2. 3. SICKLE CELL DISEASE
LEARNING OBJECTIVES
• Explain the underlying causes of sickle cell
disease(SCD) and their relationship to patient
signs and symptoms.
• Identify the desired therapeutic outcomes for
patients with SCD
• Recommend appropriate pharmacotherapy and
non-pharmacotherapy interventions for SCD
• Recognize when chronic maintenance therapy is
indicated for a patient with SCD.
• Describe the components of a monitoring plan to
assess effectiveness and adverse effects of
pharmacotherapy for SCD
3. What is Sickle Cell disease?
• A serious condition in which red blood cells can become sickle-
shaped
Normal red blood cells are smooth and round. They move easily
through blood vessels to carry oxygen to all parts of the body.
Sickle-shaped cells don’t move easily through blood.
They’re stiff and sticky and tend to form clumps and get stuck in
blood vessels.
The clumps of sickle cell block blood flow in the blood vessels that
lead to the limbs and organs.
Blocked blood vessel can cause pain, serious infection, and organ
damage.
4. Normal and Sickled Red Blood Cells in Blood
Vessels
Figure A shows normal red blood cells flowing
freely in a blood vessel.
The inset image shows a cross-section of a
normal red blood cell with normal hemoglobin.
Figure B shows abnormal, sickled red
blood cells clumping and blocking the
blood flow in a blood vessel.
The inset image shows a cross-section
of a sickled red blood cell with
abnormal strands of hemoglobin.
5. Sickle Cell Anemia vs. Sickle Cell Trait
• People who have sickle cell anemia are born with
it; means inherited, lifelong condition.
• They inherit two copies of sickle cell gene, one
from each parent.
• Sickle cell trait is different from sickle cell anemia.
People with sickle cell trait don’t have the
condition, but they have one of the genes that
cause the condition.
• People with sickle cell anemia and sickle cell trait
can pass the gene on when they have children.
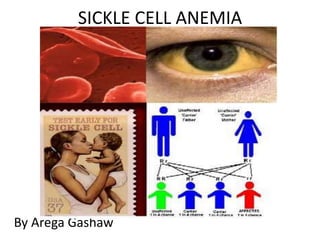
6. Inheritance of Sickle Cell Anemia
If one parent has sickle cell trait (HbAS) and the other does not carry
the sickle hemoglobin at all (HbAA) then none of the children will have
sickle cell anemia (SS).
There is a one in two (50%) chance that any given child will get
one copy of the HbAS gene and therefore have the sickle cell
trait.
It is equally likely that any given child will get two HbAA genes
7.
8. Why Anemia?
Normal red blood cells last about 120 days in the
bloodstream and then die.
In sickle cell anemia, a lower-than-normal number of
red blood cells occurs because sickle cells don’t last
very long.
Sickle cells die faster than normal red blood cells,
usually after only about 10 to 20 days.
The bone marrow can’t make new red blood cells
fast enough to replace the dying ones. The result is
anemia.
9. PATHOPHYSIOLOGY
• Sickle cell anemia is an inherited, autosomal recessive
Hgb disorder characterized by a DNA substitution at the
β-globin gene.
• Patients with SCD predominantly make hemoglobin
S.
• Hemoglobin S differs from normal hemoglobin A by
the substitution of a single amino acid within one of
the two polypeptide chains.
The s Mutation
6th Codon of -Globin Gene
GAG
Glutamic acid
GTG
Valine
11. • Sickle cell anemia results from a DNA substitution
of thymidine for adenine in the glutamic acid
codon, forming a B6 valine instead of glutamic
acid.
• βS represents the inheritance of the sickle β-
globin gene.
• The Hgb produced from this substitution has a
more negative charge than normal HbA, and in
the deoxygenated state will aggregate and
polymerize, forming sickled RBCs.
• Sickled RBCs are more rigid and may become
“lodged” when passing through the
microvasculature, resulting in vascular occlusions.
12. • Deoxygenation causes RBCs to sickle and leads to
vaso-occlusion and blockage of microvasculature,
which can cause sickle cell crisis.
• This blockage causes significant damage to the
endothelium of the arterial and venous circulation.
• Deoxygenation of SS erythrocytes leads to intracellular
hemoglobin polymerization, loss of deformability and
changes in cell morphology.
13. Laboratory Evaluation
• In patients with sickle cell disease,
– the WBC and platelet counts often are elevated, but the
WBC differential is normal.
– The reticulocyte count can range from 5% to 15%,
– the MCV may be elevated.
• If MCV values are less than the normal range,
– iron deficiency or β 0-thalassemia must be considered.
• Sickled cells may also be visually observed in poorly
oxygenated blood of a patient with sickle cell anemia.
• In contrast, a patient with the sickle cell trait should have
– normal RBC morphology and WBC, reticulocyte, and
platelet counts.
– Sickled cells are rarely observed.
