1. Articles
www.thelancet.com Vol 367 May 13, 2006 1577
Aminophylline in bradyasystolic cardiac arrest: a randomised
placebo-controlled trial
Riyad B Abu-Laban, Caroline M McIntyre, James M Christenson, Catherina A van Beek, Grant D Innes, Robin K O’Brien, Karen PWanger,
R Douglas McKnight, Kenneth G Gin, Peter J Zed, JeffreyWatts, Joe Puskaric, Iain A MacPhail, Ross G Berringer, Ruth A Milner
Summary
Background Endogenous adenosine might cause or perpetuate bradyasystole. Our aim was to determine whether
aminophylline, an adenosine antagonist, increases the rate of return of spontaneous circulation (ROSC) after out-of-
hospital cardiac arrest.
Methods In a double-blind trial, we randomly assigned 971 patients older than 16 years with asystole or pulseless
electrical activity at fewer than 60 beats per minute, and who were unresponsive to initial treatment with epinephrine
and atropine, to receive intravenous aminophylline (250 mg, and an additional 250 mg if necessary) (n=486) or
placebo (n=485). The patients were enrolled between January, 2001 and September, 2003, from 1886 people who had
had cardiac arrests. Standard resuscitation measures were used for at least 10 mins after the study drug was
administered. Analysis was by intention-to-treat. This trial is registered with the ClinicalTrials.gov registry with the
number NCT00312273.
Findings Baseline characteristics and survival predictors were similar in both groups. The median time from the
arrival of the advanced life-support paramedic team to study drug administration was 13 min. The proportion of
patients who had an ROSC was 24·5% in the aminophylline group and 23·7% in the placebo group (difference 0·8%;
95% CI –4·6% to 6·2%; p=0·778). The proportion of patients with non-sinus tachyarrhythmias after study drug
administration was 34·6% in the aminophylline group and 26·2% in the placebo group (p=0·004). Survival to hospital
admission and survival to hospital discharge were not significantly different between the groups. A multivariate
logistic regression analysis showed no evidence of a significant subgroup or interactive effect from aminophylline.
Interpretation Although aminophylline increases non-sinus tachyarrhythmias, we noted no evidence that it
significantly increases the proportion of patients who achieve ROSC after bradyasystolic cardiac arrest.
Introduction
Out-of-hospital sudden cardiac arrest treated by
emergency medical services has an estimated incidence
of 55 per 100000 person-years, which translates to about
155000 episodes annually in the USA.1
Bradyasystole is
the first recorded rhythm in up to 52% of cardiacarrests,
and many additional patients with an initial cardiac arrest
rhythm of ventricular fibrillation deteriorate to
bradyasystole after defibrillation efforts.2,3
Fewer than 3%
of patients presenting with bradyasystole survive to
hospital discharge; however, more than 17% of all cardiac
arrest survivors had initial bradyasystole.4
Thus, even a
small improvement in survival from bradyasystolic
cardiac arrest could save thousands of lives.
Adenosine is an endogenous purine nucleoside that
depresses the sinoatrial node, blocks atrioventricular
conduction, inhibits the pacemaker activity of the His-
Purkinje system, and attenuates the effects of
catecholamines.5–12
Since adenosine is produced and
released by myocardial cells during ischaemia and
hypoxia,13,14
it might be a reversible factor in the aetiology
or perpetuation of bradyasystole.15
Aminophylline is a
competitive antagonist of adenosine. The use of
aminophylline for bradycardia and heart block has been
described, and several anecdotal reports and small
studies have been published on its use in cardiac
arrest.16–24
We undertook this study to assess the effect of
aminophylline during cardiopulmonary resuscitation
(CPR) of patients with out-of-hospital bradyasystolic
cardiac arrest unresponsive to initial therapy.
Methods
We undertook this trial between Jan 21, 2001, and Sept 3,
2003, at eight advanced life-support paramedic stations
in the greater Vancouver and Chilliwack region in
Canada. This region has a population of more than two
million, served by the British Columbia Ambulance
Service. Out-of-hospital cardiacarrest patients are treated
by paramedics with protocols based on American Heart
Association guidelines,25
and are not taken to hospital
unless a perfusing rhythm develops, a shockablerhythm
persists, or there are extenuating circumstances such as
hypothermia or intermittently palpable pulses.
Patients and procedures
Cardiac arrest patients who were older than 16 years were
eligible if they had bradyasystole at any time during
resuscitation efforts, and at the time of study drug
initiation. Bradyasystolewas defined as an absent cardiac
rhythm (asystole), or an organised non-perfusing cardiac
rhythm (pulseless electrical activity) at a rate lower than
60 beats per minute.26
Before enrolment, all patients
Lancet 2006; 367: 1577–84
University of British Columbia,
Vancouver, BC, Canada
(R B Abu-Laban MD,
C M McIntyre MD,
Prof J M Christenson MD,
C A van Beek BSN,
Prof G D Innes MD,
R K O’Brien PharmD,
K PWanger MD,
R D McKnight MD, K G Gin MD,
P J Zed PharmD, I A MacPhail MD,
R G Berringer MD,
R A Milner MSc); British
Columbia Ambulance Service,
Victoria, BC, Canada
(J M Christenson,
K PWanger, JWatts EMA-3,
J Puskaric EMA-3); and Centre
for Clinical Epidemiology and
Evaluation,Vancouver, BC,
Canada (R B Abu-Laban,
C A van Beek, R A Milner)
Correspondence to:
Dr Riyad B Abu-Laban,
Department of Emergency
Medicine,Vancouver General
Hospital,Vancouver,
BCV5Z 1M9, Canada
abulaban@interchange.ubc.ca
2. Articles
1578 www.thelancet.com Vol 367 May 13, 2006
underwent endotracheal intubation, received ventilation
with 100% oxygen, and were given 3 mg of atropine and
1 mg of epinephrine intravenously.
