
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Current Trends in Management of Gastroesophageal Reflux Disease
Similar to Current Trends in Management of Gastroesophageal Reflux Disease (20)
Recently uploaded
Recently uploaded (20)
Current Trends in Management of Gastroesophageal Reflux Disease
- 2. Prevalence of GERD 18-46% 7.4% 22%21% 16%18% Russia South America North Europe South Europe South Asia Southeast Asia Gut. 2018 Mar;67(3):430-440.
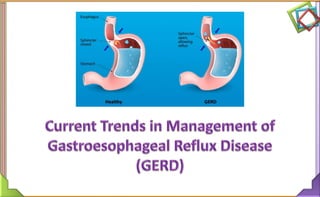
- 3. Gastroesophageal Reflux • Gastroesophageal reflux – Normal physiologic phenomenon experienced intermittently by most people, particularly after a meal • Gastroesophageal reflux disease (GERD) – Amount of gastric juice that refluxes into the esophagus exceeds the normal limit, causing symptoms with or without associated esophageal mucosal injury
- 4. GERD-Definition Am J Gastroenterol 2013;108:308-328 “Symptoms or complications resulting from the reflux of gastric contents into the esophagus or beyond, into the oral cavity (including larynx) or lung”
- 6. Pathophysiology of GERD Abnormal lower esophageal sphincter Functional (frequent transient LES relaxation) Mechanical (hypotensive LES) Foods (Coffee, alcohol) Medications (Calcium channel blockers) Increase abdominal pressure Obesity Pregnancy Increased gastric volume
- 7. Clinical Manifestations • Heartburn • Regurgitation • Hypersalivation • Nausea/Vomiting • Bloating/Belching • Cough/Wheezing • Dysphagia/Odynophagia • Weight loss • Digestive hemorrhage Typical Atypical Alarming J Clin Gastroenterol. 2017 Jul;51(6):467-478.
- 8. Phenotypic Presentations of GERD GI Motility online (2006) doi:10.1038/gimo42
- 9. GERD Phenotype-Association 1. Nonerosive Reflux Disease vs. Erosive Esophagitis NERD may progress to EE in approximately 10% of GERD patients EE is a manifestation of more severe reflux disease 2. Erosive Esophagitis vs. Barrett’s esophagus EE is a major risk factor for BE EE patients have 5-fold increased risk of BE if GERD is not controlled in 5 years compared to patients who are free of GERD in 5 years 1. Curr Treat Options Gastroenterol. 2007;10:294–304. 2. Am J Gastroenterol. 2011;106:1946–1952.
- 10. Nonerosive reflux disease (NERD) Troublesome reflux-related symptoms without esophageal mucosal erosions/breaks at conventional endoscopy No Erosion Parameter Characteristic of NERD as compared to EE Gender More female Age Younger Weight Leaner Symptom duration Shorter Motility abnormalities Slightly increased Distal esophageal acid exposure (total, supine, and erect) Mildly increased Duodenogastroesophageal reflux Slightly increased GI Motility online (2006) doi:10.1038/gimo42
- 11. Erosive Esophagitis Erosive esophagitis (EE) Esophageal mucosal erosive changes/recurrent, reflux, regurgitant, peptic and marginal esophagitis
- 12. Barrett’s esophagus (BE) • Premalignant condition – Squamous epithelium of the distal esophagus is replaced by an abnormal columnar epithelium known as specialized intestinal metaplasia • Risk Factors – Male Sex, Age (older than 50 years of age) – Prolonged GERD symptoms (O5 years) – Family history of BE and/or adenocarcinoma of the esophagus – Nocturnal reflux symptoms, hiatal hernia – Increased body mass index (BMI R25 kg/ m2), Intra-abdominal distribution of fat Barrett’s esophagus (BE) Gastrointest Endosc. 2015;81(6):1305-10.