14. • SCD usually is identified by routine
neonatal screening programs using
– hemoglobin electrophoresis,
– thin-layer isoelectric focusing,
– high-performance liquid chromatography, or
– DNA analysis.
• All tests are comparable in accuracy.
15. Signs and Symptoms Sickle Cell Trait
• SCD involves multiple organ systems, and its
clinical manifestations vary greatly between and
among genotypes
• Dehydration
• Microscopic hematuria (presence of blood in the
urine)
• Women with SCT also can have frequent urinary
tract infections, especially during pregnancy.
16. Sickle Cell Anemia
• Chronic anemia
• Fever
• Arthralgia
• Abdominal pain
• Weakness
• Anorexia
• Fatigue
• Enlargement of the liver, spleen, and heart
• Hematuria
17. TREATMENT
The goals of treatment are
• To reduce or eliminate the patient’s symptoms;
• Decrease the frequency of sickle crises,
including vaso-occlusive pain crises;
• Prevent the development of complications
• Maintain or improve the quality of life through
decreased hospitalizations and decreased
morbidity.
18. Specific therapeutic options may
– Maintain or increase the hemogloblin level to
the patient’s baseline
– Increase the HbF concentration
– Decrease the HbS concentration
– Prevent infectious complications
– Prevent or effectively manage pain
– Prevent central nervous system damage,
including stroke
19. Initiating Drug Therapy
• No specific treatment is available for patients with
sickle cell anemia.
• The management of SCD focuses on primary
prevention and treatment of the complication
• Children with SCD should be immunized against S.
pneumoniae, H. influenzae and hepatitis B virus.
20. Penicillin
• Penicillin prophylaxis: until 5 years of age--begin at
2 months of age or earlier---even if immunized
– Penicillin V potassium 125 mg po BID until age 3
years, followed by 250 mg BID until age of 5
years.
– Alternate: benzathine penicillin, 600,000 units IM
every 4 weeks for children age 6 months to 6
years, and 1.2 million units every 4 weeks for
those over 6 years of age for whom continued
therapy is warranted.
– Patients who are allergic to penicillin can be
given erythromycin 10 mg/kg twice daily.
20
21. • Folic acid supplementation at a dose of 1 mg/day is
recommended in
– adult patients, women who are contemplating
pregnancy, and patients of all ages with chronic
hemolysis.
• Patients with SCD have an increased demand
for folic acid because of accelerated
erythropoiesis.
21
22. Fetal Hemoglobin Inducers
– hydroxyurea, sodium phenylbutyrate,
decitabine, 5-Azacytidine
– They increases HbF levels, reduces polymer
formation of HbS due to its high oxygen affinity.
– High HbF levels significantly correlate with
decreased RBC sickling and RBC adhesion
– Erythropoietin therapy in combination with
hydroxyurea , erythropoietin increases HbF
levels to a greater extent than hydroxyurea
alone.
23. Hydroxyurea
• Hydroxyurea, a chemotherapeutic agent, increases HbF
levels by stimulating the production of HbF.
• The exact mechanism of HbF production is unknown.
• Other beneficial effects of hydroxyurea include
– Antioxidant properties,
– Increased intracellular water content leading to
increased redcell deformability,
– Decreased red cell adhesion to endothelium, and
– Increased levels of nitric oxide, which is a
regulator involved in physiologic disturbances.
24. • Hydroxyurea reduced the frequency of
hospitalizations and the incidences of pain,
acute chest syndrome, and blood
transfusions by almost 50% in a landmark
trial in adult SCD patients with moderate to
severe disease.
• Doses start at 15 mg/kg/day and are
increased by 5 mg/kg/day every 12 weeks
until marrow suppression is present.
• The suggested maximum dose is 35
mg/kg/day
25. • The goal of hydroxyurea is to achieve WBC count
between 5-8,000 WBCs/mm3 and suppression of
the granulocyte and reticulocyte counts.
• Hydroxyurea is a cytotoxic agent and has the
potential to cause life-threatening cytopenia.
• Other side effects include cutaneous
hyperpigmentation, alopecia, xerosis, nail
pigmentation, and leg ulcers.
• This drug should not be used in patients likely to
become
pregnant or those unwilling or unable to follow
instructions regarding treatment.
• Patients should be monitored for myelotoxicity.
26. Effect of Hydroxyurea on Mortality and Morbidity in
Adult Sickle Cell Anemia
• JAMA. 2003;289:1645-1651.
• 1.5 (5.8) deaths per 3-month period on HU vs
2.6 (7.9) deaths per 3 months for people off HU;
(P = .04)
• Increased Hgb F correlated with improved
survival
27. What effect has HU had on sickle
patients?
• In clinical trials, 44% decrease in hospitalizations,
40% decrease in mortality.
• But a review of records in MD before and after
HU approval for sickle, no change in
hospitalization rates or costs
• Lanzkron et al., Am J Heme, 2006
• Same group at JHU have surveyed care givers
and found less than half prescribed HU to all
eligible patients
28. Pain managements
• Management of acute painful episodes
consists of
– Exclusion of causes (infection),
– Hydration by oral or intravenous fluid ((D5 1/4 NS
) resuscitation, and
– Aggressive pain relief, including analgesics and
opiates.
