ORIGINAL ARTICLE
Neuromuscular complications after hematopoietic stem
cell transplantation
Susanne Koeppen & Abhiyrahmi Thirugnanasambanthan &
Michael Koldehoff
Received: 19 December 2013 /Accepted: 20 March 2014 /Published online: 29 March 2014
# Springer-Verlag Berlin Heidelberg 2014
Abstract
Purpose The aim of this study was to analyze the occurrence
of neuromuscular symptoms in recipients of allogeneic hema-
topoietic stem cell transplantation (HSCT) for treatment of
malignant hematopoietic disease.
Methods Among 247 outpatients after allogeneic HSCT, we
conducted a prospective non-interventional study between
July 2011 and August 2013. During follow-up visits, clinical
and electrophysiological findings were correlated to the pres-
ence of autoantibodies/alloantibodies and to frequencies of
lymphocyte subpopulations in peripheral blood.
Results Resulting in an incidence of 8.1 %, 20 patients were
diagnosed with neuromuscular complications at a median
onset of 12 months post-transplant. Five patients (25 %) were
identified with polyneuropathy (PNP), ten patients (50 %)
with combined PNP and myopathy, four patients (20 %) with
myopathy or polymyositis (PM), and one patient (5 %) with
myasthenia gravis (MG). Immune-mediated sensorimotor
PNP after HSCT is characterized by a predominantly axonal
lesion and can be overlapping with neurotoxic side effects.
The latency between HSCT and development of PM varied
between 60 days and 72 months. In general, PM occurs
parallel to graft-versus-host disease (GvHD) after tapering of
immunosuppressive medication. Typical clinical features are
proximal bilateral limb weakness with muscle atrophy. Auto-
antibodies (Ab) were detected in 12 patients, myositis-specific
Ab only in one patient. In patients with progressive
neurological symptoms, a decrease in the CD4/CD8 T cell
ratio was observed.
Conclusions GvHD-related myositis appeared similar to idi-
opathic myositis regarding clinical and electromyographical
findings. As outcome measure, sequential analysis of lympho-
cyte subpopulations in peripheral blood seems to be more
suitable than Ab measurements. Whereas peripheral neuropa-
thies are commonly observed shortly after HSCT, MG is a rare
complication in the late post-HSCT phase.
Keywords Allogeneic hematopoietic stem cell
transplantation . Graft-versus-host disease . Polyneuropathy .
Polymyositis . Myasthenia gravis
Abbreviations
AChR Ab Acetylcholine receptor antibody
AL Acute leukemia
ALL Acute lymphocytic leukemia
ANA Antinuclear antibodies
AML Acute myeloid leukemia
Ab Autoantibodies
CK-MB Creatine kinase-MB
CLL Chronic lymphocytic leukemia
CML Chronic myeloid leukemia
GvHD Graft-versus-host disease
HSCT Hematopoietic stem cell transplantation
ND Not done
MCL Mantle cell lymphoma
MG Myasthenia gravis
MM Multiple myeloma
MPN Myeloproliferative neoplasm
OMF Osteomyelofibrosis
PM Polymyositis
PNP Polyneuropathy
S. Koeppen (*): A. Thirugnanasambanthan
Department of Neurology, Medical School, Un.
ORIGINAL ARTICLENeuromuscular complications after hematopo.docx
1. ORIGINAL ARTICLE
Neuromuscular complications after hematopoietic stem
cell transplantation
Susanne Koeppen & Abhiyrahmi Thirugnanasambanthan &
Michael Koldehoff
Received: 19 December 2013 /Accepted: 20 March 2014
/Published online: 29 March 2014
# Springer-Verlag Berlin Heidelberg 2014
Abstract
Purpose The aim of this study was to analyze the occurrence
of neuromuscular symptoms in recipients of allogeneic hema-
topoietic stem cell transplantation (HSCT) for treatment of
malignant hematopoietic disease.
Methods Among 247 outpatients after allogeneic HSCT, we
conducted a prospective non-interventional study between
July 2011 and August 2013. During follow-up visits, clinical
and electrophysiological findings were correlated to the pres-
ence of autoantibodies/alloantibodies and to frequencies of
lymphocyte subpopulations in peripheral blood.
Results Resulting in an incidence of 8.1 %, 20 patients were
diagnosed with neuromuscular complications at a median
onset of 12 months post-transplant. Five patients (25 %) were
identified with polyneuropathy (PNP), ten patients (50 %)
with combined PNP and myopathy, four patients (20 %) with
myopathy or polymyositis (PM), and one patient (5 %) with
myasthenia gravis (MG). Immune-mediated sensorimotor
PNP after HSCT is characterized by a predominantly axonal
lesion and can be overlapping with neurotoxic side effects.
2. The latency between HSCT and development of PM varied
between 60 days and 72 months. In general, PM occurs
parallel to graft-versus-host disease (GvHD) after tapering of
immunosuppressive medication. Typical clinical features are
proximal bilateral limb weakness with muscle atrophy. Auto-
antibodies (Ab) were detected in 12 patients, myositis-specific
Ab only in one patient. In patients with progressive
neurological symptoms, a decrease in the CD4/CD8 T cell
ratio was observed.
