
Recommended
More Related Content
Similar to 13514403.ppt
Similar to 13514403.ppt (20)
Recently uploaded
Recently uploaded (20)
13514403.ppt
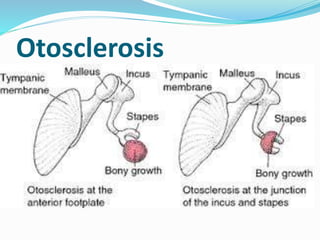
- 1. Otosclerosis
- 2. Otosclerosis Otosclerosis is an autosomal dominant disease, in which the fixation of footplate of the stapes in the oval window will occur due to development of spongy bone from the bony labyrinth, causing immobilization of the footplate of the stapes, which reduces the transmission of vibration to the inner ear
- 3. Etiology It can be 1. Hereditary 2. Endocrine abnormalities 3. Metabolic abnormalities 4. Vascular abnormalities 5. Autoimmune and infectious But none of the cause is been proven as an exact cause
- 4. Pathophysiology Otosclerosis (otospongiosis) is an osseous dyscrasia, limited to the temporal bone, and characterized by resorption and formation of new bone in the area of the Ossicles and Otic capsule (the skeletal element enclosing the inner ear mechanism).
- 5. Otosclerosis has two main forms: An early spongiotic phase (otospongiosis) The early phase is characterized by multiple active cell groups including osteocytes, osteoblasts. It develops a spongy appearance because of vascular dilation secondary to osteocyte resorption of bone surrounding blood vessels. This can be seen grossly as red hue behind the tympanic membrane termed “Schwartze's sign”
- 6. A late sclerotic phase Dense sclerotic bone forms in the areas of previous resorption. Both the sclerotic and spongiotic cells may be present at the same time. Otosclerotic changes always begin in endochondral bone (ossification of cartilage) but may progress and enter even into the membranous labyrinth.
- 7. Signs and symptoms Hearing loss – usually starts in one ear and then moves to the other Dizziness, balance problems, tinnitus
- 8. Diagnositc features History collection Physical examination Audiometry Otoscopic examination Tympanometry CT scan
- 9. Visualization - TM appears normal in the majority of patients Schwartze sign is observed in 10% of patients – otoscopic examination can reveal a reddish blush of the tympanium caused by the vascular and bony changes within the middle ear Rinne test: negative Weber test: laterization to poor Hearing level
- 10. Management Sodium fluoride with vitamin D and calcium carbonate – to retard bone resorption and encourage calcification of bony lesions Dose 20-120 mg per day
- 11. Florical Fluoride: 3.75 mg Calcium :145 mg Florical can be used three times a day for otosclerosis.
- 12. Surgical management Stapedectomy – partial removal of the stapes Stapedotomy – opening in the stapes footplate followed by prosthesis insertion Fenestration surgeries - Complete removal with prosthesis insertion
- 13. Surgery is usually performed under local anesthesia. Poorer functioning ear is treated first Other ear may be treated on 6 months to 1 year later An endaural incision is made Gelfoam is used on the incision flap to limit bleeding
- 14. 14 Prosthesis Placement Cup piston prosthesis Teflon piston prosthesis House wire prosthesis McGee/Fisch-type piston prosthesis
- 16. Nursing management (after ear surgeries) Postoperatively patient may experience dizziness, nausea and vomiting Some will have nystagmus due to the disturbance of perilymph fluid. Decrease sudden movements Actions such as coughing, sneezing, lifting, bending, and straining should be minimized. Do not try to get out of bed without assistance
- 17. Take measures to prevent and cope up with vertigo Report fever, pain and drainage from the ear If the patient needs to cough or blow the nose, leave the mouth open to help reduce the pressure Avoid crowds where respiratory infections may present Avoid high elevations or flying