The human-WASH perspective: Considering animals in WASH
1.
The human-WASH healthperspective:
considering animals in WASH
Sophie Boisson
Water, Sanitation, Hygiene and Health Unit, WHO
boissons@who.int
2.
Water, Sanitation andHygiene
Safe drinking-water
Improving water sources,
household water treatment
and safe storage…
Sanitation
Separate human excreta from
human contact at all steps of the
sanitation service chain.
Hygiene: mostly hand washing
with soap at critical times,
sometimes broader MHM, food
hygiene, environmental hygiene…
3.
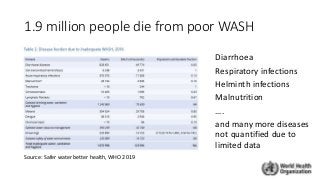
1.9 million peopledie from poor WASH
Diarrhoea
Respiratory infections
Helminth infections
Malnutrition
….
and many more diseases
not quantified due to
limited data
Source: Safer water better health, WHO 2019
4.
Recent WASH trialsfound no or little
impact on diarrhoea and child stunting
• 3 high quality RCTs
• WASH-B Kenya, Bangladesh
• SHINE Zimbabwe
• High-burden rural settings
• Interventions
• Household water chlorination
• Latrine improvements
• Handwashing with soap
• /+Nutrition
→ Why?
• Incomplete community coverage and use
• Continued exposure to animal & child faeces
• Poor food hygiene
• Lack of continuous water supply
• Limited effectiveness of chlorination against
key pathogens (cryptosporidium)
• Short timeframe
5.
How do thesefindings fit within wider body
of evidence?
• Systematic analysis of >1000 studies
• Overall protective effect of sanitation against many
infectious diseases and nutrition outcomes
• Limited increase in coverage and use leads to limited
impact on transmission
• Low quality evidence – mostly observational studies
• Significant gaps including on animal faeces and food
hygiene
6.
Exposure to humanfaeces
• 55% of the world’s population without safely managed sanitation services
• Over 2 billion lack basic sanitation services
• 673 million defecate in the open → Widespread
exposure to human
faeces and related
health risks
7.
Exposure to animalfaeces
• Worldwide, food animals produce 4 x more faecal matter than
humans (poultry, cattle and sheep…)
• In HIC, exposure via animal food productions...
• In LMIC, exposure in the domestic environment
50% of households in Southeast Asia and Africa have
domestic livestock
Livestock as source of livelihood and food → Health benefits
Close proximity between animals and humans→ Health risks
in household, community and beyond (food consumers)
Animal faeces –Healthrisks to humans?
• Systematic reviews suggest positive associations
between exposure to domestic livestock and health
(Zambrano 2014, Penakalapati 2017)
→ Diarrhoea, enteric pathogens, child growth etc.
• About 30% diarrhoeal deaths are caused by pathogens
that are known to be zoonotic (Delaroy 2018)
→ Campylobacter, NT Salmonella, Cryptosporidium, EPEC
• Many neglected zoonoses are linked to WASH (Matilla 2018)
→ Taenia/cysticercosis, Foodborne trematodiases,
Schistosomiasis, STH (e.g. Ascaris Sum)
• Antimicrobial resistance
1. Universal safetoilets that contain excreta
• Entire community coverage with a minimum level of
service
• Using demand side and supply side approaches
concurrently
• Shared/public if necessary to reach everyone
• All settings (schools, HCF, etc)
• Equitable progress
3. Coordination with local services
• Efficiency with other local services
(solid waste, transport, etc).
• Sustainability and health impacts through
coordination with other interventions,
water supply, hygiene, animal waste, child
faeces..
2. Safe sanitation chain
• Containment, transport, treatment, end use/disposal
• Context specific technologies and services
(i.e. technology agnostic)
• Incremental improvement based on local level risk
assessment (e.g. SSP)
• Protection of sanitation workers
4. Role of the health sector
• Increasing health sector engagement in core
functions (but not taking on functions that are
better done by others)
Coordinated sanitation interventions
Recommendations
12.
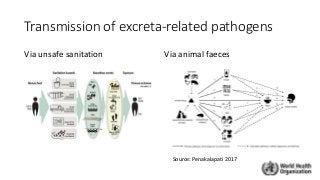
Risk assessment andmanagement
• Sanitation safety planning/
Water safety planning
• Sanitary inspections
• Sanitation facilities
• Small community water supplies
→ SI forms can be adapted to include
health risks from exposure to animal
waste
Strengthening the evidence
•Measuring exposure to animal faeces
• Quantifying related health risks
• Understanding pathogen biology
• Identifying effective interventions and how
best to deliver them across sectors
15.
Take away messages
•In LMIC, animal faeces in domestic environment expose young
children to diarrhoea, enteric infections, growth impairment etc. →
BUT are not typically addressed by WASH/sanitation sector
• Complex transmission pathways, depend on behaviours → need to
better understand related health risks and effective interventions
• One health needed: cross-sectoral action at national and district level
for health risk-based prioritization and coordination of interventions