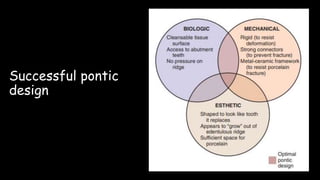
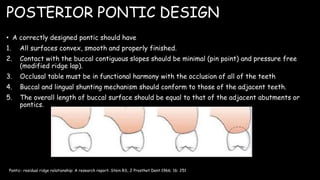
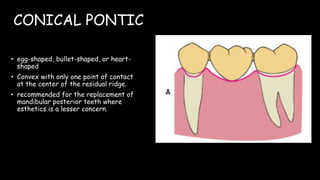
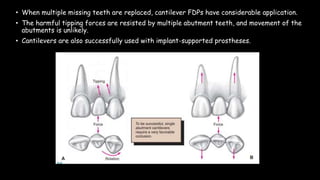
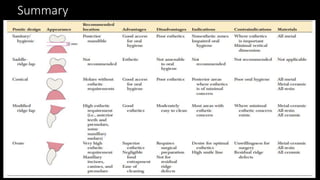
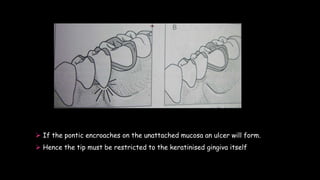
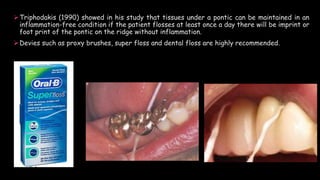
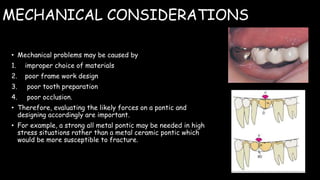
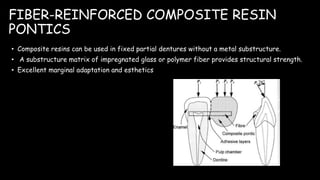
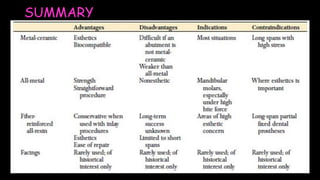
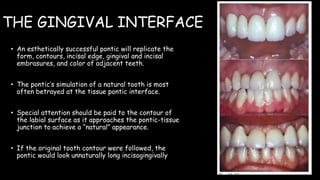
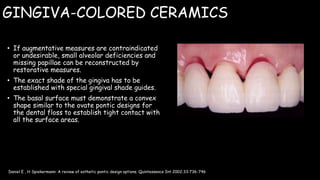
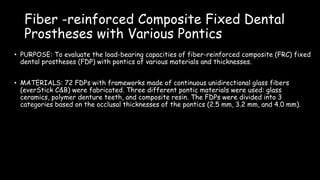
The document discusses pontic design for fixed dental prostheses. It covers pretreatment assessment of residual ridge contours, classifications of ridge deformities, surgical modification techniques, and ideal requirements for pontics. Pontic designs are classified based on their shape and materials. Factors in pontic selection include esthetics and oral hygiene. Common designs for anterior and posterior regions are described, including sanitary, ovate, and saddle pontics. Biological considerations for pontic design involve maintaining the residual ridge, abutment teeth, and supporting tissues.

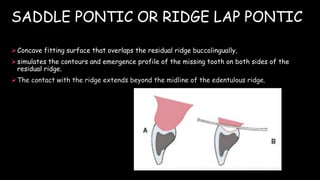
![PRETREATMENT ASSESSMENT
I] PONTIC SPACE:
One function of FPD is to prevent tilting or drifting of the adjacent teeth into the
edentulous space.
Drifting / tilting
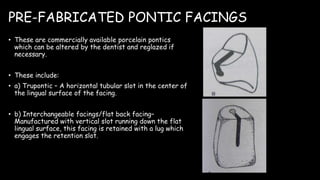
Reduced pontic space
Difficulty in fabricating pontic](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-7-320.jpg)
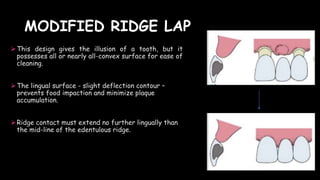
![ The edentulous ridge contour and topography should be carefully evaluated during the
treatment planning phase.
Features of Ideal Ridge Contour:
Smooth and regular surface of attached gingiva
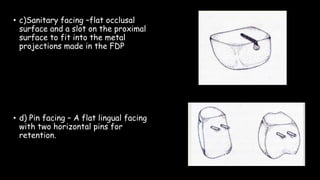
Facilitate maintenance of plaque-free environment
Sufficient height and width
Mimic adjacent tooth contours
Appear to emerge from the ridge
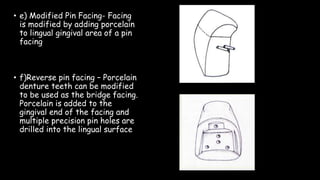
Facially, free of frenal attachment
II] RESIDUAL RIDGE CONTOUR](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-9-320.jpg)

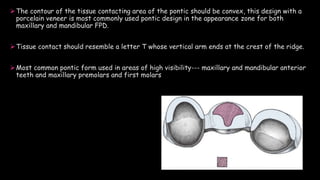
![SURGICAL CORRECTION
I] THE ROLL TECHNIQUE FOR
SOFT TISSUE RIDGE
AUGMENTATION:](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-14-320.jpg)
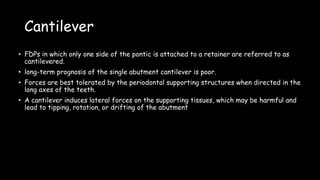
![II] THE POUCH TECHNIQUE
FOR SOFT TISSUE RIDGE
AUGMENTATION:](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-15-320.jpg)
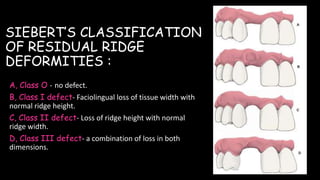
![CLASS II & CLASS III DEFECTS
I] INTERPOSITIONAL
GRAFT:
Variation of pouch technique
Augmentation of ridge height &
width](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-16-320.jpg)
![II] ONLAY
GRAFT](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-17-320.jpg)


![PONTIC DESIGN CLASSIFICATION
• According to Rosenstiel
A] MUCOSAL CONTACT:
1. Ridge lap
2. Modified ridge lap
3. Ovate
4. Conical
B) NO MUCOSAL CONTACT
1. Sanitary (hygienic)
2. Modified sanitary (hygienic)](https://image.slidesharecdn.com/ponticandponticdesigns-201011153902/85/Pontic-and-pontic-designs-23-320.jpg)












































![5)pontic and pontic designs [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5ponticandponticdesignsautosaved-250715095630-2c1631ed-thumbnail.jpg?width=640&height=640&fit=bounds)





![/'.,mklppontics final year.pptx m,l;;[']\](https://cdn.slidesharecdn.com/ss_thumbnails/ponticsfinalyear-251031103915-60ae6a8b-thumbnail.jpg?width=640&height=640&fit=bounds)



