Exclusion criteria were: a do-not-resuscitate directive;
pregnancy; evidence of haemorrhage, trauma or
hypothermia as a cause of cardiac arrest; renal dialysis;
theophylline hypersensitivity; or patients taking an oral
theophylline product. In addition, according to local
educational requirements, resuscitations directed by a
paramedic student under practicum supervision were
ineligible for enrolment and thus excluded.
All paramedics were trained in the protocol and
procedures before the study launch. All patients received
standard care as stipulated by regional cardiac arrest
protocols, which require that patients with asystole
receive 3 mg of atropine as a single bolus and patients
with bradycardic pulseless electrical activity receive
atropine in two 1·5 mg boluses given 2–3 min apart.
Eligible patients received treatment with a drug kit
randomised to contain either two 10 mL ampoules of
normal saline placebo or two 10 mL ampoules each
containing 250 mg of aminophylline (prepared under
contract by Abbott Laboratories, Saint-Laurent, QC,
Canada). Randomisation was done by computer.
Study drug kits were given to each ambulance station
in batches of eight, and carried on ambulances in batches
of two, with restocking as needed. The aminophyllineand
placebo ampoules were indistinguishable in appearance.
The first ampoule was given as an intravenous bolus
followed by a 10 mL intravenous flush of normal saline.
If the patient remained pulseless and in bradyasystole
after 90 s of CPR, the second ampoule was given in an
identical manner, resulting in a dose of either one or two
ampoules of placebo, or 250 mg or 500 mg of
aminophylline. Resuscitation efforts were continued fora
minimum of 10 mins after the last dose, and further
treatment was at the discretion of the paramedic
resuscitation leader. All treatment and investigations in
1886 cardiac arrests treated by
emergency medical services
January, 2001–September, 2003
971 randomised
1025 eligible
486 randomised to
aminophylline
485 randomised to
placebo
441 had treatment
according to
protocol
432 had treatment
according to
protocol
45 had treatment that
violated protocol
53 had treatment that
violated protocol
486 included in
intention-to-treat
analysis
485 included in
intention-to-treat
analysis
78 missed because of
paramedics’ omission
837 excluded on basis
of non-eligibility
861 not eligible
947 enrolled 24 enrolled in error
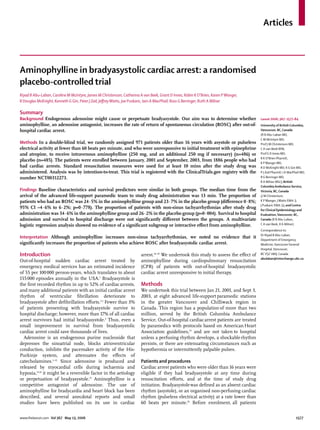
Figure:Trial profile
*178 additional patients during the study period had clear signs of death and no resuscitation attempted by
paramedics.
Aminophylline
(n=486)
Placebo
(n=485)
Age (years)
Mean (SD) 65·4 (17·4) 65·8 (17·6)
Range 18–100 18–107
Sex
Female 128 (26·3%) 149 (30·7%)
Male 358 (73·7%) 336 (69·3%)
Estimated weight (kilograms)
Unknown 36 (7·4%) 35 (7·2%)
<40 5 (1·0%) 4 (0·8%)
40–60 94 (19·3%) 80 (16·5%)
61–80 207 (42·6%) 225 (46·4%)
>80 144 (29·6%) 141 (29·1%)
Incident setting
Home 346 (71·2%) 355 (73·2%)
Workplace 11 (2·3%) 7 (1·4%)
Airport 2 (0·4%) 3 (0·6%)
In transit or automobile 8 (1·6%) 10 (2·1%)
Recreation 9 (1·9%) 12 (2·5%)
Street 14 (2·9%) 15 (3·1%)
Long-term care facility 6 (1·2%) 9 (1·9%)
Other 90 (18·5%) 74 (15·3%)
Medical history*
Stroke or transient ischaemic attack 37 (7·6%) 27 (5·6%)
Previous cardiac arrest 1 (0·2%) 5 (1·0%)
Previous myocardial infarction 75 (15·4%) 78 (16·1%)
Angina or coronary artery disease 122 (25·1%) 125 (25·8%)
Congestive heart failure 47 (9·7%) 59 (12·2%)
Dysrhythmia 30 (6·2%) 36 (7·4%)
Hypertension 109 (22·4%) 121 (24·9%)
Peripheral vascular disease 7 (1·4%) 3 (0·6%)
Diabetes 97 (20·0%) 97 (20·0%)
Renal disease 6 (1·2%) 11 (2·3%)
Respiratory disease 57 (11·7%) 52 (10·7%)
Cancer 34 (7·0%) 35 (7·2%)
Seizures 8 (1·6%) 8 (1·6%)
Gastrointestinal disease 12 (2·5%) 25 (5·2%)
Other 135 (27·8%) 128 (26·4%)
No history of disease 43 (8·8%) 60 (12·4%)
(Continues on next page)
3. Articles
www.thelancet.com Vol 367 May 13, 2006 1579
survivorsto hospital were at the discretion of the attending
physician. Physicians could request that blinding of
treatment be suspended if a patient’s subsequent care
required knowledge of whether or not they received
aminophylline or placebo. Except for such cases, study
personnel and investigators, caregivers, patients, and
their families remained blinded throughout the study
period.
