Dopamine Facilitator Amantadine Anticholinergics •Trihexyphenidyl (Benzhexol) •Procyclidine •Biperiden Antihistaminic •Orphenadrine •promethazine
- 9. Metabolic precursor of dopamine Inactive by itself 95% of an oral dose is decarboxylated in the peripheral tissues (mainly gut and liver) and converted into DA Only about 1-2% of administered levodopa crosses to the brain Always used in combination with carbidopa/benserazide(Peripheral decarboxylase inhibitor ) Levodopa(l-dopa)
- 10. -:Mechanism:-
- 11. levodopa 1. Less dose of Levodopa required and more effect of Levodopa 2. Increased half-life of Levodopa 3. Less side effects of Levodopa, peripherally 4. VitB6 interaction does not occur Dopamine LD LD LD DA DA DA Carbidopa So advantages of the combination are: Carbidopa inhibit the peripheral decarboxylation of Levodopa hence more Levodopa reaches brain Levodopa is usually combined with Carbidopa
- 12. -:Pharmacokinetics:- Absorption:- Absorbed orally by active transport by the presence of food (especially amino acids) Administered on empty stomach Bioavailability affected by: Amino acids present in food compete for the same carrier for absorption (# should be given 30-60 min before meal) Distribution: L-dopa crosses BBB (CNS disturbance) The plasma t 1/2 of levodopa is 1 - 2 hours
- 13. Metabolism:- -Levodopa undergoes high first pass metabolism in G.I. mucosa and liver Excretion:- Urine
- 14. On CNS:- Marked symptomatic improvement occurs in Parkinsonian patients Effect on behavior: ‘General alerting response’ On CVS:- (+inotropic action )-The peripherally formed DA can cause tachycardia acting on β adrenergic receptors DA and NA formed in brain central sympathetic flow-Postural hypotension Pharmacodynamics
- 15. On CTZ:- Dopaminergic receptors are present in this area and DA acts as an excitatory transmitter Peripherally formed DA gains access to the CTZ elicits nausea and vomiting Endocrine action:- DA acts on pituitary mammotropes to inhibit prolactin release In Parkinson's Disease:- Levodopa can reduce all sign and symptoms of PD. It doesn’t stop the progression of disease USES
- 16. At the initiation of therapy:- a) CNS manifestations: 1. Euphoria, anxiety, agitation, insomnia, psychological disturbances as confusion, delusions, hallucinations, 2. Dyskinesia (abnormal involuntary movements which is corrected by dose reduction) b) GIT manifestations:- Anorexia, nausea, and vomiting due to stimulation of D2-receptors in CTZ Tolerance may develop to this adverse effect, but if nausea and vomiting persist, antiemetics are given; e.g. domperidone (D2 antagonist which does not pass BBB) Constipation and bleeding peptic ulcer may occur. Adverse effects
- 17. c) CVS manifestations: Postural hypotension- central sympathetic flow Tachycardia (direct β1stimulation) Hypertension occurs with large doses or with non-selective MAO inhibitors (α1stimulation). Others:- Alteration of smell, taste sensation Abnormal movements-facial tics
- 18. After prolong therapy:- Wearing off phenomenon:- After prolong therapy(3-5 year) Duration of beneficial effect shortens as therapy progress Disease control become poor Fluctuation in symptoms occur frequently -This may be due to the interaction of DOPAC with H2O2 leading to formation of toxic oxygen free radicals which destroy dopamine storage vesicles (this can be prevented by adding selective MAO-B inhibitors as seligeline)
- 19. ‘On-off phenomenon:- may be due to variable levels of dopamine in CNS In on state:- Patient enjoys normal mobility In off state:- loss of beneficial effect of drugs eg-patient unable to raise from chair on which he had sat few min ago. Fluctuation in plasma level because of short half life Treatment:- 1. Sustained released formulation of (L-dopa+carbidopa) 2. COMT-inhibitors 3. Frequent administration of levodopa
