
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Renal failure-in-pregnancy1
Similar to Renal failure-in-pregnancy1 (20)
More from ahmed afify
More from ahmed afify (14)
Recently uploaded
Recently uploaded (20)
Renal failure-in-pregnancy1
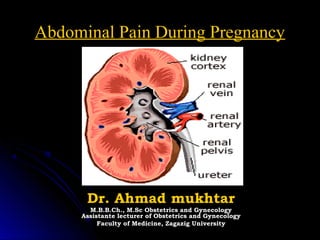
- 1. Abdominal Pain During PregnancyAbdominal Pain During Pregnancy Dr. Ahmad mukhtarDr. Ahmad mukhtar M.B.B.Ch., M.Sc Obstetrics and GynecologyM.B.B.Ch., M.Sc Obstetrics and Gynecology Assistante lecturer of Obstetrics and GynecologyAssistante lecturer of Obstetrics and Gynecology Faculty of Medicine, Zagazig UniversityFaculty of Medicine, Zagazig University
- 2. Introduction Abdominal pain in pregnancy is a common complaint. It’s management represents a challenge to the clinician because the causes may be due to pregnancy or may be related to pregnancy but not directly due to it or may be unrelated to pregnancy at all.
- 3. CAUSES OF ABDOMINAL PAIN DURING PREGNANCY (A) Pregnancy Related Pain: • Early pregnancy o Abortion: Inevitable, incomplete or septic abortions o Vesicular mole: when expulsion starts. o Ectopic pregnancy: pain precedes bleeding. • Later pregnancy o Braxton-Hicks Contraction o Round Ligament Pain o Pressure symptoms o Cholestasis of pregnancy o Placental abruption o Placenta percreta o Acute Fatty Liver o Pre-eclampsia , HELLP o Spontaneous rupture of the liver o Uterine rupture o Chorioamnionitis o Acute Polyhydramnios o Labor ( Term , Preterm ) (B)Conditions associated with pregnancy • Rupture of rectus abdominus muscle • Torsion of the pregnant uterus • Acute urinary retention due to retroverted gravid uterus MusculoSkeletal ( Pubic Symphysis pain-sacroiliac – back pain ) Red degeneration of myoma Torsion of pedunculated myoma Ovarian cyst rupture Adnexal torsion • © Non-Pregnancy Related Pain • Gastrointestinal o Acute appendicitis o Peptic ulcer o Gastroenteritis o Hepatitis o Inflammatory Bowel Complication (Crohn’s &Ulcerative Colitis ) o Bowel obstruction o Bowel perforation o Herniation o Meckel diverticulitis o Toxic megacolon o Pancreatic pseudocyst HepatoBliary o Biliary Stones o Acute Hepatitis o Acute Cholecystitis o Acute pancreatitis • Genitourinary o Ureteral calculus o Acute pyelonephritis o Acute cystitis o Rupture of renal pelvis o Ureteral obstruction • Vascular o Superior mesenteric artery syndrome o Thrombosis/infarction - Specifically mesenteric venous thrombosis o Ruptured visceral artery aneurysm • Respiratory o Pneumonia • Other o Intraperitoneal hemorrhage o Splenic rupture o Abdominal trauma o Acute intermittent porphyria o Diabetic ketoacidosis o Sickle cell disease
- 5. The incidence of the different causes of abdominal pain in pregnancy is difficult to estimate . The is because classifying this symptom into pregnancy & non-pregnancy symptom related is often not possible until after delivery.
- 6. Pain directly related to pregnancy;- First trimesterFirst trimester Abortion Hydatidiform mole Ectopic pregnancy The pain is colicky in nature felt in the lower abdomen or pelvis commonly associated with commonly associated with amenorrhoea and vaginal bleeding In threatened & missed abortions there may be mild or no pain Diagnosis by BHCG,exam & USS
- 7. .Molar pregnancy Incidence is 1 in 1200 pregnancies Pain when present is due to the uterus trying to expel the molar tissue (colicky) When severe may suggest intra-peritoneal bleeding Uterus large for date ,watery blood stained discharge USS shows snow – storm appearance .