Conclusions GvHD-related myositis appeared similar to idi-
opathic myositis regarding clinical and electromyographical
findings. As outcome measure, sequential analysis of lympho-
cyte subpopulations in peripheral blood seems to be more
suitable than Ab measurements. Whereas peripheral neuropa-
thies are commonly observed shortly after HSCT, MG is a rare
complication in the late post-HSCT phase.
Keywords Allogeneic hematopoietic stem cell
transplantation . Graft-versus-host disease . Polyneuropathy .
Polymyositis . Myasthenia gravis
Abbreviations
AChR Ab Acetylcholine receptor antibody
AL Acute leukemia
ALL Acute lymphocytic leukemia
ANA Antinuclear antibodies
AML Acute myeloid leukemia
Ab Autoantibodies
CK-MB Creatine kinase-MB
CLL Chronic lymphocytic leukemia
CML Chronic myeloid leukemia
GvHD Graft-versus-host disease
HSCT Hematopoietic stem cell transplantation
ND Not done
3. MCL Mantle cell lymphoma
MG Myasthenia gravis
MM Multiple myeloma
MPN Myeloproliferative neoplasm
OMF Osteomyelofibrosis
PM Polymyositis
PNP Polyneuropathy
S. Koeppen (*): A. Thirugnanasambanthan
Department of Neurology, Medical School, University of
Duisburg-Essen, Hufelandstraße 55, 45122 Essen, Germany
e-mail: [email protected]
M. Koldehoff
Department of Bone Marrow Transplantation, West German
Cancer
Center, Medical School, University of Duisburg-Essen, Essen,
Germany
Support Care Cancer (2014) 22:2337–2341
DOI 10.1007/s00520-014-2225-0
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT)
has been shown to provide long-term disease-free survival for
otherwise fatal malignant or non-malignant hematological
disorders. With increasing survival rates due to toxicity-
reduced HSCT methods and advanced graft-versus-host dis-
ease (GvHD) management as well as improved antiinfectious
therapy and prophylaxis, a distinct increment in late
transplant-related complications can be observed. Early or
delayed neurological complications usually associated with
GvHD occur in 30–60 % of allogeneic HSCT recipients
[1–3]. Acute GvHD and chronic GvHD remain the major
4. causes of non-relapse mortality, and T cell alloreactivity has
been established as the primary cause of GvHD. The extent of
these complications can vary depending on the type of hema-
tologic disease, stage of diagnosis, age of the transplant pa-
tient, and whether the donor is major histocompatibility com-
plex (MHC) matched or mismatched to the recipient [4, 5].
According to the National Institutes of Health (NIH) consen-
sus criteria, neurological complications associated with
GvHD affect the central or peripheral nervous system or the
musculoskeletal system [6–10]. The most commonly recog-
nized GvHD-related neuromuscular manifestations include
polyneuropathy (PNP), less frequently myopathy, and myas-
thenia gravis (MG) [11–14]. Autoimmune/alloimmune mech-
anisms play a major role in the pathogenesis of neuromuscular
symptoms in the context of GvHD. However, metabolic and
drug-related factors may contribute to the neurologic impair-
ment. The aim of this study was to investigate the incidence
and clinical course of neuromuscular symptoms following
allogeneic HSCT. We also investigated the relationship be-
tween clinical features and laboratory findings.
Methods
Among patients with malignant hematologic disease who
underwent allogeneic HSCT at the West German Cancer
Center, University of Essen, Germany, between July 2011
and March 2013, 20 patients with GvHD-associated neuro-
muscular symptoms were included in this prospective non-
interventional study and followed until August 2013. The
source population in this period included 429 allogeneic
transplant patients, median age 54, and range 17–74 years.
A total of 182 patients with active infectious diseases or
malignancy relapse or who could not tolerate electrophysio-
logical evaluation (n=2) were excluded. The IRB of the
University of Essen approved the study, and written informed
consent was obtained from each patient. Medical records were
5. reviewed to determine diagnosis and treatment of the under-
lying hematologic disease, any comorbidity, the patient’s con-
dition prior to HSCT, and the clinical course until first
neurological evaluation. The neurological status was assessed
using the total neuropathy score (TNS), the Medical Research
Council (MRC) scale, hand grip strength measurements, fine
motor activity, coordinative function, and balance tests. To
assess symptoms of chemotherapy-induced peripheral neu-
ropathy, the quality of life questionnaire of the European
Organization for Research and Treatment of Cancer
(EORTC) was used (QLQ-CIPN20). Patients were available
for a neurological follow-up examination after a period of
approximately 3 months. In parallel, blood samples were
collected for serum creatine kinase (CK) measurement and
immunological investigations including testing for autoanti-
bodies (Ab) (ANA profile, ANCA-IFT, myositis profile,
AChR Ab) and determination of lymphocyte subpopulations
by flow cytometry. The antinuclear antibodies (ANA) were
detected by immunofluorescence and by immunoblotting.
