1. Catherine J Wheeler MD, Angela Deneris CNM, PhD, Elicia Williams-King MD, Shanna M Salmon BS
University of Utah, Salt Lake City, UT, USA
BACKGROUND RESULTS RESULTS
AIMS
• As women age they tend to experience
chronic health problems
• Many chronic health conditions respond to
changes in lifestyle, such as physical activity,
improved nutrition, weight loss, and smoking
cessation
• In response, in 2007 the University of Utah
initiated a multidisciplinary, comprehensive
women’s midlife assessment clinic
CONCLUSIONS
METHODS
RESULTS
2
4
6
8
10
12
14
16
18
20
22
within 1 year1-2 years 2-3 years 3-4 years > 4 years never
GYN
Pap
Mammogram
Primary Care
Lipids
Dermatology
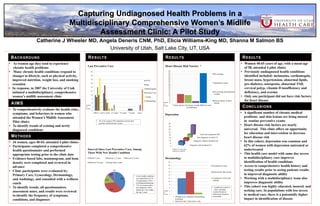
Interval Since Last Preventive Care, Among
Those With New Health Condition
38%
35%
15%
10%
2%
Within 1 year Between 1-2 years Between 2-3 years
Between 3-4 years Greater than 4 years
• A new health condition
was identified in 25 of
34 participants (74%) –
excluding dermatology
• 73% of women with a
new diagnosis had a
health care visit within
the last 2 years
• Women 40-65 years of age, with a mean age
of 58, attended 4 pilot clinics
• Previously undiagnosed health conditions
identified included: melanoma, cardiomegaly,
breast mass, hypertension, abnormal lipids,
pre-diabetes, osteopenia, abnormal TSH,
cervical polyp, vitamin D insufficiency and
deficiency, and eczema
• Only one participant did not have risk factors
for heart disease
Capturing Undiagnosed Health Problems in a
Multidisciplinary Comprehensive Women’s Midlife
Assessment Clinic: A Pilot Study
Number
of
women
• To comprehensively evaluate the health risks,
symptoms, and behaviors in women who
attended the Women’s Midlife Assessment
Pilot clinics
• To identify trends of existing and newly
diagnosed conditions
• 34 women, ages 40-65, attended 4 pilot clinics
• Participants completed a comprehensive
health questionnaire and performed
appropriate testing prior to the clinic date
• Evidence-based labs, mammogram, and bone
density were completed and reviewed in
advance
• Clinic participants were evaluated by:
Primary Care, Gynecology, Dermatology,
and Audiology, and consulted with a wellness
coach
• To identify trends, all questionnaires,
assessment notes, and results were reviewed
to identify the frequency of symptoms,
conditions, and diagnoses
Last Preventive Care
• 26 of 34 women (76%) had been seen by their
provider within the last 2 years
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
* Heart disease risk factors exclude BMI and waist
circumferance
Pre-existing
Identified at clinic
Pre-existing and identified
at clinic
Family history of heart
disease
Heart Disease Risk Factors *
Depression
Diagnosis with treatment (7)
Diagnosis without treatment (6)
New diagnosis in clinic (7)
Total with symptoms (20)
2
6
10
14
18
22
26
30
34
Number of women with
depression symptoms
Number
of
women
2
4
6
8
10
12
14
16
18
20
22
Treatment in clinic
Referred for skin lesions
Treatment in clinic and
referred
• Conditions treated in
clinic included:
- Actinic Keratosis
- Seborrheic keratosis
-Acrocordia
Dermatology
Number
of
women
• 59%had never obtained a Dermatology
evaluation
• Data from last 2 pilot clinics only
• A significant number of chronic medical
problems and skin lesions are being missed
in routine preventive exams
• Heart disease risk factors are nearly
universal. This clinic offers an opportunity
for education and intervention to decrease
heart disease risk
• In this cohort, depression was common and
62% of women with depression untreated or
undertreated
• This health care model with same day access
to multidisciplinary care improves
identification of health conditions
• Access to comprehensive health history and
testing results prior to seeing patients results
in improved diagnostic ability
• Working with a multidisciplinary team also
improves diagnostic ability
• This cohort was highly educated, insured, and
seeking care. In populations with less access
to medical care, there is a potentially higher
impact in identification of disease