❤️ Call Girls service In Panchkula☎️9815457724☎️ Call Girl service in Panchku...
CARDIOVASCULAR DISEASES.pptx
1. CARDIOVASCULAR DISEASES
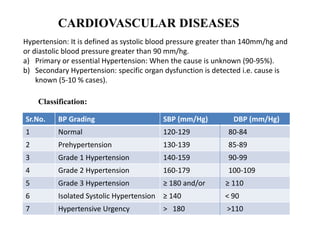
Hypertension: It is defined as systolic blood pressure greater than 140mm/hg and
or diastolic blood pressure greater than 90 mm/hg.
a) Primary or essential Hypertension: When the cause is unknown (90-95%).
b) Secondary Hypertension: specific organ dysfunction is detected i.e. cause is
known (5-10 % cases).
Sr.No. BP Grading SBP (mm/Hg) DBP (mm/Hg)
1 Normal 120-129 80-84
2 Prehypertension 130-139 85-89
3 Grade 1 Hypertension 140-159 90-99
4 Grade 2 Hypertension 160-179 100-109
5 Grade 3 Hypertension ≥ 180 and/or ≥ 110
6 Isolated Systolic Hypertension ≥ 140 < 90
7 Hypertensive Urgency > 180 >110
Classification:
2. Etiopathogenesis of Hypertension
• It is mean the cause and development of a disease or abnormal condition.
• The etiology of primary hypertension is not clear.
• Secondary hypertension can be secondary to:
1. Renal Disease, eg. Chronic diffuse glomerulonephritis, pyelonephritis,
polycystic kidney.
2. Endocrine disease, eg. Cushing syndrome, Pheochromocytoma, primary
hyperaldosteronism.
3. Vascular lesions, eg. Renal artery disese, contraction of aorta.
3. Clinical Manifestations of Hypertension
• Often asymptomatic (Silent killer)
• Non-specific symptoms are fatigue, headache, epistasis, vomiting, giddiness,
breathlessness, and palpitations.
• Stroke, acute myocardial infarction due to vascular disease.
• Symptoms of underlying organ affected due to underlying disease.
• Bruits over carotid.
• Spells of sweating, tachycardia indicates pheochromocytoma.
• Tremors, neck swelling indicates thyroid disorder.
4. Management of Hypertension
• The main aim of the management of hypertension is not only reduction of
BP to target levels but also to lower the cardiovascular risk of the patient.
• Target Bp: 150/90 mm/Hg in elderly and 140/90 mm/Hg in all others
(Including Diabetes mellitus, chronic kidney disease).
5. Non-Pharmacological Management of hypertension
• Reduce dietary sodium intake to not more than 2.4gm sodium or 6gm
sodium chloride per day.
• Adopt DASH eating plan: Diet rich in fruits, vegetables, with low fat dairy
products with a reduced content of saturated and total fat.
(DASH- Dietary approaches to stop Hypertension).
• Physical activity : Regular aerobic activity brisk walking for 30min/day
• Maintain weight : Target BMI 18.5-22.9 kg/m2
• Reduce alcohol consumption.
• Stop smoking
• Stress management
• Yoga
• Patient with grade 1 hypertension may require only lifestyle modification,
which should be tried for 3 months.
6. Type of hypertension Lifestyle Modification Drug Therapy
Normal Encourage No
Prehypertension Yes No
Grade 1 Hypertension Yes Single Agent
Grade 2 Hypertension Yes Combination
Management of hypertension
7. Pharmacological Management Of Hypertension:
In the following Description:
• ACEI is Angiotensin converting enzyme inhibitors,(eg.Enalpril) or
Angiotensin II receptor blockers (eg. Losartan) Use ARBs if the patient is
intolerance to ACE inhibitors.
• Beta blockers (eg. Atenolol).