- 20. Levodopa Non selective MAO-inhibitor- (hypertensive crisis) Levodopa Vit-B6-(metabolism, therapeutic failure) Levodopa Reserpine, phenothiazine-(block dopamine effect ) Levodopa Tricyclic antidepressant- ( absorption of levodopa ) Contraindication:- Psychoses Narrow angle glaucoma Peptic ulcer Liver & kidney disorder Interaction
- 21. Decrease peripheral decarboxylation of L-dopa Don’t cross BBB. Currently use fixed dose combinations:- L-dopa + carbidopa(4:1/10:1) ratio L-dopa + Benserazide (4:1) Advantage:- (1) BA-dopamine in BG. Hence dose of L- dopa can be reduced by 75% 2.Prolongation of half life of L-dopa 3. Systemic conc.of dopamine, hence incidence of GI- side effect 4. Cardiovascular complication-minimized 5. Better patient compliance Carbidopa
- 22. Dopamine Agonist An alternative to Levodopa-longer duration than levodopa These will act on striatal dopamine receptors even in advanced patients.(more selective receptor action-lesser Side effect) Do not require enzymatic conversion Ergot derivative Don’t require enzymatic conversion to active metabolites Longer duration of action than l-dopa Prevent motor complication Mechanism:- partial D1-Agonist Strong D2-Agonist Bromocriptine
- 23. USES:- 1. Parkinsonism- • can be used alone, use as- adjuent to levodopa • Serves improve control-’wearing of dose’ & ‘on off fluctuation’ 2. Use in suppression of lactation (safer than estrogen) 3.Acromegaly and ACTH-dependent tumors Adverse effect:- hallucination,confusion,vomiting Contraindication:- Peptic ulcer,MI,mental illness
- 24. Ergot derivative Mechanism:- agonist at D1,D2 receptor Pharmacokinetics:- Absorption-rapidly orally Metabolism:- liver by CYP-450 system 50% BA(undergo-first pass metabolism) Excretion:- urine USES:- Idiopathic PD treatment AE:- Dyspepsia,constipation,hallucination Interaction:- pergolide CYP1A2 inhibitor (Ciprofloxacin, Diltiazem)
- 25. It Non-ergot derivative dopamine agonist. It binds to presynaptic& postsynaptic dopamine D2 &D3receptors, but has the highest affinity for the D3 receptor subtype. Mechanism of action :- It stimulates presynaptic and post synaptic dopamine D2 receptors. Therapeutic uses:- Used as monotherapy in early PD. As an adjunct to levodopa in patients with advanced PD. Pramipexole
- 26. Adverse effects:- In early PD nausea, dizziness, constipation, and hallucinations. In patients with advanced disease, the most common adverse effect is orthostatic hypotension. Drug interaction:- cimetidine, ranitidine, diltiazem, verapamil, quinidine,triamterene decrease the oral clearance of pramipexole by 20%.
- 27. Two different types of isoenzymes of MAO are found (MAO –A and MAO-B). MAO-B is responsible for most of the oxidative metabolism of dopamine in the brain. MAO-A is responsible for metabolism of NA,5-HT,tyramine Selective irreversible inhibitors of MAO-B Advantage:- Prolonging T1/2 of Endogenously produce dopamine ↑Anti-parkinsonism effect of dopamine ↓‘On-off’,’wearing off’ phenomena MAO-B inhibitors Selegiline
- 29. Mechanism of action:- Selegiline retard the breakdown of dopamine in the CNS. Blockade of presynaptic dopamine receptors. Inhibition of dopamine reuptake from the synapse. Pharmacokinetics:- Extensively metabolized in the liver. metabolites Desmethyl-selegiline Methamphetamine Adverse effects:- postural hypotension, confusion, psychosis amphetamine
- 30. Interaction:- Seligiline Tricyclic antidepressant Seligiline Pethidine (excitement,rigidity) Seligiline SSRI Contraindication:- Contraindicated in patients with convulsive disorder. Newer selective MAO-B inhibitor. Advantage:- 5 time more potent than seligiline Longer acting Not metabolized to amphetamine Doesn’t produce excitatory side effects Rasagiline
- 32. Reversible COMT-inhibitors Only periphery action Shorter acting drug Mechanism of action:- Entacapone is a selective and reversible inhibitor of COMT . Adverse effects :- Dyskinesia, nausea, diarrhoea, abdominal pain, and urinary discoloration. It increases the side effects of levodopa. Entacapone