- 8. . Ectopic pregnancy Incidence is 1 in 100 pregnancies in UK Presents with pain & amenorrhoea The pain is commonly in one of the iliac fossa and may be referred to the tip of the shoulder Most of cases are diagnosed by BHCG,TVS and/or laparoscopy.
- 9. . Second trimester * Abortion* * Acute urinary retention in association with incarcerated* retroverted gravid uterus typically at 12-14 weeks * Chorioamnionitis following PROM* * Retroplacental haemorrhage following amniocentesis* * Round ligament pain due to stretch classically at 18-22 wks * Red degeneration of the fibroid
- 10. Incarcerated retroverted graved uterus Commonly occurs between 12-14wks Causes urethral obstruction with acute urinary retention & pain Indwelling urine cathter helps allow the uterus to become abdominal
- 11. . Retroplacental haemorrhage following amniocentesis Can complicate both diagnostic & therapeutic amniocentesis especially when the needle inserted transplacentally Pain is felt a few hours after after the procedure Constant & localised to the puncture site
- 12. Round ligament pain Occurs secondary to stretching of the ligament as the uterus enlarges into the abdomen (10-30% of pregnancy) Commonly occurs in the late 1stst and early 2and trimester Felt as dragging, stabbing or cramp-like pain in the outer lower abdomen radiating to groin Diagnosis is made by excluding other other causes .
- 13. . Red degeneration of fibroid Occurs due to infarction of the centre of the fibroid during mid – pregnancy The fibroid suddenly enlarges & is painful and tender The pain is ischaemic ,constant, and localised to one side of the uterus but sometimes diffuse. Mild pyrexia leucocytosis. USS may be helpful Treatment is conservative Third Trimester
- 14. 17. Fetal movements & Braxton-Hicks contractions These are spontaneous uterine contractions becoming more frequent as pregnanc. advances.
- 15. Initially painless but then perceived as vague backache which is minimally uncomfortable but does not need analgesia, however can be sever requiring hospital admission commonly in primigravida.
- 16. Placental abruption Presents with abdominal pain or vaginal bleeding or without vaginal bleeding Complicates up to 1% of pregnancies Abdominal pain could be mild constant or intermittent (like labour pains) When no vaginal bleeding, can be confused with other causes of abdominal pain.
- 17. Sever Pre-eclampsia & eclampsia Incidence about 6% among primigravida about 6% among primigravidae Pain is mainly at the epigastrium & Rt upper quadrantquadrant It’s due to stretching of the liver capsuleIt’s secondary to subcapsular haemorrhage Other symptoms & signs are often present Treatment involves control & delivery.
- 18. 20. Uterine rupture Unlikely to occur silently during pregnancy but it can occur in women with previous classical C/S usually from early 3rdrd trimester. Others occur in labour in women who had Others c/s or perforated uterus during D/C The abdominal pain typically acute, , associated with shock & shoulder tip pain Laparotomy is required after resuscitblock.
- 19. Pain not directly related to pregnancy 22. Gastrointestinal TractGastrointestinal Tract 23. Gastro-esophagealGastro-esophageal refluxreflux A common cause of upper abdominalA common cause of upper abdominal pain in pregnancy. Incidence 60- 70%pain in pregnancy. Incidence 60-70% More common in late pregnancyMore common in late pregnancy multiple pregnancy & polyhydramniosmultiple pregnancy & polyhydramnios Felt as burning sensation inFelt as burning sensation in epigastrium & behind the sternumepigastrium & behind the sternum Caused by relaxation of gastro-Caused by relaxation of gastro- esophageal sphincteresophageal sphincter
- 20. Peptic ulcerPeptic ulcer Uncommon during pregnancyUncommon during pregnancy Usually there is a pre-existing historyUsually there is a pre-existing history Pain typically in the epigasric & RtPain typically in the epigasric & Rt hypochodrium worse with hunger & spicyhypochodrium worse with hunger & spicy foodfood Perforation is rare but may occur especiallyPerforation is rare but may occur especially after delivery. Presents with acute painafter delivery. Presents with acute pain ,collapse & peritonitis,collapse & peritonitis Gas under diaphragm on erect x-ray abdomGas under diaphragm on erect x-ray abdom
