
Recommended
Recommended
More Related Content
Similar to Control of Ventilation in Health & Disease
Similar to Control of Ventilation in Health & Disease (20)
Recently uploaded
Recently uploaded (20)
Control of Ventilation in Health & Disease
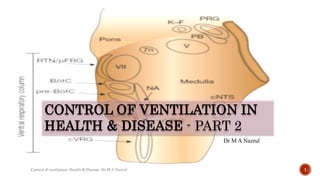
- 1. CONTROL OF VENTILATION IN HEALTH & DISEASE - PART 2 Dr M A Nazrul 1 Control of ventilation: Health & Disease- Dr M A Nazrul
- 2. CONTROLLER EFFECTOR LUNG VOLUME SENSOR rCPG Inspiration/Expiration Muscles of respiration Chemoreceptors Mechanoreceptors Reference- Fishman’s Pulmonary Diseases and Disorders Fifth Edition –Chapter 11 Control of Ventilation 2 Control of ventilation: Health & Disease- Dr M A Nazrul
- 3. CONCEPT OF LOOP GAIN • Loop gain is an engineering term that is used to define the stability or instability of a negative feedback control system. • It represents the overall response of the plant (representing the lung and respiratory muscles), the controller (representing the ventilatory control centers and the chemoreceptors), and the delay inherent in transferring the signal between the plant and the controller. • Controller gain, or chemoresponsiveness, is the change in ventilation, to hypercapnia and hypocapnia, that is ΔV₁/ΔPaCO₂ where ΔV₁ is minute ventilation. • Plant gain is determined by the magnitude of the reduction in Paco2 resulting from a given change in ventilation , that is ΔPaCO₂/ ΔV₁, the efficiency with which carbon dioxide is eliminated. 3 Control of ventilation: Health & Disease- Dr M A Nazrul
- 4. 4 Control of ventilation: Health & Disease- Dr M A Nazrul
- 5. 5 Control of ventilation: Health & Disease- Dr M A Nazrul • In the case of ventilation, the propensity for CO2 fluctuations is a function of an individual’s loop gain. That is, an individual with a high loop gain is prone to developing periodic breathing or Cheyne–Stokes breathing, even with minimal perturbation. On the other hand, an individual with low loop gain will maintain relatively stable breathing patterns even with major perturbations. • Increased controller gain (eg, due to sustained hypoxia, acute intermittent hypoxia, or heart failure) or increased plant gain due to metabolic alkalosis or disorders of hypoventilation, or both, in an individual narrows the carbon dioxide reserve to increase breathing instability. • If loop gain is less than 1, then the system corrects itself (i.e., breathing normalizes), but if loop gain is 1 or greater, then the system remains unstable. • The importance of loop gain is receiving increasing attention given the recognition of its importance in obstructive sleep apnea, central sleep apnea, periodic breathing at high altitude and other conditions.
- 6. Control of ventilation: Health & Disease- Dr M A Nazrul 6
- 7. Control of ventilation: Health & Disease- Dr M A Nazrul 7
- 8. Control of ventilation: Health & Disease- Dr M A Nazrul 8 Cheyne–Stokes Breathing was first observed in patients with cardiac or CNS disease, but it has since been reported in seemingly normal humans. The appearance of Cheyne–Stokes breathing can occur during wakefulness although often masked by behavioral influences, but is more common during nonrapid eye movement (NREM) sleep. Arousal tends to occur during the hyperpneic phase of the respiratory pattern, a finding which is often associated with paroxysmal nocturnal dyspnea in patients with heart failure.
- 9. 9 Control of ventilation: Health & Disease- Dr M A Nazrul SLEEP • Sleep is classified on the basis of the electroencephalogram(EEG) and electro-oculogram (EOG) into rapid eye movement(REM) and non-REM (stages N1–N4) sleep • Non-REM sleep is often thought of as the “restorative”nondreaming phase of sleep. It is promoted and sustained by a system of neurons that inhibit the brain-arousal systems of wakefulness. 1. Stage N1 is dozing, from which arousal easily takes place. The EEG is low voltage, and the frequency is mixed but predominantly fast. 2. In Stage N2,the background EEG is similar to stage N1 but with episodic sleep spindles (frequency 12– 14 Hz) and K complexes(large biphasic waves of characteristic appearance). Slow, large-amplitude (delta) waves start to appear in stage N2 3. In Stage N3 Delta waves become more dominant, in which spindles are less conspicuous and K complexes become difficult to distinguish. 4. In Stage N4, which is often referred to as deep sleep, the EEG is mainly high voltage (more than 75 mV) and more than 50% slow (delta) frequency • REM sleep- The EEG pattern is the same as in stage N1, but the EOG shows frequent rapid eye movements that are easily distinguished from the rolling eye movements of non-REM sleep. Skeletal muscle tone generally decreases, and dreaming occurs during REM sleep.