- 14. Diagnostic test Indication Recommendation Empirical PPI therapy (“PPI trial”) Classic symptoms, no alarm features, extraesophageal GERD A negative trial does not rule out GERD Urea breath test or Helicobacter pylori stool antigen test For uninvestigated dyspepsia & high (>20%) H. pylori prevalent area Subject to local cost-benefit Considerations, should be based on noninvasive test (UBT, monoclonal stool antigen test) Endoscopy For alarm symptoms screening of high-risk patients, chest pain, Differentiates EE from NERD, Diagnoses other causes or upper gut symptoms Consider early for elderly, those at risk for BE, noncardiac chest pain patients unresponsive to PPI, prompt endoscopy is recommended in areas with high incidence of upper GI cancer pH or impedance pH monitoring For atypical symptoms, For PPI- refractory GERD, Preoperatively, for nonerosive disease Correlate symptoms with reflux, document abnormal acid exposure or reflux frequency J Clin Gastroenterol. 2017 Jul;51(6):467-478.
- 16. Management of GERD Gut Liver. 2018 Jan 15;12(1):7-16.
- 17. Proton Pump Inhibitors - GERD
- 18. Mechanisms acid secretion 18 Histamine (H2) Gastrin Acetylcholine (M3) Activates the acid-secreting pump Proton pump Final common step
- 19. 19
- 20. 2013 ACG-Recommendations Am J Gastroenterol 2013;108:308-328
- 21. Management of GERD-Non Medical 1. Weight loss Patients with overweight or have had recent weight gain Conditional recommendation, MLOE 2. Head of bed elevation and avoidance of meals 2 – 3 h before bedtime for nocturnal GERD patients Conditional recommendation, LLOE 3. Routine global elimination of food that can trigger reflux not recommended Eg. Chocolate, caffeine, alcohol, acidic and / or spicy foods Conditional recommendation, LLOE Am J Gastroenterol 2013;108:308-328 HLOE: High Level of Evidence, MLOE: moderate level of evidence, LLOE: Low Level of Evidence
- 22. Management of GERD-PPIs 4. 8-week course of PPIs Therapy of choice for symptom relief and healing of erosive esophagitis Strong recommendation, HLOE 5. PPIs should be initiated at OD dosing, before first meal of the day Strong recommendation, MLOE 6. Traditional delayed release PPIs should be administered 30 – 60 min before meal for maximal pH control Strong recommendation, MLOE Am J Gastroenterol 2013;108:308-328
- 23. Management of GERD-PPIs 7. For patients with partial response to once daily therapy, adjust dose timing and/or BID dosing should be considered in patients with Night-time symptoms, variable schedules, and / or sleep disturbance Strong recommendation, LLOE 8. Maintenance PPI therapy should be administered for GERD patients Who continue to have symptoms after PPI is discontinued Patients with complications including EE & BE Strong recommendation, MLOE 9. Non-responders to PPI should be referred for evaluation Conditional recommendation, LLOE Am J Gastroenterol 2013;108:308-328
- 24. Management of GERD-Other agents 10. H2 -receptor antagonist (H2 RA) can be used as a maintenance option in patients without EE if patients experience heartburn relief Conditional recommendation, MLOE 11. Therapy for GERD other than acid suppression Prokinetic therapy, baclofen Should not be used in GERD patients without diagnostic evaluation Conditional recommendation, MLOE 12. There is no role for sucralfate in the non-pregnant GERD patient Conditional recommendation, MLOE Am J Gastroenterol 2013;108:308-328
- 25. World Gastroenterology Organization Global Guidelines GERD Global Perspective on Gastroesophageal Reflux Disease J Clin Gastroenterol. 2017 Jul;51(6):467-478
- 26. Management of GERD: Level of Resources - Medium Therapy Non-medical 1. Lifestyle modifications (diet, weight loss) 2. Locally available symptomatic remedies if they are safe, effective, and less costly than prescription medications Medical acid-suppression therapy 1. Alginate-antacid (AA) 2. Histamine 2 receptor antagonists (H2RA) 3. Proton pump inhibitors (PPI) OD BID Recommendation: 1. Stop after 8wk to assess response; Resume, as needed, at lowest effective dose (Intermittent/on demand) 2. Continue for, frequent symptoms, stricture, BE (to control Symptoms) 3. Consider H. pylori “test-and-treat” for continuous PPI therapy J Clin Gastroenterol. 2017 Jul;51(6):467-478.