Statistical analysis
For individual values, we selected the median and the range.
Continuous data are given as the mean with the standard
deviation (SD). Variations in data between the different groups
were tested either by a two-tailed unpaired t test or a Mann-
Whitney U test using the SPSS 11.5 program (SPSS Inc.,
Chicago, IL, USA).
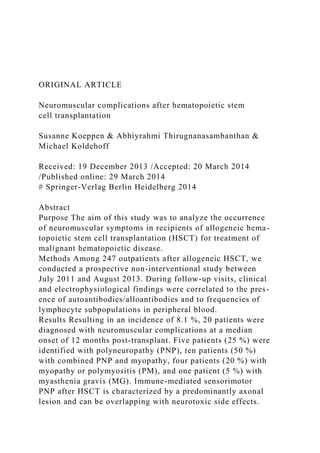
Results
Twenty patients presented with neuromuscular complications
after allogeneic HSCT resulting in an incidence of 8.1 %.
Patient characteristics and laboratory findings are summarized
in the Table 1. The mean age of the patients was 50 years (49.9
6. ±9.6 years, range 27–64). The median interval between first
evaluation and follow-up examination was 3 months. Due to
GvHD, all patients received immunosuppressive treatment
consisting of a calcineurin inhibitor and low-dose steroid
medication. The median time from transplant to the onset of
neuropathic symptoms was 12 months (range 2–120). The
latency between HSCT and development of PM varied be-
tween 60 days and 72 months. The most commonly reported
motor symptoms were weakness in 65 % and muscle cramps
in 55 % of the patients. The most frequent sensory symptoms
were paresthesia (60 %) and numbness (45 %). The major
clinical sign on neurologic examination was an impaired
vibration sense detected in 70 % of the patients. The mean
TNS score (range 0–36) was 8.97±4.5, the mean MRC sum
score (range 0–60) was 54.3±7.9, and the mean value of the
hand grip strength was 16.98±6.9 kp at baseline. Five patients
(25 %) were identified with PNP, ten patients (50 %) with
combined PNP and myopathy, four patients (20 %) with
myopathy or PM, and one patient (5 %) with MG.
2338 Support Care Cancer (2014) 22:2337–2341
T
ab
le
1
P
at
ie
n
t
ch
51. )
–
0
.6
5,
1
.2
Support Care Cancer (2014) 22:2337–2341 2339
Electrophysiological testing including nerve conduction stud-
ies and electromyography, if possible, revealed an axonal
motor neuropathy of the peroneal nerve in 12 patients and a
sural nerve axonopathy in 6 patients. The maximum CK
serum concentration observed was 475 U/l. Ab were detected
in 12 patients, myositis-specific Ab only in one patient. Nine-
teen patients had hematopoietic full chimerism, and one pa-
tient had mixed chimerism. At the time of onset of neuromus-
cular symptoms, a coincidence with a decrease of CD4 T cells
and increase of CD8 T cells was observed in 17 and 12
patients, respectively.
Discussion
Improved survival of patients undergoing allogeneic HSCT
shifts the focus of neurologic involvement towards long-term
sequelae. Because of different new conditioning protocols of
allogeneic HSCT and immunosuppression, the nature of neu-
rologic complications has changed over time. In this study,
post-HSCT PNP in combination with myopathy appeared to
be more common than isolated myopathy or peripheral neu-
ropathy. Prior to the onset of PM, the immunosuppressive
medication had been tapered in all patients. PM following
52. HSCT has been reported to occur in approximately 3.4–
7.7 % of patients usually along with other manifestations of
GvHD [15]. In general, the onset is insidious, although it can
be acute especially after donor lymphocyte infusion (DLI)
[16]. Typical clinical features of PM are proximal bilateral
limb weakness and muscle atrophy, similar to idiopathic PM
[17]. The presence of Ab may correlate with the severity of
chronic GvHD [18]. In most cases, GvHD-related PM shows
a prompt treatment response to corticosteroids and cyclospor-
ine resulting in complete and sustained remission [19]. Nor-
mal or slightly elevated serum CK-levels in our patients are
compatible with clinical stability described in most cases.
Myositis-specific Ab were found in only one patient. This is
corresponding to previous reports [20]. MG has been de-
scribed as rare manifestation of chronic GvHD in the late
post-HSCT phase [21, 22]. However, circulating Ab directed
against muscle acetylcholine receptor (AChR Ab) are detect-
able in about 20 % of patients with chronic GvHD [23]. In our
patient with MG following HSCT, the onset of clinically overt
MG was associated with elevated AChR Ab and titin Ab. It is
noteworthy that titin Ab in the context of post-HSCT MG
have not been reported before. A considerable number of
patients in the present study complained of neuropathic symp-
toms correlated with other GvHD manifestations. However,
the pathogenesis of peripheral neuropathies following alloge-
neic HSCT is often multifactorial [24, 25]. Compared to prior
studies, the onset of PNP after HSCT showed a higher vari-
ability in our patients. Electrophysiological studies revealed a
predominantly axonal lesion of the peripheral nervous system
and chronic neurogenic or myogenic changes of the affected
muscles. None of our patients met the diagnostic criteria for
chronic inflammatory demyelinating polyneuropathy (CIDP).
