
Recommended
More Related Content
What's hot
What's hot (20)
Similar to HEALTH INSURANCE
Similar to HEALTH INSURANCE (20)
Recently uploaded
Recently uploaded (20)
HEALTH INSURANCE
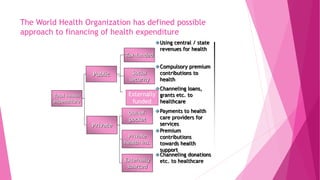
- 1. Total health expenditure Public Private Social security Private health ins. Externally sourced Out-of- pocket Using central / state revenues for health Compulsory premium contributions to health Channeling loans, grants etc. to healthcare Payments to health care providers for services Premium contributions towards health support Channeling donations etc. to healthcare Tax-funded Externally funded The World Health Organization has defined possible approach to financing of health expenditure
- 2. 19-01-2018 2 Rashitha Sithika D/o.Mohamed Abu-Bakr Sithik residing at No.484, Telugu colony, Thamaraipakkam Koot Road, Kanchipuram District, Tamil Nadu. She is a 4 years old baby. Since her birth, she had squint on Right Eye and blurred vision on her both eyes. She checked her eyes in a reputed hospital in Chennai. Under chief minister health insurance scheme she was operated in sankar eye hospital in pammal .she regained her sight.
- 4. Objectives: 1) Able to explain the terms used in health insurance . 2) Able to enumerate the types,advantage and disadvantage of health insurance. 19-01-2018 4
- 5. Synopsis Terms used in insurance objectives History of health insurance Definition: Need of the health insurance Types of health insurance Chief Minister's Comprehensive Health Insurance Scheme Private health insurance IRDA How to go for insurance- basics SWOT analysis summary 19-01-2018 5
- 6. Terms used in insurance Insured.: The person or business that gets compensated if the loss occurs. Insurer: The company that agrees to pay the compensation Premium: The money that is paid by the Insured to the Insurer. the payment required to keep your insurance policy in force Policy:legal document issued by insurance company that outlines the terms and conditions of the insurance. Policyholder – the person who buys the insurance; also called the "insured." Claim –. a person's request for payment by an insurer of a loss covered by a policy first-party claims- claims to your own insurance company pppppppppolicyPolicy Policy – the legal document issued by the insurance company that outlines the terms and conditions of the insurance. 19-01-2018 6
- 7. TO BE CONTD third-party claims- claims made by one person against another person's company Policyholder – the person who buys the insurance; also called the "insured." Exclusion – specific conditions or circumstances listed in the policy that are not covered by the policy. Occurrence – an accident that results in bodily injury during the period of an insurance policy. Peril – the cause of loss or damage. Risk – the chance of a loss Underwriting – the process of selecting risks for insurance, and determining how much to charge to insure these risks and which coverage to provide. 19-01-2018 7
- 8. TO BE CONTD TPA- means an organization, as defined and licensed under the Insurance Regulatory and Development Authority regulations-2001 and is engaged for a fee or renumeration by an Public Sector insurance company for the provision of health services. 19-01-2018 8
- 9. History of health insurance International origin: 1883 Bismarck- sickness benefit to workers. 1911 Lloyd George- National Health Insurance Scheme to cover sickness expense, medical relief, drugs & compensation of wages lost, to improve quality of life and improve industrial production. J.F.Kimball: prepayment system of health care. 1958 the Canadian Hospital and Diagnoses Act provided full hospital services almost free of charge in public wards 19-01-2018 9
- 10. National origin: 1912 Insurance Act, 1912 passed, setting down rules and regulations specific to insurance industry. 1923: Workman’s compensation Act. 1948: ESI Act passed. 1952: First ESI hospital established. Mudaliar Committee(1959-1961) recommendations: 1. Long range health insurance policy for all. 2. Small fee for availing health services. 1999: IRDA act passed. 2001: Insurance amendment Act: Emphasis onTPAs. 19-01-2018 10
- 11. HEALTH INSURANCE Definition: 19-01-2018 11 Health insurance is an insurance product which covers medical and surgical expenses of an insured individual. It reimburses the expenses incurred due to illness or injury or pays the care provider of the insured individual directly.