• CCB is calcium channel blockers (eg. Amlodipine)
• TD is thiazide diuretics (eg. Hydrochlorthiazide)
• MRA: Mineral corticoid receptor antagonist (eg. Spironolactone)
ARB: Angiotensin receptor blocker
8. Grade 1 Hypertension
• If not controlled after 3 months of lifestyle modification or involves more
than 3 risk factors such as: age : men >55 year, Women >65 years,
smoking, obesity, including abdominal obesity, dyslipidemia, impaired
fasting glucose, family history of early coronary artery disease, begin the
drug therapy as ACEI or CCB or TD
• If response is not adequate within 2-4 weeks, add second drug- CCB +
ACEI or ACEI + TD or CCB + TD.
• If response is not adequate within nest 2-4 weeks, add third drug- ACEI +
CCB + TD.
Knowledge,
experience,
skill
Best available evidence
9. Grade 2 Hypertension:
• Begin the drug therapy as soon as grade 2 hypertension is diagnosed. Begin
with ACEI or CCB or TD.
• If response is not adequate within 2-4 weeks, add second drug as add on
therapy CCB + ACEI or ACEI + TD or CCB + TD.
• If response is not adequate within next 2-4 weeks, add third drug- ACEI +
CCB + TD.
Grade 3 Hypertension:
• Use two drugs- ACEI + CCB or CCB + TD or ACEI + TD.
• If response is not adequate within next 2-4 weeks, either increase the dose
of drugs or add third drug- ACEI + CCB + TD.
All Grades of Hypertension with associated clinical conditions:
• Coronary artery disease: Bb+ACEI, CCB (is added only if it is required to
achieve the target BP)
• Congestive heart failure: TD+ACEI+Bb, MRA
• Diabetes mellitus: ACEI or CCB, TD
• Chronic kidney disease: ACEI or CCB or TD (patients with CKD may
require loop diuretics if the glomerular filtration rate is low).
10. Initial, Add-on and maximal Doses of therapy for Hypertension
Drug Doses
Doses for
initiation of
therapy
Enalpril 5 mg
Atenolol 50 mg
Amlodipine 5 mg (2.5 mg in elderly)
Hydrochlorthiazide/
Chlorthiazide 12.5 mg
Add-on doses
Enalpril With Amlodipine 5.0 mg, with
Hydrochlorthiazide 2.5 mg, later 5 mg.
Amlodipine 2.5 mg later raise to 5 mg
Hydrochlorthiazide 12.5 mg
Maximal doses
Enalpril 20-40 mg
Atenolol 100 mg
Amlodipine 10 mg
Hydrochlorthiazide 25 mg
11. Note:
• ACE inhibitors should not be combined with angiotensin receptor blockers.
• Avoid prescribing a combination of beta-blockers and diuretics as they can increase
the risk of diabetes mellitus in those at risk.
Contraindication:
• Amlodipine: Cardiogenic shock, unstable angina, significant aortic stenosis,
worsening angina or increased risk of myocardial infarction may be seen.
• Enalpril: Use of all ACE inhibitors is contraindicated in pregnancy. Bilateral
reanal atrtery stenosis. History of Hypersensitivity.
• Hydrochlorthiazide: Severe hypokalemia, hyponatremia, hypercalcemia.
Hypertension in Pregnancy:
Tablet Methyl dopa: 500mg-1000mg/day in three divided doses.
Tablet Nifedipine Extended release preparation: 30-60 mg OD/BD.
Other drugs that can be given : Labetalol, Hydralazine, Beta blocker.
12. ANGINAAND MYOCARDIAL INFARCTION
Angina and myocardial infarction (MI) are ischemic heart diseases (IHD).
Ischemia is a condition in which there is an adequate supply of blood and
oxygen to a portion of the myocardium.
The manifestation of Ischemic heart disease are:
1. Angina:
a. Stable, exertional angina (Classical angina)
b. Microvascular angina
c. Variant/prinzmetal.vasospastic angina.
2. Acute coronary syndrome (ACS)
a. Unsatble angina (UA)
b. Acute myocardial infarction (AMI)
i) Non-ST segment Elevation MI (NSTEMI)
ii) ST-Segment Elevation MI (STEMI)
13. 1. Angina: It is a pain syndrome due to myocardial ischemia caused by critical
obstruction in coronary arteries due to atheroscelrosis, or calcific aortic
stenosis, or due to vasospasm.