- 27. Management of GERD-PPIs: Level of resources – Medium & High Therapy 1. PPI OD 8-12 wk, then reassess 2. PPI BID 8-12 wk for persistent symptoms 3. Switch PPIs to a modified-release PPI (effect lasting >14h/d, MR-PPI) if available (OD or BID) 1. MR-PPI OD for 8 to 12 wk, then reassess 2. MR-PPI BID for 8 to 12wk for persistent symptoms 3. More frequent PPI therapy if incomplete response symptomatically & on pH monitoring Added Recommendation: 1. Laparoscopic antireflux surgery for structural disease (hiatus hernia) or volume reflux causing regurgitation, aspiration, stricture, or persistent nocturnal symptoms despite PPI BID J Clin Gastroenterol. 2017 Jul;51(6):467-478.MR: Modified-release (Delayed, Sustain release)
- 28. Recommendation on Helicobacter pylori Infection • In high prevalent countries consider H. Pylori assessment in management & treatment of upper GI symptoms before empirical antireflux therapy, to discriminate between symptoms of GERD, peptic ulcer disease, and functional symptoms • H. pylori status has no effect on symptom severity, recurrence, or treatment efficacy in GERD • Indeed, in patients with H. pylori-positive uninvestigated dyspepsia, eradication therapy is associated with a lower prevalence of reflux- like symptoms (36%) than control therapy (49%) J Clin Gastroenterol. 2017 Jul;51(6):467-478.
- 29. Management of GERD-Pregnancy J Clin Gastroenterol. 2017 Jul;51(6):467-478.
- 30. 2013 ACG vs. 2017 WGO Guidelines Particular ACG WGO Weight loss Recommended Recommended PPI use 8 weeks 8-12 weeks PPI partial response Increase dose Increase dose Delayed release PPI For EE & BE Recommended Recommended PPI refractoriness Consider evaluation Secondary care (Gastroenterologist, Surgeon) Use of other therapy Moderately recommended Recommended for short to medium term PPI Continuous therapy & H. Pylori test Not recommended Test & Treat recommended in high prevalent country
- 31. Proton pump inhibitors in GERD
- 32. Proton Pump Inhibitors-Pharmacokinetic Parameters Ome Esome Lanso Pantoprazole Bioavailability (%) 30-40 64 80 77 Factors affecting absorption Food Food Antacids, food none Elimination t1/2 0.7 0.9 1.2 1.2 Half-life of recovery of acid secretion < 30 h - <15h 46 h Linear PK no no yes yes Interaction with CYP 450 Inhibits CYP2C19 Inhibits CYP2C19 Inhibits CYP2C19 none
- 33. Efficacy of Different PPIs
- 34. Acid suppression by different Proton pump inhibitors
- 35. Gastric & Duodenal Ulcer Healing Rate Complete ulcer healing significantly higher in Pantoprazole users than Omeprazole & Ranitidine 58 77 87 0 50 100 Ranitidine Omeprazole Pantoprazole Cumulative ulcer healing rate (% patients) at 4 weeks Drugs 1996 Mar;51(3):460-82 Patients randomly administered Pantoprazole 40mg OD, Ranitidine 150 mg BID & Omeprazole 20mg OD 52 76 65 89 71 95 50 60 70 80 90 100 2 weeks 4 weeks Ranitidine Omeprazole Pantoprazole Cumulative ulcer healing rate (% patients)
- 36. Pantoprazole produces significantly more symptom- and heartburn- free days/nights as compared to Ranitidine Aliment Pharmacol Ther 2004; 20: 567-75 58 83 73 92 50 100 Sympton - free days Heartburn free days Ranitidine Pantoprazole 349 GERD patients Intervention: Pantoprazole 10,20 or 40 mg OD or Ranitidine 150 mg BD Duration: 1 year PPI vs. H2RA in Erosive Esophagitis
