Can the Addition of Immunotherapy to Multimodal Management of Stage I-III NSCLC Help Break the Stalled Cycle of Poor Outcomes?
•
0 likes•66 views

Co-Chairs, Nasser Altorki, MD, and Jonathan D. Spicer, MD, PhD, FRCSC, prepared useful Practice Aids pertaining to NSCLC for this CME/MOC activity titled “Can the Addition of Immunotherapy to Multimodal Management of Stage I-III NSCLC Help Break the Stalled Cycle of Poor Outcomes?” For the full presentation, downloadable Practice Aids, and complete CME/MOC information, and to apply for credit, please visit us at https://bit.ly/3m1OV2m. CME/MOC credit will be available until February 27, 2023.

Recommended
Recommended
More Related Content
Similar to Can the Addition of Immunotherapy to Multimodal Management of Stage I-III NSCLC Help Break the Stalled Cycle of Poor Outcomes?
Similar to Can the Addition of Immunotherapy to Multimodal Management of Stage I-III NSCLC Help Break the Stalled Cycle of Poor Outcomes? (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Can the Addition of Immunotherapy to Multimodal Management of Stage I-III NSCLC Help Break the Stalled Cycle of Poor Outcomes?
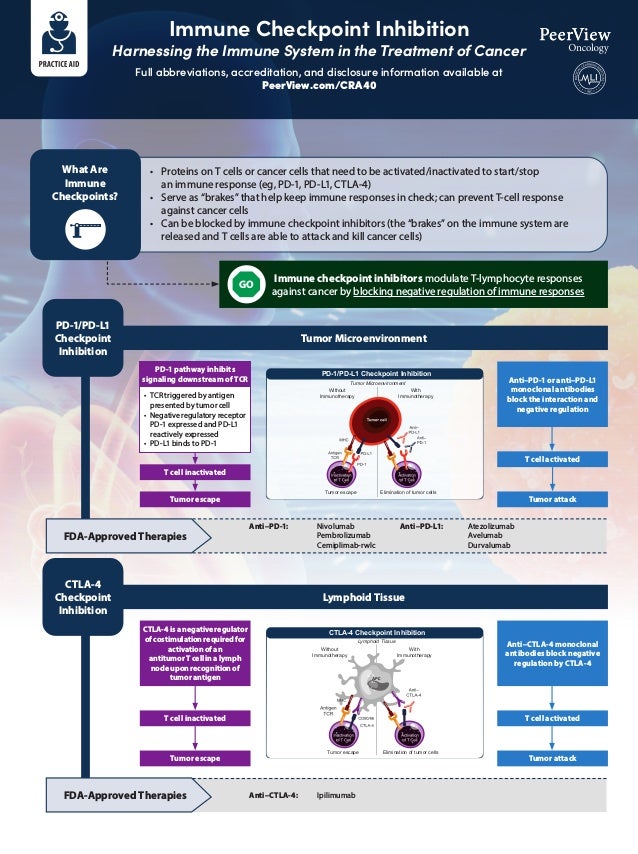
- 1. Immune Checkpoint Inhibition Harnessing the Immune System in the Treatment of Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Tumor Microenvironment Lymphoid Tissue Immune checkpoint inhibitors modulate T-lymphocyte responses against cancer by blocking negative regulation of immune responses PD-1 pathway inhibits signaling downstream of TCR • TCR triggered by antigen presented by tumor cell • Negative regulatory receptor PD-1 expressed and PD-L1 reactively expressed • PD-L1 binds to PD-1 T cell inactivated T cell inactivated T cell activated T cell activated Anti–PD-1 or anti–PD-L1 monoclonal antibodies block the interaction and negative regulation Anti–CTLA-4 monoclonal antibodies block negative regulation by CTLA-4 CTLA-4 is a negative regulator of costimulation required for activation of an antitumor T cell in a lymph node upon recognition of tumor antigen PD-1/PD-L1 Checkpoint Inhibition CTLA-4 Checkpoint Inhibition FDA-Approved Therapies FDA-Approved Therapies GO Tumor escape Tumor escape Tumor attack Tumor attack Anti–PD-1: Nivolumab Pembrolizumab Cemiplimab-rwlc Anti–CTLA-4: Ipilimumab Anti–PD-L1: Atezolizumab Avelumab Durvalumab • Proteins on T cells or cancer cells that need to be activated/inactivated to start/stop an immune response (eg, PD-1, PD-L1, CTLA-4) • Serve as “brakes” that help keep immune responses in check; can prevent T-cell response against cancer cells • Can be blocked by immune checkpoint inhibitors (the “brakes” on the immune system are released and T cells are able to attack and kill cancer cells) What Are Immune Checkpoints? Tumor Microenvironment Elimination of tumor cells Tumor escape With Immunotherapy Without Immunotherapy PD-1/PD-L1 Checkpoint Inhibition Elimination of tumor cells Tumor escape CTLA-4 Checkpoint Inhibition With Immunotherapy Without Immunotherapy Lymphoid Tissue
- 2. Expanding Role and Use of Neoadjuvant and Adjuvant Immunotherapy in Resectable Solid Tumors Rationale and Current Approvals/Indications Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Neoadjuvant immunotherapy is administered before surgery and can reduce the size of the primary tumor as well as eliminate residual cancers cells left after surgery Rationale: • Lower disease burden and intact immune system • T-cell response generated against in situ primary tumor with diverse antigen load • Fast endpoints to assess response • Allows for translational research: biologic and immunologic correlative studies Rationale: • Lower disease burden and intact immune system • Immunological pathways are disrupted by surgical stress • No risk for delaying surgery with adjuvant versus neoadjuvant approach • Prior chemotherapy or other systemic/local therapies may help augment immune responses Adjuvant immunotherapy is administered after surgery and leads to an increase in activated T cells that can eliminate residual cancer cells in the tumor bed Comparison of adjuvant and neoadjuvant immunotherapy treatment approaches1 Immunotherapy T cells T-cell activation Resection surgery Solid tumor Resection surgery Immunotherapy T-cell activation and additional immunotherapy Tumor cells Artery Healthy cells Immunotherapy