14. Clinically angina can be:
a) Stable, Exertional angina (classical angina): It is predictable. It is usually
provoked by physical exertion or emotional stress when the oxygen demand
of myocardium is increased and is relieved by rest and nitrates when the
increased oxygen demand is withdrawn.
• ECG shows ST depression. It is a result of an imbalance between the oxygen
supply and the oxygen demand of the myocardium.
• The angina index is a measure of the myocardial oxygen consumption.
• It can be calculated as: Angina index = Heart rate + systolic BP
b) Microvascular angina (Cardiac syndrome X): It is more common in
females. Ischaemia is due to endothelial or microvascular dysfunction and no
coronary artery blockage is there.
c) Variant/ prinzmetal/ vasospastic angina : Attacks are unpredictable and
almost always occur at rest or during sleep.
• Spasm of large epicardial coronary arteries responsible for this angina.
• Patients have transient ST elevations on ECG.
15. 2. Acute Coronary Syndrome (ACS):
Acute coronary syndromes refer to range of conditions associated with sudden,
reduced blood flow to the heart producing symptoms compatible with acute
myocardial ischemia which may be life-threatening. According to severity,
acute coronary syndromes may be classified:
a) Unstable Angina: It is more severe than stable angina. It occurs at rest (or
with minimal exertion), usually lasting for more than 10 min.
• It is progressive angina with prolonged or more frequent attacks
superimposed on chronic stable angina.
• Obstruction of the coronary artery is incomplete and myocardial necrosis is
absent.
• Biochemical markers of ischaemia (raised troponin I, myoglobin CK-MK
(creatine kinase myocardial band)) do not appear in blood, and ST segment is
not elevated in ECG.
16. b) Acute Myocardial Infarction (MI):
Myocardial Infarction refers to death of myocytes (necrosis) of a portion of the
myocardium due to sudden occlusion of a branch of coronary artery. It is
commonly known as heart attack.
• Depending on severity, MI can be:
Non- ST-Segment Elevation Myocardial Infarction (NSTEMI):
It is more severe than unstable angina.
Obstruction of the coronary artery is incomplete but myocardial necrosis up to
some extent is there.
Biochemical markers of ischaemia appear in blood but ST segment is not
elevated in ECG.
ST-Segment Elevation Myocardial Infarction (ETEMI):
It is the most serious type of heart attack.
Obstruction of the coronary artery is complete and full thickness of ventricular
wall and larger area of myocardium is necrosed.
ST segment in ECG is elevated and biochemical markers of ischaemia in blood
are prominent.
17.
18.
19. Etiopathogenesis
• Ischemic Heart Disease: Atherosclerosis of the epicardial vessels leading to
coronary heart disease (CHD) is the main etiology of IHD.
• Vasospastic/Prinzmetal angina is caused by vasospasm of coronary artery and
is not caused by atherosclerosis.
Angina:
The cause of angina is less supply of oxygen to the myocardium than the
demand.
Occurrence of angina depends upon two factors (a) Coronary blood flow (b)
Oxygen consumption by the myocardium.
The coronary blood flow may be obstructed by either atherosclerosis or
vasospasm.
Acute Coronary Syndrome (ACS):
The most common underlying cause of ACS is erosion or rupture of an
atherosclerotic plaque which results into platelet adherence, activation,
aggregation and activation of the clotting cascade.
20. Ultimately, a clot composed of fibrin and platelets forms which obstruct the
blood flow.
Unstable Angina:
The most common cause of unstable angina is plaque rupture. Obstruction of
the coronary artery is incomplete and myocardial necrosis is absent.
Myocardial Infarction (MI):
The most common cause of MI is the formation of occlusive thrombus
(Blood clot) at the site of rupture of an atheromatous plaque in a coronary
artery.
STEMI takes place when a coronary artery thrombus forms rapidly.