- 21. . Hiatus herniaHiatus hernia Incidence 7-22% of all pregnanciesIncidence 7-22% of all pregnancies Present in 62% of cases of severPresent in 62% of cases of sever heartburn in the 3heartburn in the 3rdrd trimestertrimester Very severe cases present with severVery severe cases present with sever vomiting & haematemesisvomiting & haematemesis Treatment as for reflux esophagitisTreatment as for reflux esophagitis 26. constipationconstipation May present as sever or chronicMay present as sever or chronic abdominal painabdominal pain Caused by slow peristalsisCaused by slow peristalsis (progeterone effect)(progeterone effect) Felt as dull, constant & sometimesFelt as dull, constant & sometimes colicky pain in the iliac fossae (Ltcolicky pain in the iliac fossae (Lt Treatment with high fibre diet &Treatment with high fibre diet & laxativeslaxatives
- 22. 27. Acute appendicitisAcute appendicitis Complicates 1 in 1500-2500Complicates 1 in 1500-2500 pregnancies (as in non- pregnants)pregnancies (as in non-pregnants) Symptoms & signs may be atypical.Symptoms & signs may be atypical. Pain may be in the Rt lumber region inPain may be in the Rt lumber region in early gestation or in the Rtearly gestation or in the Rt hypochondrium in late pregnancy duehypochondrium in late pregnancy due to displacement of caecum & appedixto displacement of caecum & appedix by the gravid uterusby the gravid uterus
- 23. The pain in early pregnancy startsThe pain in early pregnancy starts around the umbilicus then settles inaround the umbilicus then settles in the RIFthe RIF Accompanied by nausea, vomitingAccompanied by nausea, vomiting anorexia & fever however, theseanorexia & fever however, these symptoms may be absent in latesymptoms may be absent in late pregnancypregnancy 29. Leucocytosis is an important sign butLeucocytosis is an important sign but due to physiological leucocytosis indue to physiological leucocytosis in pregnancy, serial count is more usefulpregnancy, serial count is more useful Pyrexia, tenderness & guarding overPyrexia, tenderness & guarding over the Rt abdomen may be the only signsthe Rt abdomen may be the only signs presentpresent The inflammed appendix may induceThe inflammed appendix may induce preterm labourpreterm labour 30. Treatment of acute appendicitisTreatment of acute appendicitis In early pregnancy laparoscopicIn early pregnancy laparoscopic appendectomy can be done or throughappendectomy can be done or through the classical McBurney incisionthe classical McBurney incision If laparotomy is necessary, a para-If laparotomy is necessary, a para- median incision over the area of maxmedian incision over the area of max tenderness allows the best access iftenderness allows the best access if extension is neededextension is needed 31. Complications of appendicitis inComplications of appendicitis in pregnancypregnancy RuptureRupture Peritonitis: organ displacementPeritonitis: organ displacement prevents walling- off of the inflammedprevents walling- off of the inflammed appendixappendix PROM & preterm labourPROM & preterm labour
- 24. . Bowel obstructionBowel obstruction Is a rare cause of acute abdominalIs a rare cause of acute abdominal pain in pregnancy (1 in 2500-3500 )pain in pregnancy (1 in 2500-3500 ) Incidence appears to be increasingIncidence appears to be increasing due to increased abdomino –pelvicdue to increased abdomino –pelvic surgery causing adhesion bandssurgery causing adhesion bands Rarely caused by strangulated femoralRarely caused by strangulated femoral or inguinal herniae & volvulus.or inguinal herniae & volvulus. 33. Bowel obstruction ..contBowel obstruction ..cont The pain is colicky with exaggerated bowelThe pain is colicky with exaggerated bowel sounds & constipation. Abdominalsounds & constipation. Abdominal distension may be difficult to detect indistension may be difficult to detect in advanced pregnancyadvanced pregnancy Treatment is conservative with N/S tubing,Treatment is conservative with N/S tubing, fluid & electrolyte replacementfluid & electrolyte replacement it usually settle within few hours otherwiseit usually settle within few hours otherwise laparotomy is required to divide adhesionslaparotomy is required to divide adhesions