The majority of patients were in stable clinical condition
during the observation period. Accordingly, laboratory testing
gave only little evidence of disease activity. Immunosuppres-
53. sive treatment was continued. However, our study has some
limitations. First, patients were not neurologically evaluated
prior to HSCT. Therefore, chemotherapy-induced PNP under-
lying a later developing GvHD-related affection of the periph-
eral nervous system cannot be excluded despite negative
history of neuropathic symptoms prior to HSCT. Second,
steroid myopathy might be a contributing factor of the motor
deficit in some patients because corticosteroids are the first-
line therapy of GvHD. In a retrospective analysis of patients
with acute myeloid leukemia or myelodysplastic syndrome
treated with high-dose steroid for acute GvHD following
allogeneic HSCT, steroid myopathy was identified in 41 %
of the patients [26]. Third, the small number of patients and
lack of a control group requires confirmation of the results in a
larger controlled prospective study. Despite these limitations,
it can be concluded from the results of this study based on the
partly longitudinal character of neurological evaluation that
the neuromuscular system seems to be affected more frequent-
ly than reported so far in patients with GvHD after allogeneic
HSCT. The immunological findings suggest that sequential
analyses of lymphocyte subpopulations in peripheral blood
might be helpful during the immunosuppressive dose reduc-
tion period in order to prevent GvHD-related clinical deterio-
ration. However, only further research studies can determine
whether it is possible to prevent those complications by
adapting the immunosuppressive regimen based on the lym-
phocyte subpopulation findings in the peripheral blood.
Conflict of interest The authors declare no conflict of interest.
They
also state that they have full control of primary data and that
they agree to
allow the journal to review their data if requested.
References
54. 1. de Brabander C, Cornelissen J, Smitt PA, Vecht CJ, van den
Bent MJ
(2000) Increased incidence of neurological complications in
patients
receiving an allogenic bone marrow transplantation from
alternative
donors. J Neurol Neurosurg Psychiatry 68(1):36–40, Epub
1999/12/
22
2. Teive HA, Funke V, Bitencourt MA, de Oliveira MM, Bonfim
C,
Zanis-Neto J et al (2008) Neurological complications of
hematopoi-
etic stem cell transplantation (HSCT): a retrospective study in a
HSCT center in Brazil. Arquivos de neuro-psiquiatria
66(3B):685–
690, Epub 2008/10/25
3. Uckan D, Cetin M, Yigitkanli I, Tezcan I, Tuncer M,
Karasimav D
et al (2005) Life-threatening neurological complications after
bone
marrow transplantation in children. Bone Marrow Transplant
35(1):
71–76, Epub 2004/11/09
2340 Support Care Cancer (2014) 22:2337–2341
4. Kotani A, Ishikawa T, Matsumura Y, Ichinohe T, Ohno H,
Hori Tet al
(2001) Correlation of peripheral blood OX40+(CD134+) Tcells
with
chronic graft-versus-host disease in patients who underwent
55. alloge-
neic hematopoietic stem cell transplantation. Blood
98(10):3162–
3164, Epub 2001/11/08
5. Jaglowski SM, Devine SM (2014) Graft-versus-host disease:
why
have we not made more progress? Curr Opin Hematol
21(2):141–
147, Epub 2014/01/29
6. Delios AM, Rosenblum M, Jakubowski AA, DeAngelis LM
(2012)
Central and peripheral nervous system immune mediated
demyelin-
ating disease after allogeneic hemopoietic stem cell
transplantation
for hematologic disease. J Neuro-Oncol 110(2):251–256, Epub
2012/08/24
7. Sostak P, Padovan CS, Yousry TA, Ledderose G, Kolb HJ,
Straube A
(2003) Prospective evaluation of neurological complications
after
allogeneic bone marrow transplantation. Neurology 60(5):842–
848,
Epub 2003/03/12
8. Ahn JS, Cho SH, Kim YK, Yang DH, Bae WK, Shim HJ et al
(2009)
Polymyositis and myocarditis after donor lymphocyte infusion.
Int J
Hematol 90(1):113–116, Epub 2009/05/28
9. Allen JA, Greenberg SA, Amato AA (2009) Dermatomyositis-
like
56. muscle pathology in patients with chronic graft-versus-host
disease.
Muscle Nerve 40(4):643–647, Epub 2009/08/12
10. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard
JR, Lee SJ
et al (2005) National Institutes of Health consensus
development
project on criteria for clinical trials in chronic graft-versus-host
dis-
ease: I. Diagnosis and staging working group report. Biol Blood
Marrow Transplant J Am Soc Blood Marrow Transplant 11(12):
945–956, Epub 2005/12/13
11. Antonini G, Ceschin V, Morino S, Fiorelli M, Gragnani F,
Mengarelli
A et al (1998) Early neurologic complications following
allogeneic
bone marrow transplant for leukemia: a prospective study.