All cardiac arrests in the region were tracked during
the study period. The paramedic resuscitation leader
completed a questionnaire about each patient with
cardiac arrest and bradyasystole to document eligibility
and enrolment or reasons for exclusion. Further
informationwas obtained from the ambulance or hospital
records. Patients who survived to hospital admission
began to be monitored by a research coordinator by not
more than 1 day afteradmission.
All outcomes were defined beforehand, and applicable
data were collected according to the Utstein style.27
The
primary outcome was return of spontaneous circulation
(ROSC), defined as the development of a palpable pulse
of any duration. Secondary outcomes were maximum
duration of ROSC (the duration of the longest episode of
sustained pulse return), ROSC duration by survival
analysis,28
survival to hospital admission, survival to
hospital discharge, length of hospital stay, non-sinus
tachyarrhythmias in the first 24 h after treatment, seizures
in the first 24 h after treatment, and neurological outcome.
Neurological outcome was assessed with four validated
scales: the Glasgow Coma Scale,29
the Glasgow-Pittsburgh
Cerebral and Overall PerformanceScales,30,31
the Modified
Mini-Mental State Examination,32
and the Functional
StatusQuestionnaire.33
Additionaloutcomes,prespecified
for hypothesis-generating analyses, were the proportion
of patients receiving one dose of the drug compared with
those given two doses, and the proportion of patients
achieving ROSC with initial-rhythm bradyasystole
compared with those who had bradyasystole that
developed after the arrival of advanced life-support
paramedics. Survivors were followed-up for 1 year after
hospital discharge.
The study was overseen by an independent data and
safety monitoring board, whose members were aware of
the patients’ treatment assignments. Approval was
obtained from the institutional review board of the
University of British Columbia, the research ethics
committees of the receiving hospitals, and the British
Columbia Ambulance Service. As in other cardiac arrest
research in this region,34
the study was conducted
according to a policy of presumed consent.35
Survivors
with ROSC of at least 24 h or their proxy decision makers
were notified of enrolment, usually within 2 days of
admission to hospital, and written informedconsent was
obtained for follow-up data collection.
Statistical analysis
Based on a pilot study of bradyasystolic cardiac arrest
cases in the study region, we estimated the baseline
ROSC proportion in the study population to be 29·2%.
Evidence available at the time the study was designed
suggested a relative improvement in the proportion of
ROSC with aminophylline of about 50%.16,19,21
Since small
early reports frequently overestimate treatment effects,
we assumed a relative improvement in the proportion of
ROSC of 30%, which would translate to an absolute
improvement of 8·8%. The study was therefore designed
with 80% power to detect this absolute increase from
29·2% to 38·0%. Before the study started, we established
that the data for patients in the aminophylline group,
irrespective of whether they were given one or two doses,
(Continued from previous page)
Home medications (specific or class)*
ACE (angiotensin converting enzyme)
inhibitor
114 (23·4%) 105 (21·6%)
β blocker 65 (13·4%) 76 (15·7%)
Lipid lowering agents 65 (13·4%) 63 (13·0%)
Antiarrhythmic therapy 41 (8·4%) 32 (6·6%)
Calcium channel blocker 62 (12·8%) 51 (10·5%)
Nitrates 64 (13·2%) 59 (12·2%)
Coumadin 15 (3·1%) 16 (3·3%)
Digitalis 52 (10·7%) 45 (9·3%)
Aspirin 45 (9·3%) 55 (11·3%)
Diuretic 101 (20·8%) 120 (24·7%)
Cancer 1 (0·2%) 5 (1·0%)
Diabetes 69 (14·2%) 66 (13·6%)
Gastrointestinal 41 (8·4%) 58 (12·0%)
Renal 0 (0·0%) 1 (0·2%)
Respiratory 46 (9·5%) 47 (9·7%)
Anti-epileptic 12 (2·5%) 13 (2·7%)
Other non-cardiac 189 (38·9%) 208 (42·9%)
No home medications 55 (11·3%) 65 (13·4%)
Data are number (%) unless otherwise specified. *As documented by paramedics (in
about 15% of cases, information on these variables was unavailable).
Table 1: Baseline characteristics of participants
Aminophylline (n=486) Placebo (n=485)
Witnessed collapse 202 (41·6%) 184 (37·9%)
Bystander compression 135 (27·8%) 156 (32·2%)
Bystander ventilation 135 (27·8%) 165 (34·0%)
Automated external defibrillator shockable*† 100 (20·6%) 89 (18·4%)
Initial rhythm on arrival of advanced life-support paramedics
Asystole 305 (62·8%) 297 (61·2%)
Pulseless electrical activity <60 per min 99 (20·4%) 92 (19·0%)
Pulseless electrical activity ≥60 per min 14 (2·9%) 17 (3·5%)
Ventricular fibrillation† 66 (13·6%) 78 (16·1%)
Ventricular tachycardia† 1 (0·2%) 1 (0·2%)
Unknown 1 (0·2%) 0 (0·0%)
Data are number (%). *When first responders arrived before advanced life-support paramedics; †265 (27·3%) patients (133 in the
aminophylline group, 132 in the placebo group) had a shockable rhythm on initial encounter, either by automated external
defibrillator or by initial rhythm interpretation by advanced life-support paramedics.