- 10. Control of ventilation: Health & Disease- Dr M A Nazrul 10
- 11. 11 Control of ventilation: Health & Disease- Dr M A Nazrul
- 12. 12 Control of ventilation: Health & Disease- Dr M A Nazrul BREATHING IS DEPENDENT ON FEEDBACK REGULATION IN SLEEP • There are mutually opposing interactions between the wakefulness-promoting neuronal systems and the non-REM sleep-promoting neuronal systems • This organization leads to wakefulness being associated with both a relatively high level of activity in the wake- promoting neuronal arousal systems combined with a relatively low level of activity in the opposing sleep promoting GABA system and vice versa.
- 13. 13 Control of ventilation: Health & Disease- Dr M A Nazrul • A prevailing level of tonic excitation into the respiratory network is essential to drive respiratory rhythm and muscle activation • The brain arousal systems of wakefulness provide a major source of such excitation to modulate breathing volitionally and/or non-volitionally termed behavioral influences or the wakefulness stimulus • Such behavioral influences on respiratory network activity are reduced or withdrawn as one moves from wakefulness to non-REM sleep. • As a result, the respiratory system becomes dependent upon feedback regulation in non- REM sleep to sustain sufficient activity. • Tonic activity of the peripheral and central chemoreceptors is normally sufficient to sustain effective breathing in non-REM sleep • However, any reduction or defect in feedback chemoreceptor control, for any reason, causes severe respiratory disturbance in non-REM sleep
- 14. Control of ventilation: Health & Disease- Dr M A Nazrul 14 Importance of feedback regulation: Example 1 Hypocapnia is a potential cause of central apnea. Interestingly, hypocapnia, by itself, is not sufficient to elicit central apneas in wakefulness or in REM sleep because of the concomitant presence of behavioral influences on breathing. However, in non-REM sleep, hypocapnia can elicit central apneas because the stimulatory effects of brain arousal (i.e., behavioral influences) to the respiratory network are absent. Hypocapnia may be present at the onset of sleep as a result of chronic hyperventilation in wakefulness caused, for example, by heightened chemoreceptor drive (e.g., resulting from congestive heart failure) or by exaggerated behavioral influences on breathing (e.g., caused by anxiety). Hypocapnia at sleep onset can also result from the transient hyperventilation caused by sleep disturbance and brief arousal from sleep: the hyperventilation predisposing to unstable breathing by depleting the CO2 reserve .
- 15. Control of ventilation: Health & Disease- Dr M A Nazrul 15 Importance of feedback regulation: Example 2 ONDINE’S CURSE In Greek mythology, the nymph Ondine was an immortal water spirit who became human after falling in love for a man, marrying him, and having a baby. In one of the versions of the tale, when she caught her husband sleeping with another woman, she cursed him to remain awake in order to control his own breathing. During the 19th century, the rare syndrome characterized by loss of autonomic breath control, while voluntary respiration remains intact, was cleverly named “Ondine's curse”. Nowadays, the term Ondine's curse is usually associated with Congenital central hypoventilation syndrome
- 16. CONGENITAL CENTRAL HYPOVENTILATION SYNDROME a rare neurological disorder characterized by inadequate breathing during NREM sleep ventilate normally during wakefulness and during REM sleep Patients congenitally lack or have poor chemosensitivity to both hypercapnia and hypoxia, and suffer from inadequate ventilation In more than 99% of CCHS patients, mutations have been found in the paired-like homeobox 2b (PHOX2B) gene, a gene expressed by neurons involved in peripheral and central chemoreception PHOX2B is not expressed by respiratory neurons can perhaps explain the ability of these patients to breathe in wakefulness, because the mutation does not affect respiratory neurons. the state of wakefulness itself provides sufficient excitatory drive to the respiratory system to mask the major defect in chemoreceptor activity caused by the PHOX2B mutation. The ability of the CCHS patients to breathe normally in REM sleep further reinforces the principle that the relatively high levels of brain activation inherent to REM sleep can provide sufficient restoration of behavioral drives to the respiratory network to reinstitute breathing. Control of ventilation: Health & Disease- Dr M A Nazrul 16