- 33. selective and reversible inhibitor of COMT Both action- Peripheral + Central action Longer acting drug SE:- occasionally associated with hepatotoxicity
- 34. Amantadine:- Introduced as an antiviral agent Effective against influenza A2 virus. Mechanism of action: It acts presynaptically and postsynaptically Presynaptically:- 1. release of stored catecholamine from intact dopaminergic terminals 2. Inhibits catecholamine reuptake process at the presynaptic terminal. Dopamine facilitator
- 35. Postsynaptically:- Activation of DA receptors directly. Anticholinergic action. NMDA receptor blocking effect. USES:- Only in milder cases as monotherapy. Supplement to levodopa for advanced cases. It serves to suppress motor fluctuations and abnormal movements. Side effect:- Insomnia, dizziness, confusion, nightmares
- 36. These are the only drugs effective in drug induced parkinsonism. Antimuscarinic agents improve tremor and rigidity but have little effect on bradykinesia. USES:- Iatrogenic Parkinsonism:- anti dopaminergic drug induced Idiopathic parkinsonism: useful in the management of mild-to-moderate symptoms of the PD. Advantage:- Main action –centrally so minimal peripheral action cheaper and better tolerated then L-dopa Adverse effect:- Dry mouth,constipation,drowsiness Central anticholinergic
- 37. Drugs:- Orphenadrine promethazine H1 blockers-addition anti-muscarinic action of acetylcholine Promethazine- tremors,rigidity,sialorrhoea Anti-histaminic
- 38. Blocked of Dopamine receptor in striatum No deficiency of Dopamine Eg.- 1. Antipsychotic Drugs-e.g.-haloperidol,phenothiazines High potent D2 blockers Drugs induce parkinsonism 2.Reserpine-dopamine depleting agent 3.Metoclopramide- cross BBB-block D2 receptor Drug Induced Parkinsonism
- 39. 4.MPTP:- (1-Methy-4-phenyl 1,2,3,6 tetrahydro pyridine) MAO-B metabolized Neurotoxin 5. Oxidative stress:- DOPA-C + H2o2 formation of free radical Degeration of dopaminergic neuron Fe++ Fe+++ Dopamine+O2+H2O
- 40. 1.Classify anti-parkinsonian drugs. Write pharmacological action, AE and therapeutic uses of levodopa. (2)Write Short Notes on:- Levodopa Cheese reaction Dopaminergic agonist MAO-B inhibitors Explain why:- 1.Levodopa is combined with carbidopa 2. Promethazine used in drugs induce parkinsonism
- 41. The most prevalent cause of dementia with Ageing Atrophy of cortical & sub-cortical areas is associated with deposition of -amyloid protein in a form of plaques Accumulation of Aβ initiate inflammation Inflammatory mediators like IL-1,IL-6 Ultimately leads to apoptosis
- 42. Pharmacotherapy:- These drugs provide symptomatic relief but poorly affect the progression of the disease Advantage of drug treatment:- β amyloid (Aβ) production drugs to prevent Aβ aggregation drugs to promote Aβ clearance
- 43. DRUGS FOR ALZHEIMER'S DISEASE Cholinesterase Inhibitors • Donepezil • Rivastigmine • Galantamine • Tacrine NMDA receptor antagonists • Memantine Miscellaneous drugs:- Acetyl-L-carnitine
- 44. N-methyl-D-aspartate (NMDA) receptor antagonist Used as monotherapy and also in combination with Donepezil Mechanism of action:- exert therapeutic effect by blocking NMDA receptors & preventing exitotoxicity Pharmacokinetic:- Well absorbed after oral admistration. Absolute bioavailability of 90% t1/2 - 60-80 hours. Adverse effects:-Agitation, insomnia, hallucination, bronchitis, depression. Memantine
- 45. Therapeutic uses: Mild to moderate dementia Acetyl-L-cartinine:- Intracellular carrier of acetyl groups - mitochondrial membranes - promotes acetylcholine release, choline acetyltransferase activity & potent antioxidant. Investigational product Not recommended - routine use in clinical practice.
Editor's Notes
- Pallidotomy-destroy globus pallidus
- Vit B6 is acts as cofactor with DOPA decarboxylase so increase peripheral conversion of Levodopa to DA
- sudden drop in blood pressure with change in posture-orthostatic hypotension
- DOPAC-dihydroxy phenylacetic Acid 3-MT-3 methoxytyramine
- Pk delt
- DOPAC-dihydroxy phenylacetic Acid 3-MT-3 methoxytyramine