Neurology
50(5):1441–1445, Epub 1998/05/22
12. Couriel DR, Beguelin GZ, Giralt S, De Lima M, Hosing C,
Kharfan-
Dabaja MA et al (2002) Chronic graft-versus-host disease
manifest-
ing as polymyositis: an uncommon presentation. Bone Marrow
Transplant 30(8):543–546, Epub 2002/10/16
13. Dowell JE, Moots PL, Stein RS (1999) Myasthenia gravis
after
allogeneic bone marrow transplantation for lymphoblastic
lympho-
ma. Bone Marrow Transplant 24(12):1359–1361, Epub
2000/01/11
57. 14. Openshaw H (1997) Peripheral neuropathy after bone
marrow trans-
plantation. Biology of blood and marrow transplantation. J Am
Soc
Blood Marrow Transplant 3(4):202–209, Epub 1997/11/14
15. Lin PC, Hsiao LT, Chen PM (2005) Acute polymyositis
after donor
lymphocyte infusion. Eur J Haematol 74(2):166–168, Epub
2005/01/
19
16. Montoro J, Hernandez-Boluda JC, Arbona C, Solano C
(2012)
Polymyositis after donor lymphocyte infusion. Int J Hematol
96(3):
386–389, Epub 2012/08/21
17. Liu FC, Chen CH, Chao TY (2007) Polymyositis complicat-
ing donor lymphocyte infusion after stem cell transplantation
for relapsed chronic myeloid leukemia: report of a case and
review of literature. Clin Rheumatol 26(7):1207–1210, Epub
2006/08/29
18. Wechalekar A, Cranfield T, Sinclair D, Ganzckowski M
(2005)
Occurrence of autoantibodies in chronic graft vs. host disease
after
allogeneic stem cell transplantation. Clin Lab Haematol
27(4):247–
249, Epub 2005/07/29
19. Maillard-Lefebvre H, Morell-Dubois S, Lambert M,
Charlanne
H, Launay D, Hachulla E et al (2010) Graft-versus-host
disease-related polymyositis. Clin Rheumatol 29(4):431–433,
58. Epub 2010/01/14
20. Stevens AM, Sullivan KM, Nelson JL (2003) Polymyositis
as a
manifestation of chronic graft-versus-host disease.
Rheumatology
(Oxford) 42(1):34–39, Epub 2003/01/02
21. Mackey JR, Desai S, Larratt L, Cwik V, Nabholtz JM (1997)
Myasthenia gravis in association with allogeneic bone marrow
trans-
plantation: clinical observations, therapeutic implications and
review
of literature. Bone Marrow Transplant 19(9):939–942, Epub
1997/05/01
22. Tse S, Saunders EF, Silverman E, Vajsar J, Becker L,
Meaney B
(1999) Myasthenia gravis and polymyositis as manifestations of
chronic graft-versus-host-disease. Bone Marrow Transplant
23(4):
397–399, Epub 1999/04/01
23. Kotani A, Takahashi A, Koga H, Morita R, Fukuyama H,
Ichinohe T
et al (2002) Myasthenia gravis after allogeneic bone marrow
trans-
plantation treated with mycophenolate mofetil monitored by
periph-
eral blood OX40+ CD4+ T cells. Eur J Haematol 69(5–6):318–
320,
Epub 2002/12/04
24. Nagashima T, Sato F, Chuma T, Mano Y, Sasaki I, Mori M
et al (2002) Chronic demyelinating polyneuropathy in graft-
versus-host disease following allogeneic bone marrow trans-
59. plantation. Neuropathol Off J Jpn Soc Neuropathol 22(1):1–8,
Epub 2002/05/28
25. Rabinstein AA, Dispenzieri A, Micallef IN, Inwards DJ,
Litzow MR,
Wijdicks EF (2003) Acute neuropathies after peripheral blood
stem
cell and bone marrow transplantation. Muscle Nerve 28(6):733–
736,
Epub 2003/11/26
26. Lee HJ, Oran B, Saliba RM, Couriel DM, Shin K, Massey P
et al
(2006) Steroid myopathy in patients with acute graft-versus-
host
disease treated with high-dose steroid therapy. Bone Marrow
Transplant 38(4):299–303, Epub 2006/07/05
Support Care Cancer (2014) 22:2337–2341 2341
Copyright of Supportive Care in Cancer is the property of
Springer Science & Business
Media B.V. and its content may not be copied or emailed to
multiple sites or posted to a
listserv without the copyright holder's express written
permission. However, users may print,
download, or email articles for individual use.