- 12. System of assurance to make contingencies of health care expenses To provide protection against financial loss by un foreseen sickness To meet cost of good medical care Relieves anxiety and tension 19-01-2018 12
- 13. NEED OF THE HEALTH INSURANCE Lack of financial capability amongst the poor Increasing cost of medical care Health insurance protect from unexpected high cost. Make quality treatment affordable. Cashless benefits. Tax benefit. 19-01-2018 13
- 14. Types of health insurance Health insurance social Community based private Governm ent initiated Normally managed by community /groups Risk rated and offered by commercial organization
- 15. Social health insurance Two mandatory and contributory health insurance schemes ESIS CGHS RSBY
- 16. EMPLOYEE STATE INSURANCE ACT 1948 Is an important measure of social security and health insurance in India. It provides certain cash and medical benefits to industrial employees in case of sickness ,maternity and employment injury. It was amended in 1975,1984,1989 and 2010 19-01-2018 16
- 17. Coverage of factories All factories using power & otherthan seasonal factories employing 10/more persons Also small factories employing 10 or more persons ,whether power is used or not Shops Hotels and restaurants Cinemas and theatres Road motor transports etablishments News paper establishments The scheme has been extended to private medical and educational institutions employing 20 or more persons in some states Excludes mines, railways and defence establishments 19-01-2018 17
- 18. Coverage of employees: an ‘employee’ means any person employed for wages in or in connection with the work of a factory or establishment to which this act applies - employees with the monthly wage ceiling of Rs.15000 To encourage employers :to engage persons with disabilities for monthly wage ceiling of Rs.25000 are covered under this act , Govt. of India fully bears the employers’ contribution for the first 3 years. 19-01-2018 18
- 19. ADMINISTRATION -Esi corporation Meets twice a year Chairman –union minister of labour Vice chairman-secretary to minister of labour 5 reps from central government 1 rep from each state government 1 rep from all union territories 5 reps from each employers and employees 2 reps from medical profession 3 members from parliament MAKES POLICIES 19-01-2018 19
- 20. STANDING COMMITTEE:Acts as executive body for executing policies and day to day administration Meets 4 times a year Headed by director general of corporation assisted by insurance commissioner, medical commissioner, financial commissioner and actuary 19-01-2018 20
- 21. Finance: ESI Fund * State Government share 1/8th of expenditure on medical treatment & attendance * 7/8th of the expenditure borne by ESIC -Employers: 4.75% of the total wage bill -Employees: 1.75% of the wages Employees with a daily average wage upto Rs. 150 are exempted from payment of contribution. Employers will however contribute their share 19-01-2018 21
- 22. Benefits: Section 46 of the Act envisages following 7 social security benefits Medical Benefit Sickness Benefit Maternity Benefit Disablement Benefit Dependant Benefit Funeral Expenses Rehabilitation 19-01-2018 22
- 23. MEDICAL BENEFITS Medical care for self and families are admissible from day-one of entering into insurable employment. Whereas, the primary, out patient, inpatient and specialist services are provided through a network of Panel Clinics, ESI Dispensaries and Hospitals. Super Speciality services are provided through a large number of empanelled medical institutions on referral basis. 19-01-2018 23
- 24. SYSTEM AND LEVEL OF MEDICAL CARE SERVICE Provision of medical care is based upon the requirement of the region. The various systems prevalent are:- Allopathy Ayush which include Ayurveda, Sidha, Unani, Homeopathy and Yoga ESI Scheme provides all three different levels of care i.e. Primary care, Secondary care and Tertiary care (Super Speciality care). Primary care is provided through dispensaries & panel clinics. Secondary care is provided through diagnostic centres and hospitals. Tertiary care is provided by entering into tie up arrangement with specialized private and government diagnostic facilities and hospitals 19-01-2018 24
- 25. ESI scheme is provided full medical care to its beneficiaries which include preventive, promotive, curative and rehabilitative services. PROVISION OF MEDICAL CARE Medical care services to beneficiaries are provided by two ways:- Direct Provision through ESI schemes own network of dispensaries, diagnostic centres and hospitals. by service dispensaries ,part time dispensaries and mobile dispensaries Indirect Provision through tie-up with private clinics (panel system), diagnostic centres and hospitals SCALE OF MEDICAL BENEFIT Full Medical care is provided as per the need of the patient irrespective 19-01-2018 25
