Meta analysis of percutaneous ventricular restoration (pvr) therapy using the...
WCD
1. An Evaluation of Cardiac Procedures after Use of a Wearable Cardioverter Defibrillator
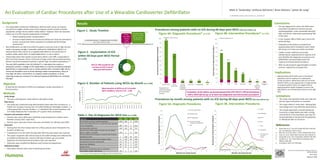
Figure 4A. Diagnostic Procedures* (n=179)
Mark A. Tankersley,1 Anthony DeFrance,1 Brian Altonen,1 James W. Long2
1. HealthHelp, Houston, TX 2. Humana, Inc., Louisville, KY
Figure 3. Number of Patients using WCDs by Month (n=1,199)
Background
• The implantable cardioverter-defibrillator (ICD) has been shown to improve
survival from sudden cardiac arrest and to improve overall survival in several
populations at high risk for sudden cardiac death.1 However, there are situations
where use of an ICD may be inappropriate or delayed:
• Patient awaiting cardiac transplantation 2
• Structural abnormalities and ventricular dysfunction have the potential to
recover causing heart failure symptoms to subside and ICD therapy
unnecessary.3
• Risk stratification can take time while the patient continues to be at high risk and
needs a temporary bridge. A wearable cardioverter-defibrillator (WCD) is an
external device that may be an acceptable alternative for the prevention of
sudden cardiac death when an implantable device is not an option.
• Clinical data shows that overall survival with a WCD is over 99%, comparable to
that of an ICD; however, there is still a lack of large-scale trials proving that these
devices should be employed routinely in specific high-risk patient populations.4,5
• The only WCD available in the US (LifeVest®), is intended to be used as a
temporary solution, a bridge to ICD implantation or until the arrhythmia subsides.
Specifically, it is approved for use in cardiac patients with a transient high risk for
ventricular fibrillation such as those awaiting cardiac transplantation, those at
very high risk after a recent MI or an invasive cardiac procedure, or those
requiring temporary removal of an infected implanted defibrillator for antibiotic
therapy.6
Objective
To describe the utilization of WCD and subsequent cardiac procedures in
clinical practice.
Methods
Study design
• This was a retrospective, observational, descriptive study.
Data source
• This study was conducted using administrative claims data from Humana Inc., a
health care company insuring over 2.8 million Medicare Advantage members, 1.2
million group fully-insured members, 1.1 individual fully-insured members, and
3.9 million Medicare Part D members (2nd quarter 2014 enrollment).
Inclusion and exclusion criteria
• Patients who used a WCD were identified using retrospective medical claims
between January 2011- April 2013.
• Patients were required to have continuous enrollment for 240 days post WCD.
Outcomes
• Starting from the first medical claim for a WCD, patients were followed for the
duration of WCD use.
• Implantation of an ICD within 60 days after WCD discontinuation was reported
• The subset of patients who did not have an ICD within 60 days were followed for
an additional 180 days (for a total of 240 days of follow-up), and cardiac
diagnostic and interventional procedures were also reported.
• Outcomes were stratified by Medicare and Commercial populations.
Statistical analysis
• Descriptive statistics were used in reporting outcomes.
Implications
• Approximately half of WCD users in this patient
population had no evidence of a subsequent
cardiac procedure. While these data do not reveal
whether WCD use was appropriate or inappropriate
in any given patient, there is an opportunity to
apply population health strategies to ensure the
right patients are utilizing these devices at the right
time.
Conclusions
• The top diagnoses for which the WCDs were
prescribed included non-ischemic primary
cardiomyopathies, acute myocardial infarction
(MI), and old MI, collectively representing 78%
of the total.
• In this analysis, 38% of WCD users had an ICD
within 60 days.
• Evaluation of the follow-up showed that
approximately half of all patients with a WCD
did not go on to have any cardiac procedure.
• Cardiac nuclear medicine and cardiac
catheterization represented the majority of all
post WCD/No ICD diagnostic procedures and
defibrillators and pacemakers were the
majority of interventional procedures.
• WCD use decreased at approximately 4 months
and was replaced by increased ICDs.