Neuromuscular complications after hematopoietic stem cell
transplantationAbstractAbstractAbstractAbstractAbstractIntrodu
ctionMethodsStatistical analysisResultsDiscussionReferences
Literature Search Chart – Quantitative or Qualitative Research
Studies
(may also use for Mixed Methods or Outcomes Studies)
60. Also attach article as PDF to assignment
Reference
1 pt
1 pt
Reference listed in correct APA format
PDF of article uploaded to Canvas assignment
Type of Research
1 pt
Accurately identify whether quantitative (non-experimental),
quantitative (experimental) or qualitative
Quantitative: Non-experimental
Quantitative - Experimental
Qualitative
Design/ Method
2 pts
1 pt
1 pt
· Describe method (e.g., longitudinal, cohort, pre-test/post-test,
retrospective chart review, interview, focus group)
· Describe whether researcher had comparison groups and how
they differed
· Describe time frame (e.g. baseline data, follow-up at x
months)
·
Sample & Setting
1 pt
1 pt
1 pt
61. 1 pt
· Population studied: demographic variables
· Inclusion criteria
· How sample is chosen
· Setting of study
·
Major Variables & Measurements
2 pts
2 pts
· Describe the variables studied (quantitative) or the general
content of questions (qualitative)
· For each variable, list the specific survey/tool/measurement
(quantitative) or how are data collected and analyzed
(qualitative)
·
Findings
1 pt
4 pts
· In your own words
· Describe the key findings of the study, specifically detailing
results, such as % of subjects who experienced a certain result;
discuss whether results were statistically significant
(quantitative) or describe/define the major themes of the study
including details about what the themes mean and any sub-
themes (qualitative)
·
Appraisal: Applicability to PICOT
2 pts
· Describe how and to what extent this study contributes to
answering your PICOT question – such as – Does it have a
similar population? Does it answer your question? Does it
support or not support your intervention?
·
62. Appraisal: Study Rigor
1 pt
1 pt
1 pt
· Discuss issues related to validity or reliability, including study
design, researcher bias, subject selection, etc.
· State whether you believe the study was sufficient to answer
the researcher’s questions in terms of: Design, number of
subjects, variables, etc. (quantitative) or Your determination of
whether the analysis of data and themes was sufficient and
whether it aligned with philosophy for this type of study
(qualitative)
· Why did you state the study was sufficient or not sufficient?
·
$75,000 in Sales & Property Taxes
$60,000 in Homeowner Property Taxes
$600,000 in Homeowner Housing Expense Saved
$1,100,000 Paid to Local Trade Contractors & Suppliers
$45,000 in Permit and Professional Fees
$60,000 in Local Purchases /other misc
$700,000 in Wages Paid (Fiscal Year)
$1,100,000 in ReStore Sales of Donated & Recycled Goods
$500,000 in Volunteer Wage Benefit
63. Generated per year in Citrus County
Page 1
Habitat for Humanity of Citrus County, Inc
Website: Link
Wikipedia: Link
Our Mission
https://www.habitatcc.org/mission.php
VISION
A world where everyone has a decent place to live.
MISSION STATEMENT
Seeking to put God's love into action, Habitat for Humanity
brings people together to build homes, communities and hope.
HABITAT FOR HUMANITY OF CITRUS COUNTY MISSION
STATEMENT
Habitat for Humanity of Citrus County is a nonprofit,
ecumenical Christian housing ministry who seeks to put God's
love into action by bringing people together to build homes,
neighborhoods and hope. We work to eliminate substandard
housing for people of all backgrounds, races and religions by
providing simple, decent, affordable housing to those who have
a need, ability to pay and willingness to partner.
Driven by the vision that everyone needs a decent place to live,
HFHCC was founded in 1993. Since then, HFHCC has increased
the number of houses we build each year in Inverness, Crystal
River, Homosassa and Hernando. Blessed with the support of
benefactors, churches, businesses, civic organizations and
others, we celebrated our 25th year with the completion of 175
homes. To date we have completed construction on 175 homes.
Habitat for Humanity is not a charity or a give-away program.
Partner families pay a small down payment and maintain a no-
interest mortgage. They also invest hundreds of hours of labor—
sweat equity—into building their own homes and the homes of
others. Through financial support, volunteering or adding a
64. voice to support affordable housing, everyone can help families
achieve the strength, stability and self-reliance they need to
build better lives for themselves. Partner families work
alongside generous Habitat volunteers who donate time, skills
and energy to help build the houses.
We are people from different faiths, diverse backgrounds and
many economic levels. We work toward a common goal,
honoring the dignity of each person by helping each one secure
a safe, secure and decent place to live.
NON-PROSELYTIZING POLICY
"As a matter of policy, Habitat for Humanity International and
its affiliated organizations do not proselytize. This means that
Habitat will not offer assistance on the expressed or implied
condition that people must either adhere to or convert to a
particular faith, or listen and respond to messaging designed to
induce conversion to a particular faith".
Our Villagehttps://www.habitatcc.org/our_village.php
Habitat for Humanity of Citrus County, Inc., is pleased to share
our story about Southern Pines Village in Inverness, Florida
located in Citrus County. The team at Habitat envisioned a
deed restricted Habitat village in our county to bring people
together in a neighborhood setting. Historically, Habitat for
Humanity's construction lots have been scattered throughout the
county, mainly as a result of donor gifts. Southern Pines is the
first time that the Citrus County affiliate has had the
opportunity to create its own deed restricted village in Citrus
County Florida.
Southern Pines Village is a 33 single family community for
qualified families earning under 80% Area Medium Income.
Today 24 families reside in Southern Pines Village in Inverness
Florida and the remaining 9 will take residence in early 2019.
