Murley Meghan Thesis Female Heart Rate Variability - A Pilot Reliability Study
Stephania's OEP Poster
1. Changes in cerebrovascular blood flow velocity during the Valsalva maneuver in
women throughout the menstrual cycle and in men
INTRODUCTION
METHODS
RESULTS
REFERENCES
PURPOSE
The purposes of this study were to investigate 1) changes in brain blood flow and
blood pressure in response to the Valsalva maneuver, and 2) changes in cardiovascular
variables that occur during a supine-sit-stand posture change protocol in men and
women throughout the menstrual cycle.
SUMMARY
Stephania Serna1, Simon Kim1, Christopher Hazlett1, Heather Edgell1
1School of Kinesiology and Health Sciences, York University, Toronto, ON, Canada
Women are well known have lower orthostatic tolerance compared to men
(Convertino, 1998). While the exact mechanisms for greater orthostatic intolerance in
women are unclear, changes throughout the menstrual cycle likely play a role. Indeed,
women in the early follicular phase experience greater sensations of light-headedness
compared to the luteal phase (Peggs et al. 2012).
There are many potential areas where female sex hormones can affect the
cardiovascular and autonomic responses to stressors. For example, estrogen has
sympathoinhibitory effects, yet progesterone has been suggested to be
sympathoexcitatory (Carter et al. 2013). These findings suggest that changes in
estrogen and progesterone have the ability to change a woman’s response to
orthostatic stress.
We hypothesized that women in the early follicular phase of the menstrual cycle will
have reduced brain blood flow and cerebral perfusion pressure during a stand test
compared to men and compared to the luteal phase. We further hypothesize that
women in the early follicular phase will have a reduced ability to recover brain blood
flow velocity during late phase II of the Valsalva maneuver compared to men and the
luteal phase.
Healthy men (n=11) and women (n=9) were recruited (age 18-30). Women were
studied in the follicular (Day 2-5; low levels of estrogen and progesterone) and luteal
(Day 18-24; high levels of estrogen and progesterone) phases of menstruation in a
repeated measures design. None were taking oral contraceptives. Brain blood flow
velocity was measured from the middle cerebral artery (MCA) using Transcranial
Doppler (Multigon). A 2 MHz ultrasound probe was positioned on the temple and
peak velocity was obtained. Continuous blood pressure and cardiac output were
measured using a Finometer Pro.
Participants were studied during a supine Valsalva maneuver test (exhalation to
40mmHg for 15 seconds). Cerebrovascular Valsalva ratio (CVR; change in cerebral
diastolic blood flow velocity/time during late phase II) and Centroperipheral Valsalva
ratio (CPVR; CVR/(change in diastolic blood pressure/time) during late phase II)
were calculated (Wallasch et al. 2011; Figure 1).
After the Valsalva maneuver, participants rested supine for 5 minutes then moved in a
continuous motion from supine to a seated position for 5 minutes, and then stood up
for 10 minutes (Figure 2). All data were recorded in LabChart Pro 8.0 and presented
as mean ± standard error. All data were compared using one-way ANOVA, one-way
repeated measures (RM) ANOVA, or two-way RM ANOVA.
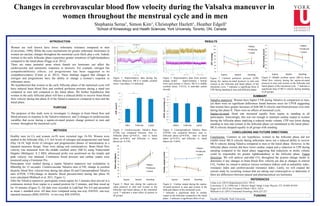
Figure 3: Cerebrovascular Valsalva Ratio
(CVR) was compared between: men vs.
follicular phase (p=0.012), men vs. luteal
phase (p=0.061), and follicular vs. luteal
phases (p= 0.570).
Figure 5: Heart rate during the supine-sit-
stand protocol in men and women in the
follicular and luteal phases of the menstrual
cycle. * indicates a main effect of posture in
all groups.
Figure 8: Middle cerebral artery (MCA) brain
blood flow velocity during the supine-sit-stand
protocol in men and women in the follicular and
luteal phases of the menstrual cycle. * indicates a
significant drop of MCA velocity during standing
in all groups.
Figure 4: Centroperipheral Valsalva Ratio
(CPVR) was compared between: men vs.
follicular phase (p=0.870), men vs. luteal
phase (p=0.423), and follicular vs. luteal
phases (p= 0.464).
Valsalva maneuver: Women have higher CVR during Valsalva in comparison to men,
yet there were no significant differences found between sexes for CPVR suggesting
that women have greater increases of both MCA velocity and blood pressure over time
during late phase II. There were no effects of menstrual cycle.
Supine-sit-stand: Heart rate increased equally from supine to standing in all
participants. Interestingly, this was not enough to maintain cardiac output in women
during the follicular phase implying a reduced stroke volume. CPP was lower during
standing in men and women in the follicular phase yet maintained in the luteal phase.
MCA velocity dropped equally in all groups with standing.
Carter et al. (2013) Hypertension 61(2): 395-9.
Convertino, V. A. (1998) Am. J. Physiol. Regul. Integr. Comp. Physiol. 275: R1909–R1920
Peggs et al. (2012) Int J Gynaecol Obstet 118(3): 242-6.
Wallasch et al. (2011) Functional Neurology 26(4):223-227
Figure 2: Representative data from posture
change model. Approximately 1 minute
from each posture is shown. MCA is middle
cerebral artery. ET-CO2 is end-tidal carbon
dioxide.
Figure 1: Representative data during the
Valsalva Maneuver. MCA is middle cerebral
artery. Late phase 2 is indicated.
Figure 6: Cardiac output during the supine-
sit-stand protocol in men and women in the
follicular phases of the menstrual cycle.
* indicates a significant drop in cardiac
output in the follicular compared to the luteal
phase. † indicates a significant effect of sex.
FUNDING
Faculty of Health, York University
CONCLUSIONS AND FUTURE DIRECTIONS
Late phase 2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
Males Follicular Luteal
CPVR (cm/mmHg x s)
50
55
60
65
70
75
80
85
90
95
100
Supine Seated Standing
Heart rate (bpm)
Males
Follicular
Luteal
*
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Men Follicular Luteal
CVR (cm/s2)
*
2
3
4
5
6
7
8
Supine Seated Standing
Cardiac output (L/min)
Males
Follicular
Luteal
*
†
Figure 7: Cerebral perfusion pressure (CPP)
during the supine-sit-stand protocol in men and
women in the follicular and luteal phases of the
menstrual cycle. * indicates a significant drop of
CPP during standing in men and follicular phase.
70
75
80
85
90
95
100
105
110
Supine Seated Standing
CPP (mmHg)
Males
Follicular
Luteal
*
35
40
45
50
55
60
65
70
75
Supine Seated Standing
MCA velocity (cm/s)
Males
Follicular
Luteal
*
*
Conclusions: Contrary to our hypotheses, women in the follicular phase did not
exhibit lower MCA velocity during orthostatic stress nor a reduced ability to recover
MCA velocity during Valsalva compared to men or the luteal phase. However, in the
follicular phase women did have lower cardiac output and a reduction in CPP during
standing compared to the luteal phase suggesting that reductions in stroke volume
could be responsible for greater lightheadedness in the follicular phase. Future
directions: We will analyze end-tidal CO2 throughout the posture change model to
determine if any changes in brain blood flow velocity are due to changes in arterial
CO2. Further we intend to analyze various resistance indices such as pulsatility index,
resistance index and cerebrovascular resistance index. Lastly, we will expand the
current study by recruiting women that are taking oral contraceptives to determine if
there are differences between natural and pharmaceutical sex hormones.