- 37. Pantoprazole offers superior action in GERD with 22% & 15% faster symptomatic relief in wk 2 & wk 4 47 65 69 80 40 45 50 55 60 65 70 75 80 85 Week 2 Week 4 %ofpatientwithrelief Rantidine Pantoprazole Digestion . 2001; 63 (3): 163 – 70 277 GERD patients Intervention: Pantoprazole 20 OD or Ranitidine 150mg BD Assessment: Primary criterion was relief from heartburn, acid eructation & pain in swallowing Comparison of pantoprazole 20 mg to ranitidine 150 mg b.i.d. in the treatment of mild gastroesophageal reflux disease
- 38. Pantoprazole versus omeprazole in the treatment of reflux esophagitis 76% 95% 71% 93% 0% 20% 40% 60% 80% 100% 4 weeks 8 weeks HealingRates 60 Patients: Pantoprazole 40/day & 60 Patients: Omeprazole 20 mg/day Pantoprazole Omeprazole Acta Med Croatica. 1999;53(2):79-82. Healing rate superior in Pantoprazole compared to omeprazole
- 39. Comparison of pantoprazole versus omeprazole in the treatment of acute duodenal ulceration—a multicentre study 96% 88% 89% 90% 91% 92% 93% 94% 95% 96% 97% 4 weeks Ratesofcompleteulcer healing 185 Patients: Pantoprazole 40 mg/day; 91 patients: Omeprazole 20 mg/day Pantoprazole Omeprazole Pantoprazole was shown to be a highly‐effective and well‐tolerated treatment for acute duodenal ulcer Aliment Pharmacol Ther. 1995 Aug;9(4):411-6.
- 40. Patients of GERD on Pantoprazole had a significantly lower risk of relapse and fewer symptom episodes 46 48 50 52 54 56 58 60 62 Esomeprazole Pantoprazole 61 51 % patients experiencing a symptomatic relapse 529 patients of GERD treated with 20mg Pantoprazole or 20 mg Esomeprazole over 4 weeks 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 Esomeprazole Pantoprazole 0.74 0.56 No. of symptom episodes Pantoprazole 40 mg is superior regarding the prevention of symptomatic relapse than esoeprazole Digestion. 2006;74(3-4):145-54
- 41. 0 2 4 6 8 10 12 14 Esomeprazole Pantoprazole 13 10 Median time to sustained symptom relief (in days) Median time to sustained symptom relief was 3 days shorter with Pantoprazole 529 patients of GERD treated with 20mg Pantoprazole or 20 mg Esomeprazole over 4 weeks Superior & Faster Sustained Symptom Relief Digestion. 2006;74(3-4):145-54
- 42. Summary 1. Weight loss is recommended for GERD management 2. PPIs are mainstay in the GERD management 3. In GERD persistent symptoms, dose modifications is advised 4. Modified release PPIs are recommended for long term management 5. PPI refractory patients needs re-evaluation/referred to specialist 6. In EE & BE continuous PPI therapy is required 7. 2017 WGO recommends H. pylori test to discriminate between GERD, functional symptoms, GI ulcer 8. Consideration to H. Pylori test is advised in continuous PPI users by 2017 WGO 9. Amongst several PPIs discussed, Pantoprazole appeared superior in efficacy
Editor's Notes
- https://www.nature.com/gimo/contents/pt1/full/gimo42.html#t2
- In the stomach, chief cells release pepsinogen. This zymogen is activated by hydrochloric acid (HCl), which is released from parietal cells in the stomach lining. The hormone gastrin and the vagus nerve trigger the release of both pepsinogen and HCl from the stomach lining when food is ingested.