- 26. SICKNESS BENEFIT Sickness Benefit is payable to an insured person in cash, in the event of sickness resulting in absence from work and duly certified by an authorized medical officer/practitioner. The benefit becomes admissible to insured persons in respect of whom contribution is paid or payable for at least 78 days in corresponding contribution period of six months and have completed 9 months in insurable employment. Sickness Benefit is payable for a maximum of 91 days in two consecutive benefit periods of sickness benefit at 70% of average daily wages 19-01-2018 26
- 27. EXTENDED SICKNESS BENEFIT (CASH) Extended Sickness Benefit becomes payable to insured persons for the period of certified sickness in case of specified 34 long term diseases and in case of rare diseases that need prolonged treatment and absence from work on medical advice. For entitlement to this benefit an insured person should have been in insurable employment for at least two years. He/she should also have paid contribution for a minimum of 156 days in the preceding four contribution periods or say two years. Extended sickness benefit at 80% of average daily wages 19-01-2018 27
- 28. EXTENDED SICKNESS BENEFIT ESB is payable for a maximum period of two years (including 91 days as SB) on the basis of proper medical certification and authentication by the designated authority. The benefit is payable within 7 days following the submission of complete claim papers at the Branch Office concerned 19-01-2018 28
- 29. ENHANCED SICKNESS BENEFIT (CASH) This cash benefit is payable to insured persons in the productive age group for undergoing sterilization operation, -vasectomy/tubectomy. The contributory conditions are same as for the normal Sickness Benefit. Enhanced Sickness Benefit is payable to an Insured Women for 14 days for tubectomy and for 7 days in case of vasectomy in respect of male IPs. The amount payable is 100% of the average daily wages. 19-01-2018 29
- 30. MATERNITY BENEFIT (CASH) Maternity Benefit is payable to Insured Women in case of confinement or miscarriage or sickness related thereto in a benefit period. The benefit is normally payable for 12 weeks for normal delivery and 6 weeks for miscarriage, extendable by 4 weeks for sickness arising out of confinement. The rate of payment of the benefit is 100% of the average daily wages. The benefit is payable within 14 days of submission of records 19-01-2018 30
- 31. DISABLEMENT BENEFIT (CASH) Disablement Benefit is payable to insured employees, being in insurable employment, suffering from physical disablement due to employment injury or occupational diseases. An insured person should be an employee on the date of the accident. Temporary disablement benefit at 90% of the average daily wages is payable till temporary disablement lasts. In case of permanent disablement, the cash benefit is payable for whole life. Amount payable is worked out on the basis of loss of earning capacity determined by a Medical Board. 19-01-2018 31
- 32. DEPENDANTS’ BENEFIT (CASH) Dependants’ Benefit (Family Pension) becomes payable to dependants of a deceased insured person where death occurs due to employment injury or due to occupational disease. Minimum amount-Rs 1200/family A widow can receive this benefit on a monthly basis for life or till her re- marriage. Son upto age of 25 years and unmarried daughter can receive benefit. Other dependants like parents including a widowed mother etc. can also receive this benefit under certain conditions. The rate of payment is 90% of the average daily wages distributed among the dependants in a fixed prescribed/ ratio/ proportion. The first payment is payable within a period of three months following the death of an insured person and thereafter periodically on regular monthly basis. 19-01-2018 32
- 33. OTHER BENEFITS OFFERED BY THE SCHEME Funeral expenses on death of an I.P. subject to a maximum of a Rs10,000/- payable at the Branch Office. The claim of such payment should be made within three month of the death of IP. Vocational Rehabilitation in case of physical disablement due to employment injury under 45 years of age with 40 percent or more disablement. Payable as long as vocational training lasts - actual fee charged or Rs.123/- a day whichever is higher Rehabilitation: The rate of contribution for superannuated/disabled IP is Rs.120/- per annum payable in lump sum at the Branch Office for availing reasonable medical care for self and spouse. 19-01-2018 33