29. 1. Simple transfusion – give blood
2. Partial exchange transfusion - remove blood
and give blood
3. Erythrocytapheresis – use apheresis to
maximize blood exchange
• When to use each method?
Transfusion in Sickle Cell
30. Simple transfusions should be used.
– In severely anemic patients or when
hemoglobin falls under 5 g/dL.
– if there is sufficient physiological derangement
to result in heart failure, dyspnea,
hypotension, or marked fatigue.
If the patient is stable and the reticulocyte count
high, transfusions can (and should) be deferred.
Transfusion in Sickle Cell
31. • Except in severe anemia, exchange transfusion
offers many benefits and is our first choice
• Packed cells are the blood product of choice.
• A post transfusion hematocrit of 30 to 36 % or
less is recommended.
• Avoid hyper-viscosity, which is dangerous to
sickle cell patients.
Transfusion in Sickle Cell
(exchange transfusion)
32. Exchange transfusion:
1. Bleed one unit (500 ml), infuse 500 ml of saline
2. Bleed a second unit and infuse two units.
3. Repeat. If the patient has a large blood mass,
do it again.
Transfusion in Sickle Cell
(exchange transfusion)
33. Transfusions usually fall into two categories:
1. Episodic, acute transfusions to stabilize or reverse
complications.
• Limited studies have shown that aggressive transfusion
(get hgb s < 30%) may help in sudden severe illness.
2. Long-term, prophylactic transfusions to prevent future
complications.
– Stroke
– Chronic debilitating pain
– Pulmonary hypertension
– Setting of renal failure and heart failure
Transfusion in Sickle Cell
(exchange transfusion)
34. New Treatments and Medicines
• Bone marrow transplants
• Gene therapy
• New medicine
– Butyric acid.
• This is a food additive that may increase normal
hemoglobin in the blood.
– Clotrimazole.
• This medicine helps prevent the loss of water from a
red blood cell and can keep the cell from turning into a
sickle cell.
– Nitric oxide.
• This may make sickle cells less sticky and keep blood
vessels open. People with sickle cell anemia have low
levels of nitric acid in their blood.
35. Prevention
Identify what can trigger the “Crisis”
such as stress, avoid extremes of
heat and cold weather, don’t travel
airplane that is not cabin
pressurized
Maintain healthy lifestyle habits
Eating healthy
Avoid dehydration
Exercise regularly
Get enough sleep and rest
Avoid alcohol and don’t smoke
Regular medical checkups and
treatment are important
36. Questions
1. In EPO deficiency RBC morphology is
A. Normocytic normochromic
B. Microcytic normochromic
C. Macrocytic normochromic
D. Microcytic hypochromic
36
37. A 55-yr-old patient with CKD undergoing dialysis
appears to be pale. A full blood count shows the
following red cell indices:
Hgb: 8.7 g/dL, Hct: 26% (low)
MCV: 92fL (NL: 80-100fL)
MCH: 33pg (NL:27-34pg)
MCHC: 33g/dL (NL: 32-36g/dL)
Reticulocyte count: 0.2% (NL: 0.5-1.5%)
2. Which of the following is the most appropriate
therapy?
A. Ferrous sulphate
B. Erythropoietin
C. Folic acid 37
38. 3. Bleeding disorders:
A. enhanced number/function of platelets
B. coagulation factor deficiency
C. decreased fibrinolysis
D. All
4. Which of the following is not true hemophilic
disorder?
A. Sons of a female carrier and a normal male have a
50% chance of having hemophilia
B. daughters a female carrier and a normal male have a
50% chance of being carriers.
C. Sons of a hemophilic father would be normal
D. Daughters a hemophilic father have a 50% chance of
being carriers.
39. A. B is a 15 years old patent who currently complain
Joint swelling and pain and erythema, Muscle and
intracranial hemorrhage and Hematuria. The
laboratory evaluation shows that factor VIII and IX
activity level is 0.3 &1.3 units/mL respectively. Titers of
inhibitors are measured and reported as 20 Bethesda
units (BU),
5. What type of disorder this patient have?
A. Vitamin k D deficiency
B. Hemophilia A
C. Hemophilia B
D. Sickle sell disease
40. 6. What subjective or objective are typical of for this
patient?
7. How should A.B.’s deficiency be managed? What
dose of should be given to treat A.B.’s deficiency?
A. Recombinant factor VIIa (rFVIIa),
B. Plasma-derived factor IV
C. Recombinant factor VIII
D. Desmo-pressin
8. Which of the following medicine helps to prevent the
loss of water from a red blood cell and can keep the
cell from turning into a sickle cell?
A. Butyric acid C. Nitric oxide
B. Clotrimazole D. Hydroquinoles