- 25. . Gallstones &Gallstones & cholecystitischolecystitis Pregnancy predisposes to gallstonesPregnancy predisposes to gallstones due to biliary stasis and raiseddue to biliary stasis and raised cholesterol in pregnancycholesterol in pregnancy Incidence about 3.5%Incidence about 3.5% Most women are asymptomaticMost women are asymptomatic Symptomatic Pt’s present with suddenSymptomatic Pt’s present with sudden onset of colicky abdominal painonset of colicky abdominal pain radiating to the back in Rt hypochodriuradiating to the back in Rt hypochodriu 35. Gallbladder ..contGallbladder ..cont Nausea, vomiting & vasovagal attacksNausea, vomiting & vasovagal attacks Tenderness & positive murphy’s signTenderness & positive murphy’s sign may be the only positive clinical signsmay be the only positive clinical signs Diagnosis can be made by ultrasoundDiagnosis can be made by ultrasound Treatment is coservativeTreatment is coservative Surgery can be performed in earlySurgery can be performed in early pregnancy laparoscopicallypregnancy laparoscopically 36. Gallbladder..contGallbladder..cont Open surgery can be done inOpen surgery can be done in advanced pregnancy but risks areadvanced pregnancy but risks are ascending cholangitis which may leadascending cholangitis which may lead to septicaemia & preterm labourto septicaemia & preterm labour 37. Gallbladder..contGallbladder..cont Acute cholecystitis is uncommon inAcute cholecystitis is uncommon in pregnancypregnancy Presents with acute Rt hypochonderialPresents with acute Rt hypochonderial pain, nausea, vomiting & pyrexiapain, nausea, vomiting & pyrexia Pyrexia differentiating it from gallstonePyrexia differentiating it from gallstone Incidence 1 in 1000 pregnanciesIncidence 1 in 1000 pregnancies Treatment with antibiotics & analgesiaTreatment with antibiotics & analgesia 38. pancreatitispancreatitis Uncommon in pregnancy (1 in 5000)Uncommon in pregnancy (1 in 5000) More common in pregnants than nonMore common in pregnants than non High mortality rate (>10%)High mortality rate (>10%) Presents with central or upperPresents with central or upper abdominal pain radiating to the backabdominal pain radiating to the back There may be nausea, vomiting &There may be nausea, vomiting & shock. Few with juandice when thereshock. Few with juandice when there is obstructed biliary systemis obstructed biliary system 39. Pancreatitis.. contPancreatitis.. cont Diagnosis confirmed by raised serumDiagnosis confirmed by raised serum amylaseamylase Ultrasound shows gallstones in 50% ofUltrasound shows gallstones in 50% of casescases Treatment is conservative with iv fluidTreatment is conservative with iv fluid & electrolyte replacement, pethidine,& electrolyte replacement, pethidine, steroids, antibiotics cimitidine &steroids, antibiotics cimitidine & glucgoneglucgone 40. Renal tractRenal tract 41. Acute pyelonephritisAcute pyelonephritis Is the most common renal cause ofIs the most common renal cause of abdominal pain in pregnancy (1-2%)abdominal pain in pregnancy (1-2%) Most cases present in the 2Most cases present in the 2ndnd & 3& 3rdrd trimesters with sever abdominal paintrimesters with sever abdominal pain in the lumbar region radiating to thein the lumbar region radiating to the iliac fossa or vulvailiac fossa or vulva Nausea, vomiting, pyrexia, rigors &Nausea, vomiting, pyrexia, rigors & tachycardia with loin tendernesstachycardia with loin tenderness