- 34. OTHER BENEFITS OFFERED Free supply of physical aids and appliances such as crutches, wheelchairs, dentures, spectacles and other such physical aids. Preventive health care services such as immunization, family welfare service, HIV/AIDS detection, treatment etc. Confinement Allowance @ Rs.2500/- is paid to an insured woman or insured person in respect of his wife in case confinement occurs at a place where necessary medical facilities under ESI Scheme are not available. This is paid for two confinements only 19-01-2018 34
- 35. UNEMPLOYMENT ALLOWANCE Unemployment Allowance named as Rajiv Gandhi Shramik Kalyan Yojana, is payable to workers facing involuntary unemployment due to closure of factory/establishment or retrenchment or permanent invalidity. The daily rate of Unemployment Allowance is 50% of the average daily wages. This allowance is payable for a maximum period of 12 months during entire life either in one spell or in different spells of not less than one month’s duration. 19-01-2018 35
- 36. Super Speciality Treatment (SST) The insured persons and their family members are entitled to Super Speciality medical care and /or reimbursement along with the cost of supply of medicines if the I.P completes three months service and contribution for 39 days w.r.t self and six month service and 78 days contribution in case of family members. 19-01-2018 36
- 37. INCENTIVES TO EMPLOYERS IN THE PVT. SECTOR PROVIDING EMPLOYMENT TO THE PERSONS WITH DISABLITIES Persons with disabilities employed on or after 01.04.2008 and drawing monthly wages upto Rs.25000/- are covered under the Scheme and Employers’ share of contribution is paid by Government for three years. THE NATIONAL TRAINING ACADEMY is the nodal agency to handle all matters relating to training of officers and staff of ESIC and officer and staff working under ESIS in State Government. NTA is presently functioning under the charge of Commissioner who is assisted by officers of other categories and medical officers 19-01-2018 37
- 38. 201O AMMENDMENT SALIENT POINTS IN ESI ACT Enhancing age limit of children for eligibility to dependants benefit Sec.2(6A)(i) & (ii): Age limit of dependant legitimate or adopted son for eligibility to dependants benefit enhanced from 18 years to 25 years Inclusion of minor brother/sister the definition of family Sec.2(11)(vi): It is proposed that in case of unmarried IPs whose parents are also not alive, dependant minor brother or sister be made eligible for medical care. 19-01-2018 38
- 39. Change in definition of ‘factory’ Sec.2(12): “factory” now comprises of any premises where 10 or more persons are employed irrespective of whether power is used in the manufacturing process or not Replacing the words ‘insured person’ with ‘employee’ Sec.51-A to 51-D: The words ‘insured person’ in Sec.51-A to 51-D have been substituted with the words ‘employee’ to prevent misuse/mis-interpretation by persons who remain IPs after going out of employment and suffer injury. Continuance of medical care to IPs retiring under VRS/pre-mature retirement Sec.56(3) & 95(ehh): Continuing medical care to IPs retiring under VRS schemes or taking premature retirement and their spouse. 19-01-2018 39
- 40. Setting up of State level autonomous Corporations Sec. 58(5) (6), Sec.96: New provision empowering State Govts. to set up state level autonomous organizations for administering medical care in the states. Provision for setting up of medical colleges : New Sec.59-B : Provision made for establishment of medical colleges, nursing colleges and training institutions for para-medical staff. 19-01-2018 40
- 41. Rajiv Gandhi Shramik Kalyan Yojana- (Unemployment Allowance Scheme) Scheme introduced w.e.f. 1-4-05. Insured person who becomes unemployed after being insured for 5 or more years, due to closure of factory/ establishment, retrenchment or permanent invalidity are entitled to:- Unemployment Allowance equal to 50% of wage for a maximum period of upto one year, Medical care for self and family from ESI Hospitals/dispensaries during the period IP receives unemployment allowance Vocational Training provided for upgrading skills – Expenditure on fee/ traveling allowance borne by ESIC. 19-01-2018 41
- 42. Reimbursement of Funeral expenses enhanced from Rs.5,000 to Rs.10,000/- Rate of Confinement Expenses payable to insured women for confinement outside ESI Hospitals raised from Rs.1000 to Rs.2500 . Differently-abled workers drawing wages upto Rs.25000 covered under the scheme and employers contribution borne by Central Government for initial three years to encourage employers to give employment to such workers. ISO Certification for all ESI institutions Grading of ESI Hospitals through professional Agencies. Client satisfaction survey being conducted in-house as well as through professional agencies. Utilization of underutilised capacity in ESI Hospitals to provide medical services to BPL workers under Rashtriya Swasthya Beema Yojna. 19-01-2018 42
