Re-establishing autonomy in elderly frail patients.pdf

The Health Innovation Network Polypharmacy programme is working with healthcare professionals to address problematic polypharmacy by supporting easier identification of patients at potential risk from harm from multiple medications. Our evidence-based polypharmacy Action Learning Sets (ALS) are being rolled out across England to support GPs, pharmacists and other healthcare professionals who undertake prescribing or medication reviews to understand the complex issues around stopping inappropriate medicines safely. To drive and accelerate changes in practice, delegates complete a quality improvement project to address problematic polypharmacy in their workplace. This poster summary, Re-establishing autonomy in elderly frail patients, can be viewed here. For more information about the polypharmacy programme, please visit https://thehealthinnovationnetwork.co.uk/programmes/medicines/polypharmacy/
Recommended

Recommended
More Related Content
Similar to Re-establishing autonomy in elderly frail patients.pdf
Similar to Re-establishing autonomy in elderly frail patients.pdf (20)
More from Health Innovation Wessex
More from Health Innovation Wessex (20)
Recently uploaded
Recently uploaded (20)
Re-establishing autonomy in elderly frail patients.pdf
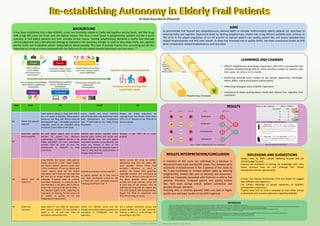
- 1. Re-establishing Autonomy in Elderly Frail Patients Dr Rute Rosa-Marsh (PharmD) Dr Rute Rosa-Marsh, PharmD ruterosa.marsh@dorsetgp.nhs.uk PDSA PLAN DO STUDY ACT #1 Elderly frail patients’ selection Select patients taking ≥1 drugs with ACB=3: Run a S1 report to populate >60yo patients taking any Ach drug with ACB=3 using the following ACB scale. 6 All eligible patients or respective carers to be contacted asking permission to participate in the study. Assess, classify and record individual patient frailty level using Rockwood Frailty Scale Questionnaire and Classification Tree. 7,8,9 Performed by the Frailty Clinical Pharmacist. Reduce the cohort population by selecting those with Clinical Frailty Score (CFS) ≥ 4 ≤7. Reassess as per PDSA #4 to assess progress. #2 Determine cognitive decline baseline Ask each eligible patient carer or family member to answer the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE)9: The same carer/family member must be used all time this questionnaire is answered to keep consistency. Establish each patient cognitive decline baseline score: Collect and record each patient IQCODE score and alert patient carer/family member to pay attention and record any changes in each of the questionnaire elements along the study, in order to keep accurate measurements of changes along the study. Reassess as per PDSA #4 to assess progress. #3 Reduce total AEC score to ≤2 Using PDSA#1 final cohort, invite patients (and/or carers) for a SMR. Obtain consent and discuss: patient concerns about their current medication; if they are coping with current regime; what are the patient preferences, and if there are any drugs they feel that are no longer needed and why. Investigate if patient takes all currently prescribed medication as indicated and if any medication is not taken, why is that so. Discuss the meaning of AEC and its effect in the individual quality of life, explaining the importance of reducing the AEC score and its relation to quality of life and independence improvement. Quantify each patient current total AEC: All eligible patients are to have each of their taken medications scored for AEC and total AEC score calculated using the following classification tool. 10 Switch current Ach drugs to another appropriate drug with the lowest AEC score possible. Always follow local formulary indications as much as possible, and respect NICE guidelines regarding initiation and monitoring all times. Aim to achieve a total AEC of 2 or less when possible. When planning multiple Ach drugs switches, switch one at each step of the process: start by switching the drug with the highest AEC first, when possible, safe and appropriate. Repeat this PDSA in conjunction with PDSA #4 according to results. #4 Determine outcomes Using PDSA #1 and PDSA #2 assessment tools, reassess patients CFS and IQCODE at weeks 4, 12, 24 post each PDSA #3 medication optimisation cycle. Collect CFS, IQCODE scores and AEC changes and analyse patients progress and correlation of CFS/IQCODE and AEC reductions. Run a patient satisfaction survey, and possibly publish the QI study outcomes. Develop a policy in anticholinergic de- prescribing for our PCN. BACKGROUND It has been established that a high ACB/AEC scores are intimately related to frailty and cognitive decline levels, and that drugs with a high AEC score are those with the highest impact. This issue is most found in polypharmacy patients and has a worse outcome in frail elderly patients due their complex clinical nature. Tackling polypharmacy demands a careful and thorough clinical judgement and a well-planned strategy to implement the necessary changes to avoid or slow down frailty and cognitive decline levels and re-establish patient independence where possible. This type of process is quite time consuming but still less expensive on a long run when compared with the daily cost of risks related hospital admissions and care plans. 