Table 2: Predictors of survival
4. Articles
1580 www.thelancet.com Vol 367 May 13, 2006
would be pooled for the primary comparison against the
placebo.
We planned an interim analysis at the halfway
enrolment point, and applied the O’Brien-Fleming
procedure for atwo-stage design, in which the significance
level for the final analysis of the primary outcome was
0·048 or lower.36
A two-sided sample size calculation,
based on an alpha level of 4·8%, showedthat 966 patients
needed to be enrolled. Outcomes were assessed with the
χ² test forproportions, Fisher’s exact t test, the Wilcoxon
rank-sum test, or the log-rank test as appropriate. We
assessed ROSC duration by survival analysis with a
Kaplan-Meier analysis of time to loss of ROSC, censoring
survivors to discharge at the point of death of all non-
survivors to discharge.28
In addition, for secondary
analysis a logistic regression was planned a priori to
allow multivariate assessment of factors associated with
achievement of ROSC. For secondary outcomes, p≤0·05
was judged significant. Analyses were by intention to
treat,and all statistical tests were two-sided.
This trial is registered with the ClinicalTrials.gov registry
with the number NCT00312273.
Role of the funding source
This study was supported by a grant-in-aid from the Heart
and Stroke Foundation of British Columbia and Yukon,
with additional support from the Vancouver Coastal
Health Research Institute. The study sponsors had no role
inthestudydesign,thecollection,analysisorinterpretation
of data, the writing of the report, or the decision to submit
the paper for publication. The corresponding author had
full access to all the data in the study and had final
responsibility to submit for publication.
Results
During the study, CPR was done in 1886 adults, 1025 of
whom were eligible (figure). 971 patients were enrolled
(486 aminophylline, 485 placebo): 947 (92·4%) of these
were eligible and 24 non-eligible (12 of whom received
aminophylline and 12 of whom received placebo). The
non-eligible patients often had more than one reason
their enrolment was inappropriate; the most common
reasons were non-administration of epinephrine
(23 cases) or administration of less than 3 mg of atropine
(18 cases). 78 eligible patients were not enrolled because
of forgetfulness of the treating paramedics. Blinding was
suspended in five cases (four by a treating physician and
one by a coroner), three in the aminophyline group and
two in the placebo group, and two unblinded patients
received non-study aminophylline during further
resuscitative efforts in the emergency department. There
were no survivors to hospital discharge in the unblinded
group.
The cause of arrest, presumed by the paramedic, was
cardiac in 799 (82·3%) cases and drug overdose in 80
(8·2%). Baseline patient characteristics were similar in
both groups (table 1). Cardiac arrest variables predictive
of survival were also similar in the two groups, with the
exception of a slightly higher proportion of bystander
CPR in the placebo group (table 2). The mean time from
first atropine dose to study drug was 7 min (median
6 min). There were 98 protocol violations (45 in the
aminophylline group and 53 in the placebo group). In
87 (89%) of these, resuscitation after giving the study
drug lasted for less than 10 min; the mean post study
resuscitation duration in these 87 patients was 7·1 min
(range 1–9) (median 6 min). Table 3 outlines the
medications given during CPR. 166 (17·1%) patients
received transcutaneous pacing. Table 4 provides an
overview of the critical steps in resuscitation sequence
and the timing of these steps, indicating the point at
which patients received aminophylline or placebo.
Primary and secondary outcomes are summarised in
table 5. 456 (93·8%) patients in the aminophylline group
received both doses of study drug, resulting in a total
aminophylline dose of 500 mg. In the aminophylline
group, 119 patients (24·5%) achieved ROSC compared
Aminophylline (n=486) Placebo (n=485)
Epinephrine 486 (100·0%) 485 (100·0%)
Atropine 485 (99·8%) 484 (99·8%)
Sodium bicarbonate 232 (47·7%) 251 (51·8%)
Lidocaine 119 (24·4%) 97 (20·0%)
Procainamide 12 (2·5%) 5 (1·0%)
Calcium 28 (5·8%) 24 (4·9%)
Magnesium 27 (5·6%) 12 (2·5%)
Amiodarone 2 (0·4%) 0 (0·0%)
Dextrose 139 (28·6%) 135 (27·8%)
Thiamine 66 (13·6%) 64 (13·2%)
Naloxone 79 (16·3%) 74 (15·3%)
Data are number (%).
Table 3: Medications given during cardiac arrest resuscitation
Aminophylline (n=486) Placebo (n=485) Both groups (n=971)
Collapse* to start CPR 4·8 (4·0) 4·9 (4·0) 4·8 (4·0)
Collapse* to ALS call received 4·5 (4·0) 5·0 (4·0) 4·7 (4·0)
ALS call received to ALS at
patient side
8·9 (8·0) 9·3 (9·0) 9·1 (8·0)
ALS arrival at patient side to
first epinephrine dose
4·2 (4·0) 4·1 (4·0) 5·1 (4·0)
ALS arrival at patient side to
qualifying bradyasystole
1·4 (0·0) 1·8 (0·0) 1·6 (0·0)
ALS arrival at patient side to
study drug dose 1
14·5 (13·0) 14·8 (13·0) 14·6 (13·0)
Study drug dose 1 to study
drug dose 2
2·4 (2·0) 3·4 (2·0) 2·9 (2·0)
Last dose study drug to ROSC 7·3 (0·0) 2·9 (0·0) 5·1 (0·0)
Start CPR to ROSC 36·5 (29·0) 33·2 (29·0) 34·9 (29·0)
Last dose study drug to death
at scene
26·5 (25·0) 33·9 (18·0) 29·9 (20·0)
Data are mean in min (median). ALS=advanced life-support. *Estimated in witnessed arrests only.