Unstable angina (UA) can progress to MI and sudden death. Possible STEMI
complications are:
1. Arrhythmias 2. Acute heart failure 3. Rupture of papillary muscle
4. Embolism leading to stroke 5. Ventricular remodelling 6. Ventricular
aneurysm.
21. Clinical Manifestations of Ischemic Heart Disease (IHD)
Angina:
i) Chest pain: pain behind the sternum, heaviness or discomfort which may
radiate to the neck, shoulder, back or the arm.
Pain is usually precipitated by exertion or stress and relieved by rest or nitrates.
ii) Associated symptoms include, sweating, nausea and/or dizziness.
Unstable angina:
i) New onset angina
ii) Angina occuring at rest or with minimal exertion.
iii) Attack is prolonged, usually >20 minutes.
iv) Increasing angina. Progressive angina with prolonged or more frequent
attacks superimposed on chronic stable angina.
Myocardial Infarction:
i) Retrosternal chest pain which is usually described as heaviness, pressure,
tightness, cramping or burning in nature.
ii) Pain may radiate to the jaw, neck, left or both arms, back or shoulder.
22. iii) Pain may occur at rest or during activity and does not respond fully to
Glyceryltrinitrate (GTN). Pain lasts for 10-20 min or longer.
iv) Atypical pattern includes pain develops in the arm, shoulder, wrist jaw or back
without occurrence in the chest.
v) Accompanying symptoms are nausea, vomiting, dyspnoea, diaphoresis, light
headedness, dizziness, syncope, a confusion state, abdominal pain, fatigue and
weakness.
vi) There may be hypo or hypertension, an unexplained drop in arterial pressure,
sudden cardiac arrest, ECG changes showing ischemia or infarction, raised
cardiac markers.
23. Diagnosis and Investigation of Ischemic Heart
Disease
Investigation and diagnosis of IHD involves:
• Typical clinical features
• Determination of biochemical markers of ischaemia
• Complete blood count
• Lipid profile
• ECG
• Chest X-ray
• Coronary CT angiography
• Echocardiography
• MRI
• Stable angina is diagnosed when the chest pain remains unchanged in
severity, frequency and duration over several weeks. Treadmill stress test
confirmed stable angina.
24. Management of angina and myocardial infarction
• Risk factors for ischemic heart disease (IHD) are:
Smoking, Diabetes, Dyslipidemia, Obesity, Hypertension, History of coronary
artery disease.
Angina: The goals for the treatment and prevention of angina are:
To decrease the oxygen requirement of the myocardium
To increase the blood supply to the ischemic region of the heart.
Acute Coronary Syndrome:
Early restoration of blood flow to the infarct-related artery to prevent complete
occlusion and MI in unstable angina or prevent infarct expansion in the case of
MI.
Prevention of death and other complications.
Relief of ischemic chest pain
Maintenance of normal blood sugar levels
Prevention of coronary artery reocclusion.
25. Non-Pharmacological management of angina and
MI
Stable Angina:
• Daily exercise, Stop smoking, Avoid alcohol, Dietary modification: Low
cholesterol, low fat diet with high roughage
• Avoid any activity known to precipitate anginal attack
• Weight reduction in obese patients.
Acute Coronary Syndrome – Unstable Angina and MI:
• Complete bed rest
• Coronary angiography and revascularization therapy should be advised.
Revascularization Therapy:
Revascularization is the restoration of perfusion to a body organ that has
suffered ischemia.
It relieves angina or ongoing myocardial infarction and prevents death due to
myocardial infarction.
Revascularization procedures include percutaneous coronary intervention
(PCI) and coronary artery bypass graft (CABG)
26. Percutaneous Coronary Intervention (PCI)
• PCI is angioplasty with or without stenting. It is carried out without
fibrinolysis.
• A stent is a metal or plastic tube inserted into the lumen of the blocked coronary
artery to keep the passageway open, and stenting is the placement of a stent.
• The following types of stents are available:
a) Bare metal stents (BMS): These are mesh like tubes made up of thin metal
wire. They are without a coating or covering of drugs.