- 26. . Pyelonephritis..contPyelonephritis..cont Associated with increased risk ofAssociated with increased risk of preterm labourpreterm labour Diagnosis by MSU for R/E & C/SDiagnosis by MSU for R/E & C/S E. Coli is the most common causeE. Coli is the most common cause If recurrent exclude renal anomaliesIf recurrent exclude renal anomalies USS during preg. Or IVP 3-4 monthsUSS during preg. Or IVP 3-4 months after delivery.after delivery. 43. Renal stonesRenal stones Affects 0.03-0.05% of pregnant women (asAffects 0.03-0.05% of pregnant women (as in non-pregnants)in non-pregnants) Pregnancy does not predispose to stonePregnancy does not predispose to stone formation . In fact small stones may passedformation . In fact small stones may passed unnoticed due to ureteric dilatationunnoticed due to ureteric dilatation Presents with loin pain radiating to thePresents with loin pain radiating to the suprapubic region the pain may besuprapubic region the pain may be excruciating & associated with shockexcruciating & associated with shock 44. Renal stones...contRenal stones...cont Renal tenderness may be the only clinicalRenal tenderness may be the only clinical sign USS may show dilated renal tract or asign USS may show dilated renal tract or a stonestone Treatment mostly conservative with potentTreatment mostly conservative with potent analgesic & liberal fluid intakeanalgesic & liberal fluid intake If obstruction persist surgery is indicatedIf obstruction persist surgery is indicated There is a risk of precipitating pretermThere is a risk of precipitating preterm labourlabour 45. Acute retention of urineAcute retention of urine More likely to occur in the 1More likely to occur in the 1stst trimestertrimester and in the puerperium.and in the puerperium. Causes include:Causes include: - incarcerated R/v gravid uterus- incarcerated R/v gravid uterus - pelvic mass (ovarian or fibroid)- pelvic mass (ovarian or fibroid) - acute herpes infection- acute herpes infection - vulval haematoma- vulval haematoma 46. Urine retention..contUrine retention..cont Presents with sudden onset of severPresents with sudden onset of sever pain with distended bladder on exampain with distended bladder on exam Catherterization for 24-48hrs &Catherterization for 24-48hrs & analgesia are very helpful and allowanalgesia are very helpful and allow the gravid uterus to becomethe gravid uterus to become abdominalabdominal 47. Adenxal accidentsAdenxal accidents Corpus luteum cyst in early pregnancy mayCorpus luteum cyst in early pregnancy may bleed causing pain or rupture causing shockbleed causing pain or rupture causing shock Mostly diagnosed by USS or bimanually ifMostly diagnosed by USS or bimanually if they are largethey are large Managed mostly conservatively but if theyManaged mostly conservatively but if they are large or showing abnormal pathologyare large or showing abnormal pathology they should be removed after 14 wksthey should be removed after 14 wks 48. Adenxal accidents..contAdenxal accidents..cont Torsion of a pre-existing ovarian cystTorsion of a pre-existing ovarian cyst (benign or malignant) presents with(benign or malignant) presents with intermittent abdominal pain which laterintermittent abdominal pain which later becomes constant (indicatingbecomes constant (indicating ischaemia). There may be nausea,ischaemia). There may be nausea, vomiting, low grade fever andvomiting, low grade fever and leucocytosis .If ignored the ovary mayleucocytosis .If ignored the ovary may become gangrenousbecome gangrenous 49. Adnexal accidents..contAdnexal accidents..cont Laparotomy with oophorectomy orLaparotomy with oophorectomy or fixing the ovary if viablefixing the ovary if viable Torsion of a pedunculated fibroid mayTorsion of a pedunculated fibroid may present in a similar way to tortedpresent in a similar way to torted ovarian cyst. They need to beovarian cyst. They need to be removed at laparotomy. Don’t try toremoved at laparotomy. Don’t try to remove subserous, intramural fibroidremove subserous, intramural fibroid as it may end by hysterectomyas it may end by hysterectomy 50. Miscellaneous causeMiscellaneous cause Musculoskeletal :Musculoskeletal : - exaggerated lumbar lordosis- exaggerated lumbar lordosis - sumphyseal diasthesis- sumphyseal diasthesis * sickle cell crisis* sickle cell crisis * rectus sheath haematoma* rectus sheath haematoma * porphyria* porphyria * Aortic aneurysm* Aortic aneurysm Recommended Strategic Planning Fundamentals Time Management Fundamentals
- 27. Renal DisordersRenal Disorders Pathogenesis:- 75-90% due to E coli, probably derived from large bowel Colonization of urinary tract results from ascending infection from the perineum and is related to sexual intercourse.