- 3. Expanding Role and Use of Neoadjuvant and Adjuvant Immunotherapy in Resectable Solid Tumors Rationale and Current Approvals/Indications Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Overall survival (OS) is the gold-standard outcome measure for phase 3 trials, but the protracted length of these clinical trials in resectable cancers makes this research daunting and expensive One strategy to expedite clinical trials, including those assessing immunotherapies in early-stage cancer settings, is the use of newer, innovative surrogate measurements for endpoints Because pathologic response reflects a therapy’s ability to eradicate tumor cells more directly than radiographic evaluation using RECIST criteria, it may better correlate with clinically meaningful outcomes Several trials in different tumor types have correlated the novel endpoints with more traditional endpoints such as OS, DFS, and RFS, but additional confirmatory studies are needed Many adjuvant approvals have been based on disease-free survival (DFS) Trials in neoadjuvant settings provide an opportunity to assess pathologic response as an early surrogate marker for survival outcomes, and pathologic response criteria such as major pathological response (MPR) and pathologic complete response (pCR) have been assessed in neoadjuvant immunotherapy trials; there are various definitions, but generally: MPR: ≤10% of viable tumor in the treated tumor bed pCR: complete absence of viable tumor in the treated tumor bed Recently, immune-related pathologic response criteria (irPRC) have also been developed with the aim of assessing the full spectrum of response to immunotherapy in resection specimens Different scoring systems exist or are in development for evaluating pathologic response in various tumor types (eg, melanoma, lung cancer, bladder cancer) Relevant endpoints for neoadjuvant and adjuvant immunotherapy clinical trials2-8
- 4. Expanding Role and Use of Neoadjuvant and Adjuvant Immunotherapy in Resectable Solid Tumors Rationale and Current Approvals/Indications Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Adjuvant treatment of patients with urothelial carcinoma who are at high risk of recurrence after undergoing radical resection Adjuvant treatment of patients with completely resected esophageal or gastroesophageal junction cancer with residual pathologic disease who have received neoadjuvant chemoradiotherapy Adjuvant treatment of patients with melanoma with lymph node involvement or metastatic disease who have undergone complete resection Current perioperative approvals and indications of immunotherapies in solid tumors9 Nivolumab Adjuvant treatment of patients with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy Ipilimumab
- 5. Expanding Role and Use of Neoadjuvant and Adjuvant Immunotherapy in Resectable Solid Tumors Rationale and Current Approvals/Indications Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Neoadjuvant treatment of high-risk, early-stage triple-negative breast cancer with chemotherapy adjuvant treatment after surgery as a single agent Adjuvant treatment of patients with renal cell carcinoma at intermediate-to-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions Adjuvant treatment of patients with stage IIB, IIC, or III melanoma following complete resection Patients with BCG-unresponsive, high-risk, non–muscle invasive bladder cancer with carcinoma in situ with or without papillary tumors who are ineligible for or have elected not to undergo cystectomy Current perioperative approvals and indications of immunotherapies in solid tumors9 Pembrolizumab Adjuvant treatment following resection and platinum-based chemotherapy in patients with stage II to IIIA non–small cell lung cancer whose tumors have PD-L1 expression on ≥1% of tumor cells Atezolizumab 1. Krishnamoorthy M et al. J Natl Cancer Inst. 2021;113:823-832. 2. Topalian SL et al. Science 2020;367:eaax0182. 3. Benitez JC et al. Clin Cancer Res. 2020;26:5068-5077. 4. Bilusic M, Gulley JL. J Natl Cancer Inst. 2021;113:799-800. 5. Krishnamoorthy M et al. J Natl Cancer Inst. 2021;113:823- 832. 6. O’Donnell JS et al. Clin Cancer Res. 2019;25:5743-5751. 7. Hellmann MD et al. Lancet Oncol. 2014;15:e42-50. 8. Cottrell TR et al. Ann Oncol. 2018;29:1853-1860. 9. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies- approval-notifications.