- 43. PANCHADEEP PROJECT IT Enablement Project under implementation which will provide [PANCHADEEP PROJECT]:- PEHCHAN cards for IP and family which will enable availment of benefits anywhere anytime. Insurance number & Card to remain same even if job changes. Online registration of factory/estt., employees Online submission of challan and contribution payment IP can access eligibility, status of claims Registration of patients in hospitals/dispensaries & Medical history of patient. 19-01-2018 43
- 44. 19-01-2018 44
- 45. RECENT INITIATIVES Modernisation/upgradation/expansion of all ESI Hospitals to bring them at par with best Corporate hospitals. Hospital Development Committees constituted in all ESI Hospitals with executive/financial powers and representation of stakeholders. Medical Colleges, Para-medical and nursing training institutions will be set up to improve quality of medical care and to overcome shortage of medical/para- medical personnel. Tie-up arrangements with 417 hospitals (govt/private ) for providing cashless super specialty services and specialties not available in ESI Hospitals anywhere in the country as per IPs choice 19-01-2018 45
- 46. Tie- up arrangement for primary care where 5000 IPs are there and there is no ESI dispensary within 8 Kms. Tie up arrangement for secondary and tertiary care where: a] 25000 IPs but ESI Hospital is more than 25 Kms away; b]15000 IPs but ESI hospital is 75 to 125 Kms away; c]10000 IPs but ESI Hospital is more than 125 Kms away 19-01-2018 46
- 47. NETWORK OF MEDICAL FACILITIES 1384 -Esi dispensaries 2100 -Panel clinics 307 -Diagnostic centres 151 -Esi hospitals 116 hospitals directly run by STATE govt.and 35 run by ESIC. Hospital annexes are-42 with 27000 beds Super speciality medical care given with advanced medical institution Cash payment –through 624 branch offices and 197 cash offices Head office in New Delhi .23 regional office,26 sub regional office 19-01-2018 47
- 48. CENTRAL GOVERNMENT HEALTH SCHEMES The Central Government Health Scheme (CGHS) was started under the Indian Ministry of Health and Family Welfare in 1954 with the objective of providing comprehensive medical care facilities to Central Government employees, pensioners and their dependents residing in CGHS covered cities. The scheme was initially started in Delhi in 1954. Subsequently CGHS Services were extended to the following 17 cities Allahabad, Ahmadabad, Bangalore, Chennai , Guwahati,Lucknow,hyderabad Jaipur, Jabalpur, Kolkata, Kanpur, Mumbai, nagpur, Patna, Pune ,Thiruvananthapuram and West Bengal, 19-01-2018 48
- 49. The Central Govt. Health Scheme is applicable to the following categories of people residing in CGHS covered cities: Central Govt. Servants paid from Civil Estimates (other than those employed in Railway Services and those employed under Delhi Administration except members of Delhi Police Force). Pensioners drawing pension from Civil Estimates and their family members (Pensioner residing in non- CGHS areas also may obtain CGHS Card from nearest CGHS covered City) Members and Ex-members of Parliament Judges of the Supreme Court and High Court (sitting and retired) Freedom Fighters Central Government Pensioners, Employees of Semi-Autonomous bodies/Semi Government Organisations Accredited Journalists Ex-Governors and Ex-Vice-Presidents of India 19-01-2018 49
- 50. The medical facilities are provided through Wellness Centres(previously referred to as CGHS Dispensaries) /polyclinics under Allopathic, Ayurveda, Yoga,Unani Sidha and Homeopathic systems of medicine. Service rendered via 254 allopathic dispensaries 9 polyclinics 78 Ayush dispensary/ units 3 Yoga Centres 65 Laboratories 17 Dental Units 19-01-2018 50
- 51. Main components of cghs: The dispensary services including domiciliary care. F. W. & M.C.H. Services Specialists consultation facilities both at dispensary, polyclinic and hospital including X-Ray, ECG and Laboratory Examinations Hospitalization Organization for the purchase, storage, distribution and supply of medicines and other requirements. Health Education is also given to beneficiaries. 19-01-2018 51
- 52. 19-01-2018 52
- 53. UNIVERSAL HEALTH INSURANCE SCHEME Government of India launched the universal health insurance in 2003 It is a standard mediclaim product with an annual cover of Rs 30,000 for a family It was marketed by the public sector insurance companies and was for BPL population But it failed due to lack of willingness of insurers, improper identification of beneficiaries and in adequate coverage It was superseded by RSBY 19-01-2018 53