The homes are on quarter-acre lots and include paved streets
and city water.
The development is located on S. Apopka Avenue and is only a
few blocks from Downtown Inverness. This subdivision is close
to shopping, dining and many healthcare facilities along
65. Highland Boulevard, including Citrus Memorial Hospital.
Home Ownership Requirements
https://www.habitatcc.org/director_message.php
Basic Requirements
• You must have lived or worked in Citrus County for the past
12 months.
• You must be a US Citizen or Permanent Resident.
• If married, you must apply with your spouse.
• You must wait 2 years after foreclosure or bankruptcy has
been finalized.
Family Selection Criteria
A volunteer Selection Committee consisting of Citrus County
citizens considers applications based on the following criteria:
Need:
• You do not already own a home.
• You are currently living in substandard housing, which would
include any of the following conditions:
- Home is in poor physical condition.
- Home is overcrowded.
- Rent is subsidized.
- Rent is more than 30% of income.
• Your household gross income is between 35% and 80% of the
area median income.
Income Eligibility (effective 05/14/2019)
Annual Gross Income Guidelines for Consideration of
HFHCC Partnership for Homeownership
Family Size
Min. Income
Max. Income
1
$14,814.00
$29,550.00
2
$14,814.00
$33,750.00
66. 3
$14,814.00
$37,950.00
4
$15,814.00
$42,150.00
5
$17,100.00
$45,550.00
6
$18,360.00
$48,900.00
7
$19,620.00
$52,300.00
8
$20,880.00
$55,650.00
Ability to pay
• You have proof of at least 1 year of steady, verifiable, annual
income.
• You do not have any judgments or liens against you.
• You do not have excessive debt or multiple accounts in
collection.
• You pay your rent on time.
Willingness to partner with Habitat
• Contribute 500 hours of sweat equity hours.
• Attend Habitat homeowner training classes.
• Pay $2,000 towards closing costs.
Sweat Equity
Sweat equity is the single most important strategy Habitat uses
to empower future homeowner families (partner families) and
one of the features that sets us apart from other affordable
housing providers.
Habitat uses the term “sweat equity” to refer to the hours of
67. labor our homeowners dedicate to building their homes and the
homes of their neighbors, as well as the time they spend
investing in their own self-improvement. Habitat for Humanity
of Citrus County partner families begin their sweat equity after
being accepted into the program, and they must complete a
minimum of 500 hours before they can move into their homes.
Sweat equity reduces the amount of paid labor needed for a
house, which in turn helps reduce cost. Additionally, time spent
building their own homes instills a sense of pride and
ownership, teaching the basic building and house-maintenance
skills that are necessary for home ownership.
Most importantly, by going beyond a mere financial investment
in their property and performing sweat equity alongside other
volunteers and neighbors, Habitat homeowners gain a greater
sense of self-worth and become more personally invested in
their community.
How To Apply
***APPLICATION PERIOD IS NOW ***OPEN***. PLEASE
SEE THE LATEST NEWS ON OUR HOME PAGE FOR
DETAILS REGARDING HOME OWNERSHIP INFORMATION
SESSIONS AND ORIENTATIONS***
The first step toward homeownership is by attending a
Homeowner Orientation Session. Call Family Services at 352-
563-2744 or visit our office at 7768 W. Gulf to Lake Hwy,
Crystal River, FL 34429 to find out when the next orientation
is.
Frequently Asked Questions
Are Habitat for Humanity homes FREE?
No. All Habitat for Humanity homeowners pay a small amount
of closing costs when they have completed the program and all
Habitat for Humanity homeowners will pay a monthly mortgage
loan payment until the home is paid in full, usually after 20 to
30 years. One of the benefits of having a Habitat for Humanity
home mortgage in Citrus County, Florida, is that our mortgage
loans are 0% interest. Paying no interest on a home mortgage
saves our homeowners hundreds of thousands of dollars over the
68. life of their loan compared to getting a mortgage elsewhere.
Why aren't the home free? I thought habitat homes were
built with donated money, materials and volunteer labor.
Some land is donated, some land Habitat for Humanity must
buy. A few materials are donated to every home build; the rest
Habitat for Humanity must buy. Some labor is volunteered; but
some things only licensed & insured professional contractors
such as electricians, plumbers, heating & cooling installers, and
roofers must do. Cash donations and grants help pay for some of
the costs, and selling the donations of gently used items at our
ReStore helps pay for the rest. Habitat for Humanity could not
exist without the generosity of our donors & volunteers. Our
homeowners also play an important part in building more
homes: as each new homeowner pays back the cost of building
their home, they provide more money to Habitat for Humanity
so that we can build more homes.
Are Habitat for Humanity homes available for rent?
No. Habitat for Humanity of Citrus County does not rent homes.
Does Habitat for Humanity provide emergency housing/shelter?
No. We recommend you contact your local Red Cross or United
Way for emergency housing.
When and where are the Home Ownership Information Sessions
held?
Typically, we hold "How to Become a Habitat Homeowner"
oreintation quarterly. We will announce in the local paper, local
radio station, on our website and our Facebook page when we
will be holding the next homeowner orientation session.