Table 4: Duration of critical steps in resuscitation sequence
5. Articles
www.thelancet.com Vol 367 May 13, 2006 1581
with 115 patients (23·7%) in the placebo group (difference
0·8%; 95% CI –4·6 to 6·2; p=0·778). The median
maximum duration of ROSC, excluding survivors to
discharge, was 17 min (mean 717 min) in the
aminophylline group and 27 min (2341 min) in the
placebo group (p=0·418). The survival analysis of ROSC
duration showed a statistically insignificant curve
separation favouring the placebo group (p=0·58), and a
mean survival in the aminophylline and placebo groups
of 19763 min (median 32 min) and 29970 min (41 min),
respectively.
32 aminophylline recipients (6·6%) and 37 placebo
recipients(7·6%)survivedtohospitaladmission(p=0·527),
and two aminophyllline recipients (0·5%) and three
placebo recipients (0·6%) survived to hospital discharge
(p=0·653). Three of the five who survived to discharge had
asystole on advanced life-support paramedic arrival (two
of whom had an automated external defibrillator shock
administered by first responders, and received placebo);
the other two survivors had ventricular fibrillation on
advanced life-support paramedic arrival (one received
placebo and the other aminophylline, and neither had
previouslyhadanautomatedexternaldefibrillatorapplied).
The fifth survivor received aminophylline. All five
survivors to hospital discharge had excellent neurological
and functional outcomes: three had cerebral and overall
performance scores of 1 at 1 year; one was “walking and
talking” at 1 year, according to his family, but had moved
residence and could not be assessed; and one individual
had cerebral and overall performance scores of 1 on
hospital discharge but refused follow-up.
The proportion of patients with non-sinus
tachyarrhthmias within 24 h of study drug administration
was 168 (34·6%) in the aminophylline group compared
with 127 (26·2%) in the placebo group (p=0·004). Most of
these tachyarrhythmias were episodes of ventricular
fibrillation or ventricular tachycardia occurring shortly
after study drug administration. The mean time from first
dose of study drug to first episode of tachyarrhythmia in
the aminophylline group was 7·1 min (median 5 min).
Logistic regression modeling, with ROSC as the
dependant variable, fit the following pre-specified
covariates: age; sex; witnessed arrest; bystander CPR;
initial rhythm on advanced life-support paramedic
arrival; estimated patient weight; bradyasystole on
advanced life-support paramedic arrival versus
Aminophylline (n=486) Placebo (n=485) Difference (95% CI) p
Overall who achieved ROSC 119 (24·5%) 115 (23·7%) 0·8% (–4·6 to 6·2) 0·778
ROSC after first dose 30 (6·1%) 27 (5·6%) 0·5% (–2·4 to 3·6) 0·688
ROSC after second dose 92 (18·9%) 92 (18·9%) 0·0% (–4·9 to 4·9) 0·998
ROSC after both doses 3 (0·6%) 4 (0·8%) –0·2% (–1·2 to 0·6) 0·703
First rhythm bradyasystole with ROSC 96 (80·7%) 87 (75·7%) 5·0% (–5·6 to 15·7) 0·355
Later rhythm bradyasystole with ROSC 23 (19·3%) 28 (24·3%) –5·0% (–15·7 to 5·6) 0·355
Prehospital death 374 (77·0%) 380 (78·4%) –1·4% (–6·6 to 3·8) 0·602
Transport to hospital 112 (23·0%) 105 (21·6%) 1·6% (–3·9 to 6·6) 0·602
Arrival to hospital with pulse 66 (13·6%) 63 (13·0%) 0·6% (–3·7 to 4·9) 0·787
Arrival to hospital without pulse 46 (9·5%) 42 (8·7%) 0·8% (–2·8 to 4·4) 0·661
Survival to hospital admission 32 (6·6%) 37 (7·6%) –1·0% (–4·3 to 2·2) 0·527
Seizures <24 h post study drug 8 (1·6%) 4 (0·8%) 0·8% (–0·6 to 2·2) 0·247
Nonsinus tachyarrhythmias <24 h post study drug 168 (34·6%) 127 (26·2%) 8·4% (2·6 to 14·2) 0·004
Maximum ROSC duration in mins*; median (mean) 17 (717) 27 (2341) –10 (–52 to 32) 0·418
Length of hospital stay in days; median (mean) 0·0 (6·5) 2·0 (10·6) –2·0 (–5·4 to 1·6) 0·291
Length of hospital stay for survivors in days; median (mean) 12·5(12·5) 27·0 (27·0) –15·0 (–21·0 to –8·0) 0·011
Length of hospital stay for non–survivors in days; median (mean) 6·1 (1·0) 9·6 (2·0) –3·5 (–14·9 to 7·8) 0·534
Survival to hospital discharge 2 (0·4%) 3 (0·6) –0·2% (–1·1 to 0·7) 0·653
Data are number (%) unless otherwise specified. *Excludes survivors to hospital discharge.