- 28. DiagnosisDiagnosis Most women with asymptomatic bacteriuria are found to be infected during early pregnancy and very few subsequently acquire asymptomatic bacteriuria Bacteriuria is only considered significant if the colony count exceeds 100,000/ml on a MSU
- 29. ManagementManagement The choice of antibiotic depends on culture/sensitivity Ampicillin, amoxicillin, Augmentin and the cephalosporin are safe and appropriate antibiotics in pregnancy. Treatment should be continued for 2 weeks in the first instance and regular urinary culture required.
- 30. Risks: pyelonephritis, preterm birth, low birth weight, increased perinatal mortality
- 31. Acute CystitisAcute Cystitis Acute cystitis:-inflammation of the bladder {bacterial or nonbacterial causes (eg, radiation or viral infection)}. Cystitis complicates 1% of pregnancies Clinical features:- Urinary frequency, dysuria, haemeturia and suprapubic pain Diagnosis Significant bacteriuria on MSU
- 32. Acute CystitisAcute Cystitis Management:- Same as asymptomatic bacteriuria Several non-pharmacological maneuvers may help to prevent recurrent infection in women with recurrent urinary-tract infections in pregnancy. These include: Increase fluid intake Emptying the bladder following sexual intercourse
- 33. Acute PyelonephritisAcute Pyelonephritis Incidence :- This complicates 1-2% of pregnancies More common in pregnancy ( physiological dilatation of the upper renal tract).
- 34. Epidemiology:- UTIs in women: 14 times more frequent than in men. 1. The urethra is shorter 2. lower 1/3 of the urethra is continually contaminated with pathogens from the vagina and the rectum 3. Women tend not to empty their bladders as completely as men do 4. Urogenital system is exposed to bacteria during intercourse .
- 35. Hormonal and mechanical changes:- urinary stasis and vesicoureteral reflux urinary stasis {progesterone-induced ureteral smooth muscle relaxation}. urinary retention {weight of the enlarging uterus} Loss of ureteral tone combined with increased urinary tract volume. urinary stasis: dilatation of the ureters, renal pelvis, and calyces. more common on right side (86% of cases) Glycosuria and aminoaciduria.
- 36. Etiology :- E coli : most common cause of UTI, 80- 90% originates from fecal flora colonizing the periurethral area: ascending infection. Other pathogens: Klebsiella pneumoniae (5%) Proteus mirabilis (5%) Enterobacter species (3%) Staphylococcus saprophyticus (2%) Group B beta-hemolytic Streptococcus (GBS; 1%) Proteus species (2%)
- 37. Acute PyelonephritisAcute Pyelonephritis Clinical Features :- Fever, Loin and abdominal pain, Vomiting, Rigors Proteinuria, Haematuria. Risk increases in women:- On steroid therapy With polycystic kidneys Congenital abnormalities of renal tract Urinary-tract calculi Diabetes
- 38. Acute PyelonephritisAcute Pyelonephritis Diagnosis Significant bacteriuria on MSU specimen. Differential diagnosis:- Pneumonia Viral infections Cholecystitis , biliary colic Acute appendicitis Gastroenteritis, Placental abruption Degenerating uterine fibroid. Blood cultures and a full blood count is recommended
- 39. Complications :- IUGR Preeclampsia preterm delivery. acute cystitis maternal anemia, and amnionitis.
- 40. Other complications: 1. Perinephric cellulitis and abscess, Septic shock (rare) 2. Renal dysfunction. 4. Pulmonary injury: 2% Endotoxins that alter alveolar-capillary membrane permeability are produced; subsequently, pulmonary edema and acute respiratory distress syndrome develop.
- 41. Acute PyelonephritisAcute Pyelonephritis Management:- Should be after hospitalization I/V Antibiotic Penicillin and cephalosporin are the Ist choice.
- 42. Chronic Renal DiseaseChronic Renal Disease Pregnancy with Chronic Renal Disease Effects of Pregnancy The risks include: Accelerated decline in renal function Rising hypertension Worsening proteinuria Effects of chronic renal disease on pregnancy The risks includes: Miscarriage Pre-eclampsia Intrauterine growth retardation Preterm delivery Fetal death
- 43. Chronic Renal DiseaseChronic Renal Disease Factors Influencing Outcome The presence and degree of renal impairment The presence and severity of proteinuria The underlying type of chronic renal disease
- 44. Chronic Renal DiseaseChronic Renal Disease Degree of Renal Impairment:- Mild renal impairment (plasma creatinine <125 umol/I) Moderate renal impairment (plasma creatinine 125-250 umol/I) Severe renal impairment (plasma creatinine >250 umol/I)
- 45. Chronic Renal DiseaseChronic Renal Disease In general, women without hypertension or renal impairment prior to conception have successful pregnancies, and pregnancy does not adversely influence the progression of the renal disease.