27. b) Drug-eluting stents (DES): These are coated with medicine, which is
released into the artery over time to prevent the artery from narrowing
again.
28. c) Biodegradable or bioabsorbable stents: These stents dissolve after a few months.
They are useful when the need is temporary.
29.
30. PCI is considered in the patients with:
1. Contraindications to IV fibrinolytic therapy.
2. High-risk features with cardiogenic shock.
Contraindications for PCI are:
1. High bleeding risk.
2. Multiple percutaneous coronary intervention restenosis.
3. Intolerance for oral antiplatelets long term use.
Coronary Artery Bypass Graft (CABG):
Coronary artery bypass surgery restores normal blood flow to the heart by
creating bypass around the blocked artery/arteries.
This is done by using a healthy blood vessel called a graft.
A graft is usually a piece of blood vessels located in the chest, leg or arm.
The graft is connected below and above the blocked arteries in the heart.
This creates a new pathway to carry oxygen rich blood to the heart.
31.
32.
33.
34.
35. Pharmacological management of Angina
Stable Angina
• Antiplatelet drug: Aspirin 75mg or Clopidogrel 75mg / day
• Antihyperlipidemic drug: Atorvastatin 40mg or Rosuvastatin 40mg /day
• Nitro vasodilator drugs: Nitrates-sublingual glyceryl trinitrate 300-
500microgram t.i.d. or Isosorbide dinitrate 10mg t.i.d. If there is headache,
lower dose of 5mg twice or thrice daily can be tried.
• Beta-blockers: Metoprolol 50-200mg/day (orally in divided dose.)
• Potassium channel Opener: Nicorandil 10mg BD.
• CCB: Amlodipine, Nifedipine 5-10mg once a day
• Refer for coronary angiogram and revascularization therapy.
36. Unstable Angina And Non-ST-Segmemnt Elevation MI:
• Sublingually Nitroglycerin 300-600 micrograms stat (immediately). It can be
repeated after 5 min. Max 3 doses can be given.
• If symptom persist, administer intravenous Nitroglycerin infusion at dose of 5-
10 microgram/min. Once pain has resolved, oral isosorbide dinitrate 10mg BD
can be given.
• Aspirin initial dose of 325mg followed by 150 mg/day life long.
• Clopidogrel initial dose of 300 mg followed by 75 mg/day for 2 years.
• Atorvastatin 40 mg/day life long.
• IV beta blocker: Metoprolol 5-15 mg over 5 minutes followed by tab
Metoprolol 50-100 mg/day in divided doses with BP monitoring.
• Unfractionated Heparin bolus 60-70 U/Kg (maximum5000 U) Iv followed by
infusion of 12-15 U/Kg per hr. (initial maximum 1000 U/h) titrated to A PTT
50-70 s. OR Enoxaparin 1 mg/kg SC every hr. (PTT: Partial thromboplastin
time.) It indicates how long it takes for blood to clot. (Anticoagulant drug)
37. ST segment Elevated MI:
• Oxygen therapy- 2-4 L/min.
• Sublingually Nitroglycerine 300-600 micrograms start. It can be repeated after
5 min. Max 3 doses can be given.
• If symptom persist, administer intravenous Nitroglycerin infusion at dose of 5-
10 microgram/min. Once pain has resolved, oral isosorbide dinitrate 10mg BD
can be given.
• Aspirin initial dose of 325mg followed by 150mg once a day life long.
• Clopidogrel initial dose of 300 mg followed by 75 mg BD.
• Atorvastatin 80 mg and then 40mg HS (Hora somni at bed time)
• Reperfusion therapy: If presenting within 12 hr of chest pain with ECG
showing ST elevation > 1 mm then give INJ. Streptokinase 1.5 million units
over 1hr. (Thrombolytic drug)
38. Contraindication for this therapy are: (Reperfusion therapy)
i) A history of cerebrovascular haemorrhage at any time.
ii) A non-haemorrhagic stroke or other cerebrovascular event within the past
year.
iii) Marked hypertension at any time during the acute presentation.
iv) Suspicion of aortic dissection, and active internal bleeding.