Table 5: Outcomes
Odds ratio (95% CI)
Age 1·01 (1·00–1·02)
Being female 1·56 (1·03–2·35)
Witnessed cardiac arrest 1·62 (1·13–2·32)
Bystander CPR 1·00 (0·68–1·46)
Initial cardiac rhythm* 1·49 (0·94–2·37)
Estimated patient weight†
60–80 kilograms 1·05 (0·64–1·74)
>80 kilograms 1·27 (0·73–2·19)
Initial (vs subsequent) bradyasystole 1·09 (0·70–1·72)
Time from call received to study drug 0·99 (0·97–1·01)
Study drug allocation 1·12 (0·80–1·59)
*The odds ratio represents the estimate for pooled ventricular fibrillation and pulseless
ventricular tachycardia; the comparison group was all other cardiac arrest rhythms
(predominately bradyasystole). †Paramedic-estimated weight on a categorical scale; the
comparison group was weight lower than 60 kg.
Table 6: Effect estimates for prespecified covariates in logistic
regression model
6. Articles
1582 www.thelancet.com Vol 367 May 13, 2006
bradyasystole that developed subsequently; time from
call received to study drug administration; and study
drug allocation (table 6). There was no evidence of a
subgroup or interactive effect from aminophylline, and
this analysis identified only whether an arrest was
witnessed (odds ratio 1·62, 95% CI 1·13–2·32) and being
female (1·56, 1·03–2·35) to be significant independent
predictors of ROSC.
Discussion
In this randomised, double-blind, placebo-controlled trial
of out-of-hospital bradyasystolic cardiac arrest, we
identified no evidence that aminophylline significantly
increases the proportion of patients who achieve ROSC.
Our 95% CI reliably excludes an absolute aminophylline-
related increase in the proportion of ROSC of more than
6·2%. Moreover, we found no suggestion of an increase
in survival to hospital admission or survival to hospital
discharge from aminophylline in the population we
studied.
Interest in aminophylline for bradyasystolic cardiac
arrest was ignited after the 1993 publication of a
consecutive case series of 15 cardiac arrest patients, 11 of
whom developed a “stable heart rhythm within 30 s of
aminophylline administration” and remained alive for at
least 1 h.16
Three subsequent clinical trials that were well-
done but small suggested the possibility of a treatment
effect on ROSC,19,21,24
however, the low statistical power of
these studies precluded determination of whether a
benefit actually existed.
Our findings fall within the wide 95% CIs for ROSC of
these previous clinical trials. Notably, neither our study,
nor the previous trials, were designed or powered to
detect an effect from aminophylline on survival to
hospital discharge. Given the low baseline survival rate
from bradyasystole, this would require a study of many
thousands of patients. The decision to use ROSC as a
primary outcome in preliminary cardiac arrest studies,
although common, is predicated on the assumption that
there is a link between ROSC (as a “predictor” of a
clinically relevant treatment effect) and survival to
hospital discharge (if a survival benefit actually exists).
This assumption has never been proven, and different
commonly reported ROSC definitions lead to strikingly
different treatment effect estimates.28
Our finding of a significant 8·4% absolute increase in
non-sinus tachyarrhythmias after aminophylline
administrationsuggeststhisdrugdoeshavecardiovascular
effects in the setting of cardiac arrest. These effects could
account for the higher rate of “reversal of asystole” reported
in a previous study that also failed to find a significant
increase in ROSC.24
Whether this finding provides any
encouragement that a meaningful treatment effect from
aminophylline exists in some subgroups is unclear.
Our study has some limitations. In keeping with
previous reports, we chose to administer aminophylline
after epinephrine and atropine, thus our results are not
generalisable to a different sequence of medication
administration. Although it is possible that a beneficial
effect from aminophylline was negated by the presence
of epinephrine and atropine, or the time delay arising
from the administration of these drugs, the sequence we
used was identical to that which preliminary research
suggested could be efficacious. The possibility of giving
aminophylline as the first drug to eligible patients was
carefully considered during the design of the study, but
rejected because such an approach was inconsistent with
the available evidence, and because a proposal to
administer an investigational drug before standard
recommended therapy would probably have been
unacceptable to the medical community and might have
been deemed unethical.
The median time from paramedic arrival to study
drug administration was 13 min, a delay in large part
due to our stipulation of administering standard
treatment before the study drug, and because not all
enrolled patients were initially in an eligible cardiac
rhythm. This time delay was anticipated from knowledge
of the various steps that paramedics needed to take
before they could adminster the study drug. Although
the timing of study drug delivery in our trial is consistent
with previous reports, it is conceivable that giving
aminophylline to patients earlier might have led to
different results. We administered aminophylline at an
initial dose of 250 mg because previous reports
suggested this dose was potentially efficacious. Since
the pharmacokinetics of aminophylline during cardiac
arrest are not known, and a wide dosing range of this
drug has been used in other settings, we incorporated a
second 250 mg aminophylline dose in our treatment
protocol if bradyasystole was persistent after 90 s. Such
an approach is similar to the medication administration
recommendations for many drugs during cardiac
arrest.25
Our results are not generalisable to the combined use
of aminophylline with other agents that could be
promising treatments for bradyasystole, such as
vasopressin,37
or to the use of other methylxanthines or
“pure”adenosineantagonistsratherthanaminophylline.38
Moreover, patients with bradyasystole represent a
heterogeneous population, and it is possible that our
study failed to detect a beneficial effect within a specific
patient subgroup. Finally, as with all cardiac arrest studies
of medications, the maintenance of potentially viable
vital organs is an important issue. If support of circulation
with CPR is not sufficient, medications arriving to the
heart might be ineffective even if they would be beneficial
in viable tissue. Recent evidence suggests that common
CPR practices may provide suboptimal blood flow
because of inappropriately rapid ventilation rates and
pauses in chest compressions.39,40
We did not control or
assess the quality of CPR in this study, and it is possible
that aminophylline administered in a setting with
optimised CPR could result in different findings.