Who can help with my sweat equity hours?
Each Partner Family must contribute a total of 500 "Sweat
Equity" hours prior to the sale of the home to the family. The
Partner Family must complete 250 hours before they are in line
for a home, and the Partner Family must contribute 100 hours
themselves toward the construction of their house. If the Partner
Family includes 2 adults, a total of 200 hours out of the 500
hours must be completed by the Partner Family themselves, and
the remaining 300 hours may be contributed by extended family
69. & friends. When there is only 1 adult in the Partner Family, a
total of 100 hours out of the 500 hours must be completed by
the Partner Family themselves, so 400 hours may be contributed
by extended family & friends. Children in the Partner Family
must be at least 18 years old to contribute sweat equity hours on
the construction site, 16 years old for the Habitat ReStores and
at least 10 years old and accompanied by a parent for sod
lays. However, younger Partner Family children are also able to
contribute sweat equity hours by earning good grades in school.
I know nothing about building a home. How am I going to be
able to help on a job site?
At each job site we have a Construction Director and/or a Site
Supervisor who will instruct you in what needs to be done.
Every job is important, even the cleanup. You will learn
important skills for the upkeep of your home as well.
Will I immediately be able to move into my house when my
hours and classes are complete?
Home availability depends on the building schedule. You may
have to wait for your home to be built. First your home is
completed, an appraisal is performed, and a Certificate of
Occupancy must be issued by the local building inspector's
office, and you can get a homeowners' insurance quote. Then we
can begin the paperwork for closing on the sale of your home to
you. This paperwork will take about 1 month to complete.
Usually our homeowners are able to move into their homes on
the day of (or shortly after) their closing paperwork is signed.
The keys to the home are given to the homeowner(s) at their
home dedication.
If I tell you how much money I make, can you tell me if I
qualify for a Habitat house?
No. Your income is only part of the qualification process. First,
we can NOT take any income information by telephone. You
should only provide your income information when you submit
a written application during our open enrollment periods.
Second, Our Family Selection Committee reviews your entire
completed application and performs a home visit to see your
70. current living conditions in order to decide if you will qualify
for our Home Ownership Program. We Income Guidelines
posted on our website, which you can review. The minimum and
maximum income shown is based on the number of people who
will live in your home.
If I tell you how much money I make, can you tell me how
much my house payment with Habitat would be?
No. First, we can NOT take any income information by
telephone. You should only provide your income information at
your scheduled application appointment. Second, when you
become a homeowner, part of your monthly payment is based on
how much your homeowners' insurance premium will be, and
how much your property taxes will be. We do not know how
much either of those things will cost until the home is built and
the completed home is appraised. Finally, while your income is
part of how much your payment will be, we also look at your
debts and other financial matters as well as your household size
when reviewing your application to see how much you can
afford. We want each of our homeowners to be successful when
repaying the mortgage on their home.
Changing Lives...One Family at a Time
By Rose Strawn, Family Services Director, Habitat for
Humanity of Citrus County, Inc.
We would like to begin this story of our Habitat Mission
by defining our purpose. “We seek to put God’s love into
action, by bringing people together to build homes, communities
and hope! We do so, through the dreams of our Partner
Families, who are striving to improve their lives with
determination, with assistance, in the form of a “hand up, not a
hand out”, from our Construction, Family Services, ReStores
and our Administrative Teams, as well as, numerous Habitat
Volunteers and Donors, in the many facets of our operation.
Ultimately, achieving the “American Dream” of
Homeownership!
Looking back, we do so with a real sense of accomplishment
with nearly 180 families achieving Homeownership in
71. partnership with our Habitat Affiliate. These homes were
completed through our fiscal year ending in June 2019.
Presently, we are working on completing homes in our Southern
Pines Village in Inverness, as well as permitting new homes in
the North Highlands area in Inverness. In our not too distant
future, we envision the development of villages in our newly
acquired Citrus Springs area!
As those of us either working with or volunteering with our
Habitat Affiliate look forward to what our future holds, please
be mindful of the following scripture: Roman’s 8:28: ….and
we know that in all things GOD works for the good for those
who love HIM, who have been called according to HIS
purpose”!!
God Bless and Keep, as we thank you for helping us further
our Habitat Mission!!! Rose Strawn/Family Services
Director
Minimum two paragraphs per question.
1. Summarize the organization's purposes, functions and sources
of funding. Include the
organization's impact if applicable (for example: number of
low-income clients served,
number of units built, etc.)
2. Political or geographic boundaries of area focused on during
this specific contact:
72. 3. Community Profile: Current economic conditions; current
demographic characteristics;
general banking and credit needs; other (e.g. Identifying names
of low or moderate income
neighborhoods).
4. Opportunities for participation by local financial institutions:
Community development,
other credit-related projects, or financing programs; level of
opportunity for bank
involvement.
5. Performance of local financial institutions: Perceptions or
experience regarding the
degree of involvement of the local financial institution industry
and of the specific financial
institution (if obtained) in the community.