1–6 AIMS To demonstrate that focused and comprehensively planned SMR’s in complex multimorbidity elderly patients can contribute to reducing frailty and cognitive impairment levels by tackling polypharmacy related risks using relevant available tools. Achieve an AEC of ≤2 in the subject population of our GP practice to improve patient care quality, patient QoL and reduce polypharmacy related hospitalisations and NHS costs overall. To show that investing time in quality SMR’s has lower economical burden to NHS when compared to related hospitalisations and care plans. People Communication Process Equipment Culture Environment No ACB/AEC check: Hospital Discharge/Consultant Letters Patient is seen by several medical professionals due to multimorbidity Clinical Professionals workload: Lack of time, funding, support, trained staff/experts Lack of awareness and knowledge about ACB/AEC polypharmacy consequences Communication challenges: Inter- professionals; Clinician-patient S1/EMIS/Ardens no automatic alert for ACB/AEC score ≥2 Local/National formularies/Guidelines Cognitive Impairment development Increased Frailty and Cognitive Impairment Levels REFLEXIONS AND SUGGESTIONS Always make my SMR’s patient wellbeing focused and not strictly budget focused; Improve self-confidence of sharing my knowledge with more senior clinicians than me and challenge their clinical therapeutical choices appropriately. Contact The Phoenix Partnership (TTP) and Ardens to suggest total ACB/AEC alert algorithm; Use Clinical Meetings to spread awareness of ACB/AEC consequences importance; Propose local CCG to fund a campaign to train other clinical professionals and increase awareness regarding ACB/AEC. RESULTS RESULTS INTERPRETATION/CONCLUSION A reduction of AEC score can contribute to a decrease in Rockwood Frailty Scale and IQCODE scores. This revealed some autonomy re-establishment in the 2 patients of this study so far. It also contributes to increase patient safety by reducing polypharmacy related risks such as dizziness and drowsiness, which are frequently associated with fractures in elderly frail patients. Therefore, increased patient care quality, patient QoL, NHS costs savings overall, patient satisfaction and possibly lifespan extension. Investing time in carefully planned SMR’s can lead to higher quality care and lower burden to the NHS in general. GP Nurse Rheumo Memory Clinic Urologist Pain Clinic Polypharmacy Champion ACB LEARNINGS AND CHANGES • ePACT2: Polypharmacy prescribing comparators. ACB score is incorporated into indicators available through ePACT2, which identifies numbers of patients with ACB scores ≥6, ≥9 or ≥ 12 in a month. • Performing AEC/ACB score screens at any Ad-Hoc opportunity: discharges, letters, SMR’s, repeat prescriptions authorisations. • Influencing colleagues about ACB/AEC importance. • Importance of always putting patient health best interest first, regardless time constraints. 6 2 Patient X AEC reduction AEC 6 AEC 2 Time (wks) FCS IQCODE 0 6 3.38 4 6 3.12 8 6 3.01 12 5 2.89 Figure 2. Rockwood Frailty Scale 10 REFERENCES 1. Bell B, Avery A, Bishara D, Coupland C, Ashcroft D, Orrell M. Anticholinergic drugs and risk of dementia: Time for action? Pharmacol Res Perspect. 2021;9(3). doi:10.1002/PRP2.793 2. Scottish Government Polypharmacy Model of Care Group. Polypharmacy Guidance, Realistic Prescribing 3 rd Edition, 2018. Scottish Government. Published 2018. Accessed September 19, 2022. https://www.therapeutics.scot.nhs.uk/wp-content/uploads/2018/04/Polypharmacy-Guidance-2018.pdf 3. Gorup E, Rifel J, Petek Šter M. Anticholinergic Burden and Most Common Anticholinergic-acting Medicines in Older General Practice Patients. Slovenian Journal of Public Health. 2018;57(3):140. doi:10.2478/SJPH-2018-0018 4. Cardwell K, Hughes CM, Ryan C. The Association Between Anticholinergic Medication Burden and Health Related Outcomes in the ‘Oldest Old’: A Systematic Review of the Literature. Drugs Aging. 2015;32(10):835-848. doi:10.1007/S40266-015-0310-9 5. Bulletin 253: Anticholinergic burden | PrescQIPP C.I.C. Accessed September 19, 2022. https://prescqipp.info/our-resources/bulletins/bulletin-253-anticholinergic-burden/ 6. PrescQIPP. B140. Anticholinergic drugs 2.1. Accessed September 19, 2022. www.prescqipp.info 7. Aging Brain Program of the Indiana University Center for Aging Research. ANTICHOLINERGIC COGNITIVE BURDEN SCALE. Published 2012. Accessed September 19, 2022. https://gwep.med.ucla.edu/files/view/docs/initiative2/conferences/Anticholinergic-Burden-Scale.pdf 8. Clinical Frailty Scale Health Questionnaire. Accessed September 19, 2022. https://cdn.dal.ca/content/dam/dalhousie/pdf/sites/gmr/2021-08-03_CFS%20Questionnaire%20Online%20Version.pdf 9. CFS Classification Tree - Geriatric Medicine Research - Dalhousie University. Accessed September 19, 2022. https://www.dal.ca/sites/gmr/our-tools/clinical-frailty-scale/cfs-classification-tree.html 10. Clinical Frailty Scale (Rockwood) : Frailty Toolkit. Accessed September 19, 2022. https://www.frailtytoolkit.org/rockwood/ 11. Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) | Doctor | Patient. Accessed September 19, 2022. https://patient.info/doctor/informant-questionnaire-on-cognitive-decline-in-the-elderly-iqcode 12. Medichec. Accessed September 19, 2022. https://medichec.com/ Table 1. Patient X IQCODE results along time 11 Figure 1. Patient X MEDICHEC AEC score comparison 1 Oxybutynin Solifenacin Promethazine Hydroxyzine 3 3 1 1