7. Articles
www.thelancet.com Vol 367 May 13, 2006 1583
Although our study does not eliminate the possibility
that aminophylline could benefit some patients who have
had cardiac arrest, our results indicate that use of amino-
phylline in bradyasystolic cardiac arrest unresponsive to
initial interventions does not significantly increase the
proportion of patients who achieve ROSC. Thus, we do
not recommend the routine addition of aminophylline to
current treatment for bradyasystolic cardiac arrest.
Contributors
R B Abu-Laban conceived of the study and was the principal investigator.
R B Abu-Laban, C M McIntyre, J M Christenson, C A van Beek,
G D Innes, R O’Brien, K P Wanger, R D McKnight, K G Gin, J Watts,
and I A MacPhail designed and sought funding for the study.
C A van Beek was responsible for overall study coordination. P J Zed
oversaw all aspects of the study drug preparation and distribution.
J Puskaric led the interaction and communication between the study
coordinating office and the paramedic base stations. R A Milner was the
study statistician. All authors participated in the implementation and
execution of the study, and in the analysis and interpretation of the data.
R B Abu-Laban and C M McIntyre drafted the manuscript, which all
authors subsequently reviewed, edited and approved.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgments
R B Abu-Laban is supported by a Clinical Scholar Award from the
Michael Smith Foundation for Health Research. We thank
Bernie Bressler, Howard Bright, Jan Buchanan, Keith Chambers,
Chris Evans, Mark Fitzgerald, Sue Goguen, Peter Jewesson,
David Jung, Lisa Kuramoto, Charlie Kerr, Tim Mader, Roy Purssell,
Michael Schultzer, Michael Shuster, Carol Shaben, Joel Singer,
Chuck Sun, and Don Zarowny for their support and contributions; and
the paramedics of the British Columbia Ambulance Service, whose
dedication to excellence in both patient care and research made this
study possible.
References
1 Rea TD, Eisenberg MS, Sinibaldi G, White RD. Incidence of EMS-
treated out-of-hospital cardiac arrest in the United States.
Resuscitation 2004; 63: 17–24.
2 Herlitz J, Ekstrom L, Wennerblom B, Axelsson A, Bang A,
Holmberg S. Predictors of early and late survival after out-of-
hospital cardiac arrest in which asystole was the first recorded
arrhythmia on scene. Resuscitation 1994; 28: 27–36.
3 Sedgwick ML, Dalziel K, Watson J, Carrington DJ, Cobbe SM. The
causative rhythm in out-of-hospital cardiac arrests witnessed by the
emergency medical services in the Heartstart Scotland Project.
Resuscitation 1994; 27: 55–59.
4 Pepe PE, Levine RL, Fromm RE Jr, Curka PA, Zachariah BS.
Cardiac arrest presenting with rhythms other than ventricular
fibrillation: contribution of resuscitative efforts toward total
survivorship. Crit Care Med 1993; 21: 1838–43.
5 Malcolm AD, Garratt CJ, Camm AJ. The therapeutic and diagnostic
cardiac electrophysiological uses of adenosine.
Cardiovasc Drugs Ther 1993; 7: 139–147.
6 Pelleg A, Hurt C, Miyagawa A, Michelson EL, Dreifus LS.
Differential sensitivity of cardiac pacemakers to exogenous
adenosine in vivo. Am J Physiol 1990; 258: 1815–22.
7 DiMarco JP, Sellers TD, Lerman BB, Greenberg ML, Berne RM,
Belardinelli L. Diagnostic and therapeutic use of adenosine in
patients with supraventricular tachyarrhythmias. J Am Coll Cardiol
1985; 6: 417–25.
8 Favale S, DiBiase M, Rizzo U, Belardinelli L, Rizzon P. Effect of
adenosine and adenosine-5’-triphosphate on atrioventricular
conduction in patients. J Am Coll Cardiol 1985; 5: 1212–19.
9 Urthaler F, James TN. Effects of adenosine and ATP on AV
conduction and on AV junctional rhythm. J Lab Clin Med 1972; 79:
96–105.
10 Dobson JG Jr. Mechanism of adenosine inhibition of
catecholamine-induced responses in the heart. Circ Res 1983; 52:
151–60.
11 Dobson JG Jr. Adenosine reduces catecholamine contractile
response in oxygenated and hypoxic atria. Am J Physiol 1983; 245:
468–74.
12 Schrader J, Baumann G, Gerlach E. Adenosine as inhibitor of
myocardial effects of catecholamines. Pflügers Arch 1977; 372: 29–35.
13 Berne RM. Cardiac nucleotides in hypoxia: possible role in
regulation of coronary blood flow. Am J Physiol 1963;
204: 317–22.
14 Bardenheuer H, Schrader J. Supply-to-demand ratio for oxygen
determines formation of adenosine by the heart. Am J Physiol 1986;
250: 173–80.