- 46. Specific Types of RenalSpecific Types of Renal DiseaseDisease Glomerulonephritis Reflux nephropathy Diabetic nephropathy SLE nephritis Polycystic kidney disease (PKD)
- 47. Chronic Renal DiseaseChronic Renal Disease Women with chronic renal disease should be managed jointly by obstetricians and physicians Preconceptual assessment of renal functions and blood pressure should be made. In view of the increased risk of pre-eclampsia, treatment with low dose aspirin should be considered especially in those with hypertension, renal impairment or a previous poor obstetric history. Careful monitoring and control of blood pressure both prepregnancy and antenatally is important.
- 48. Specific Types of Renal DiseaseSpecific Types of Renal Disease The fetus should be monitored with regular ultrasound assessment of growth and Doppler assessment of uterine and umbilical circulation. Admission should be considered if the woman develops worsening hypertension, deteriorating renal function or proteinuria, or superimposed eclampsia.
- 49. Acute Renal FailureAcute Renal Failure Incidence :- Rare in pregnancy <0.005% Clinical Features Anuria/oliguria urea, creatinine rises Decreased GFR Causes Infection Septic abortion Puerperal sepsis Rarely acute pyelonephritis Blood Loss Postpartum hemorrhage Abruption
- 50. Acute Renal FailureAcute Renal Failure Causes Infection :- Septic abortion Puerperal sepsis Rarely acute pyelonephritis Blood Loss:- Postpartum hemorrhage. Abruption Volume Contraction Pre-eclampsia Eclampsia (6%) Hypermesis gravidarum Post-renal Failure Ureteric damage or obstruction HELLP Syndrome 7% have actual renal failure Thrombotic thrombocytopenic purura/hemolytic uraemic syndrome (TTP/HUS)
- 51. Idiopathic postpartum renalIdiopathic postpartum renal failurefailure Associated primarily withAssociated primarily with microangiopathic processesmicroangiopathic processes Postpartum hemolytic-uremic syndrome.Postpartum hemolytic-uremic syndrome. These were often irreversible and wereThese were often irreversible and were associated with substantial mortality.associated with substantial mortality. Now improved outcome with plasmaNow improved outcome with plasma exchange,dialysis,prostacyclin infusion,exchange,dialysis,prostacyclin infusion, correcting coagulopathycorrecting coagulopathy 5151Dr Mona ShroffDr Mona Shroff
- 52. DialysisDialysis pregnancy on dialysis is unusual: end-stagepregnancy on dialysis is unusual: end-stage renal failure reduces fertility.renal failure reduces fertility. Patients on dialysis should be advised not toPatients on dialysis should be advised not to get pregnant.get pregnant. Common risks: anaemia and haemorrhage.Common risks: anaemia and haemorrhage. Increased risks of:Increased risks of: miscarriage, fetal death, pre-eclampsia, pre-miscarriage, fetal death, pre-eclampsia, pre- term labour, PROM, polyhydramnios andterm labour, PROM, polyhydramnios and placental abruption.placental abruption. Pregnant women require increasing dialysis toPregnant women require increasing dialysis to maintain the pre-dialysis urea < 15-20 mmol/l.maintain the pre-dialysis urea < 15-20 mmol/l. Poor obstetric outcome is similar with bothPoor obstetric outcome is similar with both haemodialysis and peritoneal dialysis.haemodialysis and peritoneal dialysis.