- 54. RASHTRIYA SWASTHYA BIMA YOJANA GOALS:Inability to deal with medical emergencies without facing a financial crisis Heavy expenditure on medical care and hospitalization Recourse to adequate and competent treatment 19-01-2018 54
- 55. BENEFITS:Total sum insured of Rs 30,000 per BPL family on a family floater basis Pre-existing diseases to be covered Coverage of health services related to hospitalization and services of surgical nature which can be provided on a day-care basis Cashless coverage of all eligible health services. Provision of Smart Card. Provision of pre and post hospitalization expenses. Transport allowance @ Rs.100 per visit upto maximum of Rs 1000 19-01-2018 55
- 56. It is implemented by the Identification of Insurance agency Enrollment of Beneficiaries and Delivery of Smart Card to commence Empanelment of Government and private institutions Payment of insurance premium to the insurance service provider. Delivery of health services 19-01-2018 56
- 57. QUALIFICATION OF INSURANCE COMPANY Registered with IRDA Should have full-fledged establishment with experience in conceptualizing, designing and implementing large health care schemes At least one year experience in catering Health Insurance of 50,000 families or more under one group insurance policy in 2005-06 or 2006-07 19-01-2018 57
- 58. Both public, including ESI, and private health providers could offer services The service providers should possess specified basic facilities, like:- At least 10 inpatient medical beds; Medical & Surgical facilities along with Diagnostic facilities i.e. Pathological test, X-Ray, ECG, etc. 19-01-2018 58
- 59. FUNDING Contribution by GOI : 75% of the estimated annual premium of Rs 750, subject to a maximum of Rs. 565 per family. Contribution by the State Governments: 25% of the annual premium and any additional premium beyond Rs 750. Beneficiary to pay Rs. 30 per annum as Registration Fee/ Renewal Fee Administrative cost to be borne by the State Government will come from Rs 30 received from beneficiary Cost of Smart Card to be borne by the Central Government. An additional amount of Rs.60 per beneficiary would be available for this purpose. 19-01-2018 59
- 60. AAM ADMI BIMA YOGANA WITH RSBY AABY Provides for insurance of head of the family or an earning member of the family of rural landless household between the age of 18 to 59 years against natural death as well as accidental death and partial/permanent disability. AABY is now collaborating with RSBY 19-01-2018 60
- 61. Ex-serviceman contributory health scheme 19-01-2018 61 This scheme is meant for ex army personals They have to contribute as per laid norms and they are entitled for specific services in lieu of contributions. It was launched with effect from April 1 2003 The objective was to provide medical care to its members and its dependant It has 227 polyclinics ,106 military and 121 non military stations It was fully established by 31 march 2008 It covers 320lakh ex-serviceman and 10 million beneficiaries
- 62. COMMUNITY HEALTH INSURANCE Is NOT- FOR –PROFIT insurance scheme Aimed at the informal sector and formed on the basis of a collective pooling of health risks, and in which the members participate in its management Initiated by NGOS Mainly to improve access to health care Covers about 1000 to 100,000 people Covers mostly poor and near poor 19-01-2018 62
- 63. 3 basic models of CHI Provider model Insured model Linked model 19-01-2018 63
- 64. Example YESHASVINI –karnataka-june 2003 ORGANISED BY YESHWANI TRUST Eligibility –cooperative farmers and their families Premium-Rs 120+30 per person per year Benefit –any surgery up to Rs 1 lakh per hospitalization and 2 lakh per patient per year Providers – empanelled hospital Administration by TPAS 19-01-2018 64
- 65. KARUNA TRUST Initiated in September 2002 in karnataka Organised by karuna trust Eligibility –BPL families in talukas where karuna trust works Premium-Rs 20 per person per year Benefit- hospitalization expenses up to Rs 2500;loss of wages up to Rs 1500; payment to the doctors up to Rs 1500 Providers –only government hospitals Now covering 10,000 people 19-01-2018 65
- 66. RAJIV AAROGYA SRI HEALTH INSURANCE SCHEME To improve access of BPL families to quality medical care for treatment of identified diseases involving hospitalization, surgery 1. Heart 2 Cancer treatment 1. Surgery/Therapy 2. Chemo Therapy 3. Radio Therapy 4. Neurosurgery 5. Renal diseases 6. Burns 7. Poly trauma cases (not covered by the Motor Vehicles Act) 8. Cochlear Implant Surgery with Auditory-Verbal Therapy for Children below 6 years 19-01-2018 66