15 Mader TJ, Bertolet B, Ornato JP, Gutterman JM. Aminophylline in
the treatment of atropine-resistant bradyasystole. Resuscitation 2000;
47: 105–12.
16 Viskin, S, Belhassen B, Roth A, et al., Aminophylline for
bradyasystolic cardiac arrest refractory to atropine and epinephrine.
Ann Intern Med 1993; 118: 279–81.
17 Littmann L, Ashline PT, Hayes WJ, et al. Aminophylline fails to
improve the outcome of cardiopulmonary resuscitation from
prolonged ventricular fibrillation: a placebo-controlled,
randomized, blinded experimental study. J Am Coll Cardiol 1994;
23: 1708–14.
18 Burton JH, Mass M, Menegazzi JJ, Yealy DM. Aminophylline as an
adjunct to standard advanced cardiac life support in prolonged
cardiac arrest. Ann Emerg Med 1997; 30: 154–58.
19 Mader TJ, Gibson P. Adenosine receptor antagonism in refractory
asystolic cardiac arrest: results of a human pilot study. Resuscitation
1997; 35: 3–7.
20 Perouansky M, Shamir M, Hershkowitz E, Donchin Y. Successful
resuscitation using aminophylline in refractory cardiac arrest with
asystole. Resuscitation 1998; 38: 39–41.
21 Mader TJ, Smithline HA, Gibson P. Aminophylline in
undifferentiated out-of-hospital asystolic cardiac arrest. Resuscitation
1999; 41: 39–45.
22 Lee CC, Dill CE, Carter WA. Restoration of spontaneous circulation
from asystole with aminophylline. Am J Emerg Med 2000;
18: 350–51.
23 Lee CC, Kim GW, Kim SH, Crupi RS. Cases of aminophylline and
vasopressin use after failed prehospital resuscitation of cardiac
arrest. Prehosp Emerg Care 2001; 5: 304–07.
24 Mader TJ, Smithline HA, Durkin L, Scriver G. A randomized
controlled trial of intravenous aminophylline for atropine-resistant
out-of-hospital cardiac arrest. Acad Emerg Med 2003; 10: 192–97.
25 American Heart Association, in collaboration with the International
Liaison Committee on Resuscitation. Guidelines 2000 for
cardiopulmonary resuscitation and emergency cardiac care:
international consensus on science, part 1: introduction. Circulation
2000; 102 (suppl 1): 1–384.
26 Ornato JP, Peberdy MA. The mystery of bradyasystole during
cardiac arrest. Ann Emerg Med 1996; 27: 576–87.
27 Cummins RO. The Utstein style for uniform reporting of
data from out-of-hospital cardiac arrest. Ann Emerg Med 1993;
22: 37–40.
28 Abu-Laban RB, Shuster M, MacPhail IA, et al. A comparison of
methodologic approaches to quantify return of spontaneous
circulation (ROSC) in cardiac arrest research including ROSC
survival analysis. Acad Emerg Med 2004; 11: 601–02.
29 Teasdale G, Murray G, Parker L, Jennett B. Adding up the Glasgow
Coma Score. Acta Neurochir Suppl 1979; 28: 13–16.
30 Brain Resuscitation Clinical Trial I Study Group: A randomized
clinical study of cardiopulmonary cerebral resuscitation: design,
methods, and patient characteristics. Am J Emerg Med 1986; 4:
72–86.
31 Jennett B, Bond M. Assessment of outcome after severe brain
damage. Lancet 1975; 1: 480–84.
32 Teng EL, Chui HC. The Modified Mini-Mental State (3MS)
examination. J Clin Phychiatry 1987; 48: 314–18.
33 Jette AM, Davis AR, Cleary PD, et al. The Functional Status
Questionnaire: reliability and validity when used in primary care.
J Gen Intern Med 1986; 1: 143–49. [Erratum, J Gen Intern Med 1986;
1: 427.]
34 Abu-Laban RB, Christenson JM, Innes GD, et al. Tissue
plasminogen activator in cardiac arrest with pulseless electrical
activity. N Engl J Med 2002; 346: 1522–28. [Erratum, N Engl J Med
2003; 349: 1487.]
8. Articles
1584 www.thelancet.com Vol 367 May 13, 2006
35 Gray JD. The problem of consent in emergency medicine research.
Can J Emerg Med 2001; 3: 213–18.
36 Lewis RJ. An introduction to the use of interim data analyses in
clinical trials. Ann Emerg Med 1993; 22: 463–69.
37 Wenzel V, Krismer AC, Arntz HR, Sitter H, Stadlbauer KH,
Lindner KH. European Resuscitation Council Vasopressor During
Cardiopulmonary Resuscitation Study Group. A comparison of
vasopressin and epinephrine for out-of-hospital cardiopulmonary
resuscitation. N Engl J Med 2004; 350: 105–13.
38 Kaplan JL, Gao E, de Garavilla L, Victain M, Minczak B, Dalsey W.
Adenosine A1 antagonism attenuates atropine-resistant hypoxic
bradycardia in rats. Acad Emerg Med 2003; 10: 923–30.
39 Aufderheide TP, Sigurdsson G, Pirrallo RG, et al. Hyperventilation-
induced hypotension during cardiopulmonary resuscitation.
Circulation 2004; 109: 1960–65.
40 Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of
cardiopulmonary resuscitation during out-of-hospital cardiac arrest.
JAMA 2005; 293: 299–304.