- 53. Indications for KidneyIndications for Kidney Replacement TherapyReplacement Therapy Acidosis unresponsive to medical therapyAcidosis unresponsive to medical therapy Acute, severe, refractory electrolyteAcute, severe, refractory electrolyte changes (e.g., hyperkalemia)changes (e.g., hyperkalemia) EncephalopathyEncephalopathy Significant azotemia (blood urea nitrogenSignificant azotemia (blood urea nitrogen level >100 mg per dL [36 mmol per L])level >100 mg per dL [36 mmol per L]) Significant bleedingSignificant bleeding Uremic pericarditisUremic pericarditis Volume overloadVolume overload 5353Dr Mona ShroffDr Mona Shroff
- 54. Hemodialysis Vs PeritonealHemodialysis Vs Peritoneal dialysisdialysis Limited usefulnessLimited usefulness if hypotensionif hypotension C/I in activelyC/I in actively bleeding pt.bleeding pt. ControlledControlled anticoagulation reqdanticoagulation reqd Volume shifts-Volume shifts- carefulcareful Faster correctionFaster correction Can be used inCan be used in preg/PP pt.preg/PP pt. Easily availableEasily available Simple,inexpensiveSimple,inexpensive Lower Cx rateLower Cx rate Minimises rapidMinimises rapid metabolicmetabolic pertubations & fluidpertubations & fluid shiftsshifts Insert cath highInsert cath high direct visiondirect vision 5454Dr Mona ShroffDr Mona Shroff
- 55. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Women receiving renal transplants should be warned that as renal function returns to normal, ovulation, menstruation and fertility also resume. Women desiring pregnancy are usually advised to wait about 1-2 years after transplantation.
- 56. Guidelines for pregnancy in kidney:- transplant recipient Two years post-transplant, with good general health and serum creatinine less than 2.0 mg/dL (preferably <1.5 mg/dL(. No recent or ongoing rejection . Normotension, or minimal antihypertensives Absent or minimal proteinuria. No evidence of pelvicalyceal dilation on renal ultrasonogram
- 57. Immunosuppression Prednisone - Less than 15 mg per day Azathioprine - Less than or equal to 2 mg/kg/d Calcineurin inhibitor–based therapy - Therapeutic levels Mycophenolate mofetil and sirolimus - Discontinue 6 weeks prior to conception
- 58. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Complication Risks Immunosuppressive agents increase the risk of hypertension during pregnancy. Preeclampsia occurs in approximately one-third of transplant recipients. Almost 50% of pregnancies in these women end in preterm delivery due to hypertension Blood levels of calcineurin inhibitors need to be frequently monitored due to changes in volumes of distribution of extracellular volume. There is an increased risk of infection included cytomegalovirus, toxoplasmosis, and herpes infections, and bacterial infection which arouse concern for the fetus.
- 59. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Effects of pregnancy on renal transplants:- Pregnancy probably has no adverse long- term effect Renal allograft adapt to pregnancy About 15% of women develop significant impairment About 40% develop proteinuria towards term. Effect of renal transplants on pregnancy:- The chance of successful outcome is >90%, but this is reduced to 70% if complications occur before 28 weeks’ gestation. The complication rate is higher for diabetics.
- 60. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Recommended :- Antenatal Management;-Women should be managed jointly by nephrologists and obstetricians with expertise in the care of pregnant renal transplant recipients. Careful monitoring and control of blood pressure is important. Regular assessment of RFTs by creatinine clearance and 24 hour protein excretion,
- 61. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients as well as serum creatinine and urea is essential. a full blood count, LFTs should also be checked regularly. Anemia is common and haematinics should be prescribed. The fetus should be monitored with regular ultrasound assessment of growth and Doppler assessment of uterine Sand umbilical circulation.
- 62. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Immunosuppressive Therapy:- The doses of immunosuppressive drugs are maintained at prepregnancy Levels which should preferably be: Prednisolone, <15 mg/day plus either Azathioprine, <2 mg/kg/day Cyclosporin A, 2-4 mg/kg/day
- 63. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Delivery :- Caesarean section is only required for obstetric indications. Prophylactic antibiotics should be given to cover any surgical procedure including episiotomy. Parental steroids are necessary to cover labour, as with any woman on maintenance steroids.
- 64. Pregnancy in Renal TransplantPregnancy in Renal Transplant RecipientsRecipients Neonatal Problems These are largely related to prematurely but also include the following: Thymic atrophy Transient leukopenia or thrombocytopenia Depressed haemopoiesis