- 67. SELF EMPLOYED WOMEN ASSOCIATION SEWA is a trade union for poor, self-employed women workers in India It was founded by famous gandhian and civil rights leader dr Elabhatt in 1972 members are women who earn a living through their own labour or small business SEWA began offering health insurance, which cost their member Rs 85 annually Since 1992, Vimo SEWA has provided life and hospitalization insurance for its members and their families for as little as Rs 100 per person 19-01-2018 67
- 68. CONCULSION: 19-01-2018 68 Useful tool to improve access to health care and protect families from impoverishment But there are some preconditions- trustworthy organization Good quality providers Community with some means Managerial skills
- 69. PERFORMANCE OF CHI: Able to reach out to the weaker sections of society Provide some form of health security Has improved access to health care Has protected households, but only partially Has not improved quality of care for the patient Many of them require external subsidies 19-01-2018 69
- 70. Chief Minister's Comprehensive Health Insurance Scheme Objectives:universal health care, providing affordable and quality health service effective in fulfilling the public aspirations. State empowered committee under chairpersonship of chief secretary of Tamilnadu and 12 members to process and finalize the tender and to provide operational guidelines for the implementation of the scheme. State empowered committee meeting held on 13-7-2011 has suggested to name the NEW COMPREHENSIVE HEALTH INSURANCE SCHEME as CHIEF MINISTER ‘S COMPREHENSIVE HEALTH INSURANCE SCHEME 19-01-2018 70
- 71. ELIGIBLE PERSON :The Eligibility to avail Chief Minister’s Comprehensive Health Insurance Scheme, is as indicated for the resident of tamilnadu by the presence of his/her name in the Family card and whose annual income is less than Rs.72, 000/ per annum. , it is sufficient to produce family card and Income certificate by the VAO/Revenue authorities along with the self declaration of the head of the concerned family. “Family” includes the eligible member, and the members of his or her Family as detailed below: (i) Legal spouse of the eligible person (ii) Children of the eligible person (iii) Dependent parents of the eligible person. Srilankan refugees in the camps are also eligible without any Income limit. Migrants from other states can also join this CMCHIS based on the request letter along with a list of Eligible member’s from labour department, provided they have resided for more than six months in the state as certified by suitable authority. 19-01-2018 71
- 72. Orphans residing in any registered/unregistered organization can be given a singlecard. This also includes the rescued girlchildren and any other person defined as orphan by the government. 19-01-2018 72
- 73. PREMIUM PAID: 699rs/per family per year for 1.34 crore families in Tamilnadu. A 24 hour Call Centre has been set up at CMCHISTN Project Office with sufficient manpower with toll free help line. The Toll Free Number is 1800 425 3993. TPAs: United India Insurance( TTK health care TPA Private limited,MD India health care TPA private limited,Medi Assist India TPA Private Limited. 19-01-2018 73
- 74. Free health camps / screening camps will be conducted by network hospitals as per the directions given by Project Director of Tamil Nadu Health Systems Society. Minimum of one camp per month per empanelled hospital will be held in the districts in each policy year. The persons who need treatment are identified in the Health camps. Hospitals to be covered under the scheme:both government and private hospitals with the approval of empanelment and disciplinary committee with a minimum criteria: a)hospital should have at least 30 inpatient beds. b) it should be equipped and engaged in providing medical and surgical facilities along with diagnostic facilities i.e. pathological test, x-ray and other investigation etc. 19-01-2018 74
- 75. c)fully equipped OT d)qualified doctors,nurses,physically in charge round the clock. e)maintain necessary and complete records. 19-01-2018 75
- 76. Private health insurance A voluntary health insurance wherein people can enrol and purchase the insurance product of their liking, paying a risk rate premium Both public and private insurance companies market a variety of health insurance products Out of these mediclaim is the most sold product. Introduced in 1986 A voluntary health insurance scheme offered by the private sector since 1999 Any body =3 months to 80 yrs. who can afford the risk related premium is eligible to join the scheme The premium depends on the age, risk and the benefit package opted for The subscribers are usually the middle and upper class, especially as there is a tax benefit 19-01-2018 76
- 77. legislation Insurance regulation formally began in India with the passing of the Life Insurance Companies Act of 1912 and the provident fund Act of 1912 Insurance is a federal subject in India. There are two legislations that govern the sector- The Insurance Act- 1938 and the IRDA Act- 1999. 19-01-2018 77
