Download as PDF, PPTX
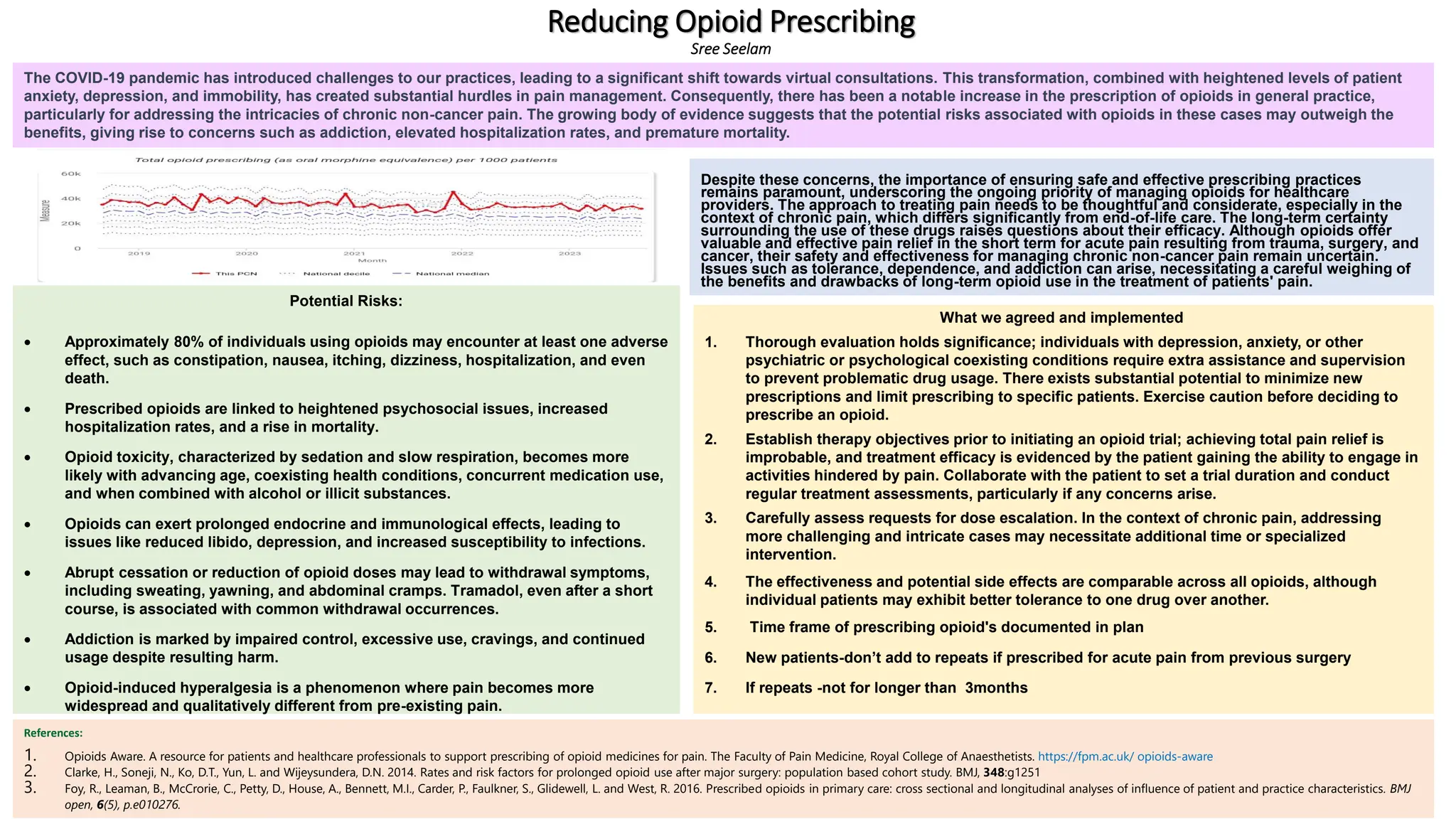

The document outlines the significant risks associated with opioid prescribing, including potential adverse effects, heightened psychosocial issues, and addiction. It emphasizes the necessity for careful evaluation and management of opioid prescriptions, especially for patients with coexisting psychiatric conditions and in the context of chronic non-cancer pain. Furthermore, the challenges posed by the COVID-19 pandemic have led to increased opioid use, raising concerns about their long-term efficacy and safety.



































































