Overcoming the Challenges of Acute and Chronic GVHD: The Integration of Novel Therapies Into Modern Management Protocols
•
0 likes•83 views

Chair, Leslie Kean, MD, PhD, Corey Cutler, MD, MPH, FRCP(C), and Shernan Holtan, MD, prepared useful Practice Aids pertaining to graft-versus-host disease for this CME activity titled “Overcoming the Challenges of Acute and Chronic GVHD: The Integration of Novel Therapies Into Modern Management Protocols.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/3qkmiiY. CME credit will be available until June 18, 2023.

Recommended
Recommended
More Related Content
Similar to Overcoming the Challenges of Acute and Chronic GVHD: The Integration of Novel Therapies Into Modern Management Protocols
Similar to Overcoming the Challenges of Acute and Chronic GVHD: The Integration of Novel Therapies Into Modern Management Protocols (16)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Overcoming the Challenges of Acute and Chronic GVHD: The Integration of Novel Therapies Into Modern Management Protocols
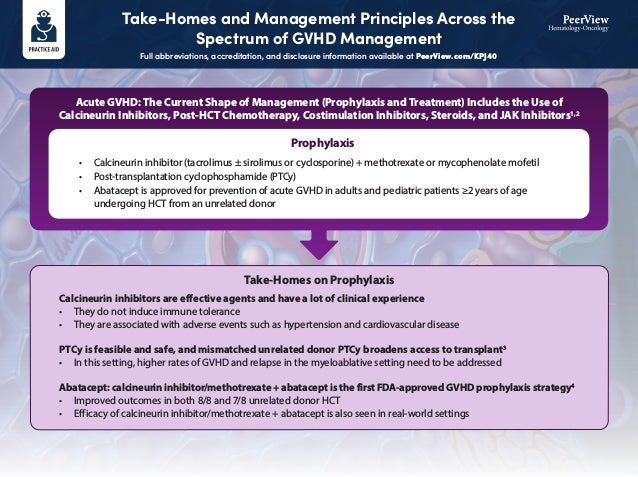
- 1. Acute GVHD: The Current Shape of Management (Prophylaxis and Treatment) Includes the Use of Calcineurin Inhibitors, Post-HCT Chemotherapy, Costimulation Inhibitors, Steroids, and JAK Inhibitors1,2 • Calcineurin inhibitor (tacrolimus ± sirolimus or cyclosporine) + methotrexate or mycophenolate mofetil • Post-transplantation cyclophosphamide (PTCy) • Abatacept is approved for prevention of acute GVHD in adults and pediatric patients ≥2 years of age undergoing HCT from an unrelated donor Calcineurin inhibitors are effective agents and have a lot of clinical experience • They do not induce immune tolerance • They are associated with adverse events such as hypertension and cardiovascular disease PTCy is feasible and safe, and mismatched unrelated donor PTCy broadens access to transplant3 • In this setting, higher rates of GVHD and relapse in the myeloablative setting need to be addressed Abatacept: calcineurin inhibitor/methotrexate + abatacept is the first FDA-approved GVHD prophylaxis strategy4 • Improved outcomes in both 8/8 and 7/8 unrelated donor HCT • Efficacy of calcineurin inhibitor/methotrexate + abatacept is also seen in real-world settings Prophylaxis Take-Homes on Prophylaxis Take-Homes and Management Principles Across the Spectrum of GVHD Management Full abbreviations, accreditation, and disclosure information available at PeerView.com/KPJ40
- 2. Acute GVHD: The Current Shape of Management (Prophylaxis and Treatment) Includes the Use of Calcineurin Inhibitors, Post-HCT Chemotherapy, Costimulation Inhibitors, Steroids, and JAK Inhibitors1,2 First-line therapy • Methylprednisolone (initiate for grade ≥2) Steroid-refractory • Ruxolitinib (adult and pediatric patients aged ≥12 years) Basic treatment principles: Provide appropriate immunosuppression + supportive care; appropriate immunosuppression is determined by severity of disease5,6 • Higher-risk disease may be signaled by high levels of amphiregulin Initial steroid-based therapy is effective but be prepared to plan for subsequent/second-line therapy7 • ~50% of patients may need second-line therapy Ruxolitinib is an approved second-line option in steroid-refractory acute GVHD • Longer follow-up from the REACH2 study continues to show the benefits of ruxolitinib vs best available therapy (FFS and EFS) in this setting8 Treatment Take-Homes on Treatment Take-Homes and Management Principles Across the Spectrum of GVHD Management Full abbreviations, accreditation, and disclosure information available at PeerView.com/KPJ40
- 3. In Chronic GVHD, Treatment Also Includes Multiple Modalities Such as Steroids and Calcineurin, BTK, JAK, and ROCK inhibitors1,2 Treatment Take-Homes on Treatment First-line therapy • Steroids and calcineurin inhibitors • Mycophenolate mofetil in triple-agent regimens Steroid-refractory • Ibrutinib • Ruxolitinib (adult and pediatric patients aged ≥12 years) First-line therapy in chronic GVHD remains steroid and calcineurin-inhibitor based • Emerging options (not yet approved) may include combinations of steroids with JAK or BTK inhibitors Newer developments in second- and third-line therapy include the FDA approval of JAK inhibitors (eg, ruxolitinib), BTK inhibitors (eg, ibrutinib), and ROCK inhibitors (eg, belumosudil) • Based on current evidence, factors that may influence treatment selection in these settings include: age of <18, a prior B-cell malignancy, presence of myelofibrosis/JAK2 disease, or lung involvement, including advanced fibrosis8-11 Third-line therapy • Belumosudil 1. Ruutu T et al. Bone Marrow Transplant. 2014;49:168-173. 2. Wolff D et al. Biol Blood Marrow Transplant. 2010;16:1611-1628. 3. Bolaños-Meade J et al. Lancet Haematol. 2019;6:e132-e143. 4. Watkins B et al. J Clin Oncol. 2021;39:1865-1877. 5. Holtan S et al. Blood Adv. 2018;2:1882-1888. 6. Levine JE et al. Lancet Haematol. 2015;2:e21-e29. 7. Jagasia M et al. Blood. 2020;135:1739-1749. 8. Zeiser R et al. N Engl J Med. 2020;382:1800-1810. 9. Chin K-K, Cutler C et al. Transplant Cell Ther. 2021;27:990.e1-990.e7. 10. Miklos D et al. EHA 2021. Oral Abstract Presentation. 11. Jagasia M et al. J Clin Oncol. 2021;39:1888-1898. Take-Homes and Management Principles Across the Spectrum of GVHD Management Full abbreviations, accreditation, and disclosure information available at PeerView.com/KPJ40