- 78. IRDA A regulatory body, controlled by the Indian govern ,governing insurance companies across India The head quarters of IRDA is in Hyderabad AIMS To protect the interests of the policy holders, and To regulate ,promote and ensure orderly growth of the insurance industry Conduction of insurance business across the country in ethical manner 19-01-2018 78
- 79. Composition of Authority As per the section 4 of IRDA Act' 1999, Insurance Regulatory and Development Authority (IRDA, which was constituted by an act of parliament) specify the composition of Authority The Authority is a ten member team consisting of (a) a Chairman; (b) five whole-time members; (c) four part-time members, (all appointed by the Government of India) 19-01-2018 79
- 80. Claim disputes/grievances Ombudsman is a special court constituted under IRDA for addressing grievances associated with insurance claims The claimant can approach the ombudsman for resolving claim issues 19-01-2018 80
- 81. Viewers at this time …… 19-01-2018 81
- 82. List of health insurance companies in India Apollo Munich Health Insurance Company limited Star Health and Allied insurance Co Ltd Future Generali India Insurance Company Ltd Bajaj Allianz General Insurance Co Ltd ICICI Lombard General Insurance Co Ltd National Insurance Co Ltd The New India Assurance Co Ltd Reliance General Insurance Co Ltd 19-01-2018 82
- 83. United India insurance Co Ltd It is a nationalized general insurance company having its operation in whole country Royal Sundaram Alliance Insurance Co Ltd Religare Health Insurance Co Ltd 19-01-2018 83
- 84. How to go for insurance- basic knowledge If you are healthy- Basic Health Insurance Plan If at hereditary risk/poor health-Critical Illness Policy -pays lump sum when holder is diagnosed with one of specified critical illness.( cancer, CAD, Heart attack, major organ transplant, paralysis, stroke) -after lump sum is paid policy terminates -these policies are far cheaper than basic health policies, so can’t depend alone on these. 19-01-2018 84
- 85. Senior citizens specific covers Bajaj Allianz general insurance Silver Health National Insurance Varishtha Mediclaim New India Assurance Sr. Citizen Mediclaim Oriental Insurance Health of Privileged Elder Star Health Allied Sr. Citizen Red Carpet United India Insurance Sr. Citizen Mediclaim 19-01-2018 85 Bajaj Allianz general insurance Silver Health National Insurance Varishtha Mediclaim New India Assurance Sr. Citizen Mediclaim Oriental Insurance Health of Privileged Elder Star Health Allied Sr. Citizen Red Carpet
- 86. ADVANTAGES OF HEALTH INSURANCE Risk Cover Protection against rising health expenses Daily hospital cash allowance Peace of Mind Tax Benefits Coverage of expenses related to organ donors Convalescence Benefits 19-01-2018 86
- 87. DISADVANTAGE Restricted hospital Health does not cover pre-existing diseases Expenses of defect related aids is not covered Eg:- Contact lens, Hearing aids, general ability & intoxicating Drugs Most company do not have separate health insurance cover for a child Older the age higher the cost of premium 19-01-2018 87
- 88. TAX BENEFITS under section 80 D for paying medical insurance premium earlier the deduction allowed was Rs. 15000 In march 2015 which has now been increased to Rs. 25000, which means by additional saving of Rs. 10000, the tax saving will be Rs. 3000 who are in 30% tax bracket and Rs. 1000 for those who are in 10% tax bracket. above 80 years of age. For them additional allowance of Rs. 30000 for expenditure incurred for treatment on certain specified diseases has also been allowed 19-01-2018 88
- 89. conclusion Growth potential for the insurance sector is immense. Consideration required to poor and unemployed. Private health insurance has positive role to play. Insurance sector needs to widen its scope from only providing treatment facilities to promotive and preventive health care 19-01-2018 89
- 90. RajbirKaur,MPH,PU References World Health Organization Park K: Preventive and Social Medicine Rowitz Louis: Public Health for the 21st Century www.google.com Textbook of community medicine suryakantha Global Journal of Management and Business Studies. THE GAZETTE OF INDIA : EXTRAORDINARY [PART II—SEC. 3(i)] www.slidesshare.com
- 91. 19-01-2018 91 Ignoring health insurance is ignoring health... We must select our proper insurance plan !!!
Editor's Notes
- CHARACTERISTIC OF UNORGANIZED SECTOR-POOR Self-Employed Employers not identifiable Illiterate Migratory Lack of skills
- WHO CAN PROVIDE HEALTH INSURANCE
- Exemption to the single speciality hospital/remote area.
- FAMILY PLANS ,DISEASES SPECIFIC PLANS