Society for Medical Decision Making | Miami, Fl
Oct 18-22, 2014
GCHJ3DUEN
Abstract #: 8708
38%
ICD 62%
No
ICD
0
10
20
30
40
50
60
70
80
90
100
Cardiac Nuclear Cardiac
Catherization
Coronary
Computed
Tomography
Angiography
Stress Echo CT_Angiography MRI
OccurrencesofDiagnosticProcedure
Medicare Commercial
5
96
5
2
5
0
10
20
30
40
50
60
70
80
90
100
ICD WCD CABG Pacemaker Stent Left
Ventricular
Assistance
Device
Angioplasty
OccurrencesofInterventionProcedure
Medicare Commercial
28
68
47
3
20
4
Results
Figure 4B. Intervention Procedures* (n=174)
Figure 1. Study Timeline
62% (n=746) of patients did
not have an ICD in the 60
days post-WCD period
0
20
40
60
80
100
120
140
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Jul-12
Aug-12
Sep-12
Oct-12
Nov-12
Dec-12
Jan-13
Feb-13
NumberofWCDs
Mean duration of WCD use of 2.4 months
(95% confidence interval 2.33 – 2.50)
66
2
Evaluation of the follow-up period showed that 47% (567/1,199) of all patients
with a WCD did not go on to have any diagnostic and intervention procedures
Enrollment Period: 1st Medical Claim for WCD
Jan 1, 2011 to Oct 31, 2012
1/1/11 8/31/13
60 day
Post-WCD
Period
(ends
2/28/13)
240 Day Follow-
up for No ICD in
60 day period
(ends 8/31/13)
Figure 2. Implantation of ICD
within 60 Days post-WCD Period
(n=1,199)
Table 1. Top 10 diagnoses for WCD Use (n=1,199)
Procedures among patients with no ICD during 60 days post-WCD (240 days follow-up)
Diagnoses 1st 2nd 3rd Total
Non-ischemic primary cardiomyopathies 1950 206 0 2156
Acute myocardial infarction, unspecified site, episode
of care unspecified 889 126 6 1021
Old myocardial infarction 458 235 18 711
Infection and inflammation reaction due to cardiac
device, implant, and graft 249 1 0 250
Post-procedural percutaneous transluminal coronary
angioplasty status 1 168 46 215
Post-procedural aortocoronary bypass status 11 124 34 169
Paroxysmal ventricular tachycardia 115 28 2 145
Ventricular fibrillation 84 27 3 114
Cardiac arrest 87 27 0 114
Mechanical complication due to automatic
implantable cardiac defibrillator 102 1 0 103
1st, 2nd, and 3rd refer to placement of diagnosis code on medical claim
Figure 5A. Diagnostic Procedures Figure 5B. Intervention Procedures
Procedures by month among patients with no ICD during 60 days post-WCD (240 days follow-up)
0
2
4
6
8
10
12
14
16
18
20
0 1 2 3 4 5 6 7 8
OccurrencesofDiagnosticProcedure
Months into Study Period
Cardiac Catherization
Cardiac Nuclear
CT_Angiography
Coronary Computed
Tomographic Angiography
MRI
0
2
4
6
8
10
12
14
16
18
20
0 1 2 3 4 5 6 7 8
OccurrencesofInterventionProcedure
Months into Study Period
CABG
Angioplasty
Stent
ICD
WCD
Pacemaker
Left Ventricular
Assistance
Device
1. Russo AM, et al. J Am Coll Cardiol 2013;61:1318–68.
doi: 10.1016/j.jacc.2012.12.017
2. Klein HU, et al. Eur Heart J. 2013; 34(29):2230-2242.
3. Francis J, et al. Indian Heart Journal. 2014; 66:68-72.
4. Chung MK, et al. J Am Coll Cardiol. 2010;56:194–203.
5. Lee BK, et al.. Curr Treat Options Cardiovasc Med.
2009;11:360–365.
6. Circulation. 2013; 127: 854-860.
References
Limitations
• This study only reported trends over time and
did not report association or causation.
• This study relied on claims data. Missing data
and coding errors may affect the observations.
• The sample population included individuals
insured by a single health plan with a strong
concentration in the Southeast, and may not
be generalizable to the general US population
or individuals with no insurance.
*Diagnostic and
intervention groups
are not mutually
exclusive