
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Clavicular fracture .pptx
Similar to Clavicular fracture .pptx (20)
Recently uploaded
Recently uploaded (20)
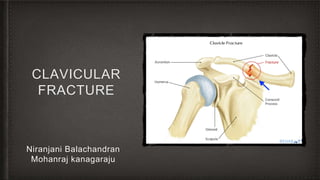
Clavicular fracture .pptx
- 2. Clavicle fracture • It is also known as broken collarbone, often as a result of indirect or direct trauma to shoulder region. • Very common injuries in adults (2-5%) and children (10-15%) and represent the 44-66% of all shoulder fractures. • It is the most common fracture of childhood.( perinatal fracture with birth trauma) • A fall onto the lateral shoulder most frequently causes a clavicle fracture. • While most clavicle fractures treated conservatively, severely displaced or comminuted fractures may require surgical fixation.
- 3. How common they are? • Clavicle fractures represent 2% to 10% of all fractures. • Affect 1 in 1000 people per year • Approximately two-third of all clavicle fractures occurring in males between ages of 13 and 20 years , 20% in women • The middle third of the clavicle is fractured in 69% of cases following the distal third in 28% of cases and the proximal third in 3% of cases
- 4. Clinical anatomy • It is located subcutaneously between the sternum and the scapula, connects the arm to the body. • It is the first bone in human body to begin intra-membranous ossification directly from mesenchyme during the fifth week of fetal life. • Similar to all long bones, it has both a medial and lateral Clavicular epiphysis but it lacks a well defined medullary cavity. • It S shaped double curve, which is convex medially and concave laterally.
- 5. How do they occur? • Younger individuals often sustain these injuries by way of moderate to high-energy mechanisms such as motor vehicle accidents or sports injuries. • Elderly individuals are more likely to sustain injuries because of the sequela of a low energy fall • Although a fall onto an outstretched hand was traditionally considered the common mechanism, it has been found that the clavicle most often fails in direct compression from a force applied directly to the shoulder. • About 87% of reported cases, a clavicle fracture results from a fall directed onto the lateral shoulder.
- 6. How are they classified? They typically described using the Allman classification system, dividing the clavicle into 3 groups based on location which was later revised by Neer ( in which Group 2 was further classified into 3 types) Group 1: fractures of the middle third or mid shaft. They defined by shortening/comminution/angulation Group 2: fractures of distal or lateral third ( common site for non-union. Around and lateral to coracoclavicular ligaments) Group 3: fractures of the proximal or medial third.( sternoclavicular dislocation) Robinson’s classification was more specific for different fracture pattern in middle third. Craig’s classification was more specific for fractures of lateral
- 7. What do they look like- clinically? The patient may appear with the following signs and symptoms: A patient may cradle the injured extremity with the uninjured arm May report snapping or cracking sound when injury occurs Shoulder may appear shortened relative to opposite side and may droop Swelling, ecchymosis, and tenderness over the clavicle Abrasion over clavicle suggest fracture from direct mechanism Crepitus from fracture ends rubbing against each other with gentle manipulation. Difficulty breathing or diminished breath sound on affected side indicate pulmonary injury, such as pneumothorax
- 9. What investigations should be ordered? • Diagnosis can often made by history and physical examination • Laboratory studies ordered according to the severity of the trauma. • With suspected vascular injury, obtain a CBC to check the hemoglobin and hematocrit values • If a pulmonary injury suspected perform an arterial blood gas test and obtain an expiration posteroanterior chest film. • Other imaging studies are • Radiography of clavicle and shoulder • CT • Arteriography • Ultrasonography
- 10. What do they look like on X- ray?
- 12. When is reduction required? • Clavicle fracture managed either surgically or conservatively based upon various factors include • Location • Nature of the fracture • Open Vs closed injury • Age • Neurovascular compromises • Traditionally, conservative management can done with sling immobilization and subsequent rehabilitation • It provide satisfactory results for undisplaced fractures
- 13. Surgical treatment • Chief goal is to achieve a healed Clavicular strut in normal anatomical position as possible • Indications for operation Severe displacement caused by comminution Symptomatic non-union Neurovascular injury Open fracture Type 2 distal fracture Multiple trauma Floating shoulder Inability to tolerate closed immobilization Cosmetic reason
- 15. Surgical procedure • It includes • Internal fixation with plates and screws • Intramedullary fixation • The routine removal of metal work was recommended for IM nails but not for plate fixation in mid-shaft displaced fracture. • In displaced lateral clavicle fracture routine removal of metalwork was performed for • Hook plate fixation • Screw fixation • Cerclage wire fixation • Tension band wire fixation • Not performed for, • Non ACJ spanning plate fixation • Suture fixation • These fixation methods are necessary for lateral clavicle fracture as it involves acromioclavicular joint and various ligaments that may become injured during fracture.
- 17. What are the potential complications associated? • Subclavian vessel injury • Hemopneumothorax • Brachial plexus paresis • Thoracic outlet syndrome • Nonunion • Malunion • Post traumatic arthritis • Refracture
- 18. THANK YOU