- 6. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 What Are irAEs? • Immune checkpoint inhibitors are associated with important clinical benefits, but general immunologic enhancement can also lead to a unique spectrum of immune-related adverse events • Any organ system can be affected, but more commonly occurring are pulmonary (pneumonitis), dermatologic (rash, pruritus, blisters, ulcers, vitiligo), gastrointestinal (diarrhea, enterocolitis, transaminitis, hepatitis, pancreatitis), and endocrine (thyroiditis, hypophysitis, adrenal insufficiency) irAEs Endocrine Hyper- or hypothyroidism Hypophysitis Adrenal insufficiency Diabetes Hepatic Hepatitis Renal Nephritis Dermatologic Rash Pruritus Psoriasis Vitiligo DRESS Stevens-Johnson Hematologic Hemolytic anemia Thrombocytopenia Neutropenia Hemophilia Ocular Uveitis Conjunctivitis Scleritis, episcleritis Blepharitis Retinitis Respiratory Pneumonitis Pleuritis Sarcoid-like granulomatosis Cardiovascular Myocarditis Pericarditis Vasculitis Gastrointestinal Colitis Ileitis Pancreatitis Gastritis Neurologic Neuropathy Guillain Barŕe Myelopathy Encephalitis Myasthenia Musculoskeletal Arthritis Dermatomyositis Prevention Anticipation Treatment Monitoring Detection
- 7. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 Guidance for Surgeons: Suspect, Detect, and Refer for Treatment5,6 • irAEs frequently occur in the perioperative setting, either before or after surgical intervention • irAEs occurring during neoadjuvant immunotherapy are generally manageable and in most cases should not exclude patients from surgery • The onus is on the surgeon to have a high degree of suspicion for potential toxicities in patients treated with immunotherapy • Vague symptoms should not be dismissed, because nonspecific ailments can be indicative of severe toxicity – Rheumatologic toxicities and endocrinopathies are some of the most difficult to recognize, given their relatively nonspecific presentation » For example, fatigue, poor energy, and low mood could represent hypophysitis or adrenal insufficiency – Other toxicities can be essentially asymptomatic » For example, renal and hepatic toxicity are generally only detected on routine labs – Pneumonitis is another relevant irAE requiring awareness by surgeons, as severe pneumonitis could potentially exclude patients from operative therapy, but significant pneumonitis has been rare in trials to date • A comprehensive workup for irAEs, with a thorough history specifically targeted to potential irAEs, should be conducted • Coordinate and collaborate with oncologists and other multidisciplinary experts to optimally diagnose and manage irAEs in patients who have received/are receiving perioperative immunotherapy • The National Comprehensive Cancer Network (NCCN) and American Society of Clinical Oncology (ASCO) have issued guidelines for recognition and management of immune-related adverse events
- 8. How Should irAEs Be Diagnosed and Managed? Minimal or No Symptoms; Diagnostic Changes Only • In general, immunotherapy should be continued with close monitoring, with the exception of some neurologic, hematologic, and cardiac toxicities Mild to Moderate Symptoms • Hold checkpoint inhibitor therapy for most grade 2 toxicities • Consider resuming immunotherapy when symptoms and/or lab values revert to grade 1 • Corticosteroids (initial dose of 0.5-1.0 mg/kg/day of prednisone or equivalent) may be administered Severe or Life-Threatening Symptoms Grade 3 toxicities • Hold checkpoint inhibitor therapy • Initiate high-dose corticosteroids (prednisone 1-2 mg/kg/day or methylprednisolone IV 1-2 mg/kg/day) • If symptoms do not improve with 48-72 hours of high-dose corticosteroid, infliximab may be offered for some toxicities • Taper corticosteroids over the course of at least 4-6 weeks • When symptoms and/or laboratory values revert to grade 1, rechallenging with immunotherapy may be considered; however, caution is advised, especially in those patients with early-onset irAEs; dose adjustments are not recommended Grade 4 toxicities • In general, permanent discontinuation of checkpoint inhibitor therapy is warranted, with the exception of endocrinopathies that have been controlled by hormone replacement irAEs are often diagnosed by exclusion; other causes should be ruled out (including AEs of other therapies used), but immunotherapy-related toxicity should always be included in the differential There should be a high level of suspicion that new symptoms are treatment related; early recognition, evaluation, and treatment of irAEs plus patient education are essential for the best outcome Depending on severity of irAE, management may require corticosteroid or other immunosuppressive treatment and interruption or discontinuation of therapy If appropriate immunosuppressive treatment is used, patients generally recover from irAEs Use of immunosuppressive therapy to manage irAEs does not appear to impact response to immunotherapy Grade 1 Grade 2 Grade 3/4 Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40
- 9. Hold immunotherapy with radiographic evidence of pneumonitis progression May offer one repeat CT in 3-4 weeks; in patients who have had baseline testing, may offer a repeat spirometry/DLCO in 3-4 weeks May resume immunotherapy with radiographic evidence of improvement or resolution; if no improvement, should treat as grade 2 Monitor patients weekly with history, physical examination, and pulse oximetry; may also offer CXR Grade 2: Symptomatic; 1 lobe of lung or 25%-50% of lung parenchyma; medical intervention indicated; limiting instrumental ADL Grade 3: Severe symptoms requiring hospitalization; involves all lung lobes or 50% of lung parenchyma; limiting self care Grade 4: Life-threatening respiratory compromise; urgent intervention indicated (intubation) Hold immunotherapy until resolution to grade ≤1 Prednisone 1-2 mg/kg/day and taper by 5-10 mg/week over 4-6 weeks Consider bronchoscopy with BAL Consider empiric antibiotics Monitor patients every 3 days with history, physical examination, and pulse oximetry; consider CXR; if no clinical improvement after 48-72 hours of prednisone, treat as grade 3 Discontinue immunotherapy Empiric antibiotics; methylprednisolone IV 1-2 mg/kg/day; if no improvement after 48 hours, may add infliximab 5 mg/kg, or mycophenolate mofetil IV 1 g 2x/day, or IVIG x 5 days, or cyclophosphamide Taper corticosteroids over 4-6 weeks Pulmonary and infectious disease consults if necessary Bronchoscopy with BAL +/- transbronchial biopsy Patients should be hospitalized for further management How Should Pulmonary irAEs Be Diagnosed and Managed? Pneumonitis: focal or diffuse inflammation of the lung parenchyma (typically identified on CT imaging) Diagnostic work-up: CXR, CT, pulse oximetry; for grade ≥2, may include infectious work-up Grade 1: Asymptomatic; confined to 1 lobe of lung or 25% of lung parenchyma; clinical or diagnostic observations only Additional considerations • GI and pneumocystis prophylaxis may be offered to patients on prolonged steroid use (12 weeks) • Consider calcium and vitamin D supplementation with prolonged steroid use • Bronchoscopy + biopsy; if clinical picture is consistent with pneumonitis, no need for biopsy Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CRA40 1. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1786. 2. Postow MA et al. N Engl J Med. 2018;378:158-168. 3. Gordon R et al. Clin J Oncol Nurs. 2017;21(suppl 2):45-52. 4. Champiat S et al. Ann Oncol. 2016;27:559-574. 5. Helmink BA et al. Ann Surg Oncol. 2020;27:1533-1545. 6. Stiles BM et al. J Thorac Cardiovasc Surg. 2020;160:1376-1382.