• Beta blockers: Metoprolol 20-50 mg b.i.d, atenolol 25-100 mg once a day (if
pulse rate >60 beats/min, BP >90/60 mm Hg, lung field clear).
• ACE inhibiors: Enalapril 2.5-20 mg/day in divided doses twice a day.
• Stool softners : Bisacodyl (Dulcolax) 10 mg at night.
39. HYPERLIPIDAEMIA
• Hyperlipidaemia is characterized by elevated levels of total cholesterol (TC),
triglycerides (TG) and /or low density lipoproteins (LDL), very low density
lipoproteins (VLDL) in the blood which is often associated with an increased
risk of cardiovascular disease.
• Hyperlipidaemia is a condition of having serum concentrations of total
cholesterol >200 mg/dL, triglycerides >150mg/dL and/or LDL >130mg/dL,
<40mg/dL.
Classification of Hyperlipidaemia:
a) Hypercholesterolemia: Increased serum level of total cholesterol, low density
lipoproteins, and low density lipoproteins-cholesterol.
b) Hypertriglyceridemia: Increased serum level of very-low-density lipoproteins
and triglycerides.
c) Combined hyperlipidemia: Increased TC, LDL, VLDL, LDL-C and TG.
40. ETIOPATHOGENESIS
• Hyperlipidaemia can be due to primary or secondary causes. Primary
causes include familial hypercholesterolemia which is a genetic disorder.
• Seconadry causes:
Diabetes mellitus , High carbohydrate diet, Hypothyroidism, Sedentary
lifestyle, Renal disease, Alcohol consumption, Hepatic disease,
cholestatic liver disease, Obesity, Cushing disease, Drugs (eg.
Corticosteroids, metoprolol, ciclosporin, estrogens, protease inhibitors,
isotretinoin etc.)
Hyperlipidaemia significantly increase the risk of pancreatitis,
atherosclerotic complications and of cardiovascular events.
41. CLINICAL MANIFESTATIONS
Hyperlipidaemia does not cause any symptoms, Severe hyperlipidaemia may
manifest with secondary diseases such as:
• CHD
• Peripheral arterial disease
• MI
• CAS
• Stroke
• Cholesterol embolization syndrome
42. Diagnosis and Investigation and Management
• It is detected by lipid profile test.
• This test includes : TG, TC, HDL, LDL, and non-HDL levels.
Treatments on Hyperlipideamia:
• It is indicated to reduce the risk of cardiovascular disease, clinical
atherosclerotic cardiovascular disease and diabetes mellitus.
• It involves dietary changes, exercise, and lipid-lowering drugs.
43. Non-Pharmacological Management:
• Motivate all patients to make lifestyle modifications
• Increase physical activity
• Weight loss
• Smoking cessation
• Moderate alcohol intake.
Pharmacological Management:
It is based on patients age, LDL level, and ASCVD risk.
1. First line lipid lowering drugs (Statins): eg. Atorvastatin, Rosuvastatin,
Simvastatin, Pravastatin, Lovastatin, Fluvastatin, Pitavastatin.
2. Second line lipid lowering drugs (Non-statin):
i) Cholesterol absorption inhibitors: Ezetimibe
ii) PCSK9 inhibitor: eg. Evolocumab or alirocumab
iii) Anti-sense apoliprotein B oligonucleotides: eg. Mipomersen
iv) Adenosinetriphosphate-citrate lyase (ACL) inhibitors: eg. Bempedoic acid.
v) Bile-acid sequestrant : eg. Colesevelam.
44. vi) Human monoclonal antibody: eg. Evinacumab
vii) Inclisiran
viii) Microsomal triglyceride transfer protein (MTP) inhibitor: eg. Lomitapide
ix) Lipoprotein lipase activators : eg. Gemfibrozil, benzafibrate, Fenofibrate
x) Lipolysis and triglyceride synthesis inhibitor: eg. Niacin
xi) Omega-3 fatty acids