- 17. Control of ventilation: Health & Disease- Dr M A Nazrul 17 Importance of feedback regulation: Example 3 Wakefulness as an independent driver of respiratory activity • Deep non-REM sleep and anesthesia are the most vulnerable states for respiratory rate depression by opioids at the pre-Bötzinger complex. 1. Opioids depress the rate and depth of respiration at the pre-Böt C to induce ventilatory depression; this was reversed by injection of naloxone into the pre-Böt C. 2. Opioids also hyperpolarize the KF neurons, contributing to opioid-induced loss of the post inspiration phase of the respiratory cycle and induction of apneusis. 3. Opioids alter the discharge properties of cranial motoneurons of the larynx and pharynx and the bulbospinal neurons controlling the diaphragm, chest wall, and expiratory abdominal muscles -to induce chest and abdominal wall rigidity, -reduce genioglossus muscle activity and upper airway patency, -acutely blunt hypoxic and hypercapnic responsiveness • Breathing can be sustained by wakefulness even when opioids are present at the pre-Bötzinger complex. • However, loss of this important wakefulness stimulus to breathing can lead to hazardous respiratory depression in non-REM sleep and anesthesia. • The clinical relevance of this principle is that sedating agents can be deemed well tolerated in the initially alert patient but, when the stimulating effects of wakefulness are withdrawn during sleep, the patient may suffer significant respiratory depression • Particularly dangerous when patients with sleep-related breathing problems use opioids for pain management
- 18. Control of ventilation: Health & Disease- Dr M A Nazrul 18 SLEEP DISORDERED BREATHING • This term is used to describe a continuum of respiratory abnormalities seen during sleep, ranging from simple snoring to life-threatening obstructive sleep apnea. • All are characterized by periods of apnea, with or without episodes of airway narrowing or obstruction, that lead to repeated episodes of subcortical arousal from sleep and arterial hypoxia. • Four syndromes are described,but there is considerable overlap between them- 1. Upper airway resistance syndrome in which tidal volume and arterial oxygen saturation (SaO2) remain normal, but at the expense of extensive respiratory effort, which causes over 15 arousals per hour. 2. Obstructive sleep hypopnea involves frequent (.15 per hour) episodes of airway obstruction of sufficient severity to reduce tidal volume to less than 50% of normal for over 10 seconds. There may be small decreases in SaO2. 3. Obstructive sleep apnea is characterized by more than five episodes per hour of obstructive apneas lasting over10 seconds and associated with severe decreases in SaO2. In fact, durations of apnea may be as long as 90 seconds, and the frequency of the episodes as high as 160 per hour. In severe cases, 50% of sleep time may be spent without tidal exchange. 4. The last two syndromes are commonly grouped togetheras Sleep apnea/hypopnea syndrome (SAHS).
- 19. Control of ventilation: Health & Disease- Dr M A Nazrul 19 The Mechanism of Airway Obstruction There are four components contributing to airway obstruction during sleep-disordered breathing: 1. An anatomically narrow airway, 2. Inadequate control of airway muscles, 3. The ease of arousal during apnea (the arousal threshold) 4. Instability of the respiratory control system
- 20. Control of ventilation: Health & Disease- Dr M A Nazrul 20
- 21. Control of ventilation: Health & Disease- Dr M A Nazrul 21 CENTRAL APNEA • Central apneas arise from complete or partial reductions in central neural outflow to the respiratory muscles during sleep • Central apneas are distinguished from obstructive apneas by the absence of respiratory effort, which can be detected by routine monitoring techniques such as respiratory inductive plethysmography combined with assessment of nasal pressure • Mechanisms which can produce central apneas include (1) reduced excitation of chemoreceptors as a consequence of hypocapnia and hyperoxia (2) functional or actual structural medullary damage which may result in a pattern of grossly irregular ataxic breathing (3) loss of nonspecific respiratory excitatory stimulation (noise, light, tactile stimuli) in the absence of adequate chemical drive (4) active suppression of breathing by respiratory inhibitory reflexes, which is observed in a number of clinical situations including pharmacological therapy with methadone and other opiate medications. Reflex inhibition may arise from the cardiovascular system, from the lung and chest wall, or from somatic and visceral afferents.
- 22. Control of ventilation: Health & Disease- Dr M A Nazrul 22
- 23. Control of ventilation: Health & Disease- Dr M A Nazrul 23 AGE CSA is more prevalent in older individuals than in middle-aged adults. Sleep state oscillations may precipitate central apnea in older adults Children have risk of obstructive sleep apnea if they have adenotonsillar hypertrophy SEX Women are less susceptible to the development of hypocapnic central apnea during NREM sleep compared with men. Administration of testosterone to healthy premenopausal women for 12 days resulted in an elevation of the Apnea Threshold(AT) and a diminution in the magnitude of hypocapnia required for induction of central apnea during NREM sleep. Conversely, suppression of testosterone with leuprolide acetate in healthy men decreased the AT. GENETIC FACTORS Several transcription factors are responsible for control of breathing. The transcription factor Dbx1 is essential for pre-Böt C development; deletion of Dbx1 eliminated all pre-Böt C glutamatergic respiratory neurons, with complete elimination of inspiratory activity RTN development is particularly vulnerable to a PHOX2B mutation that causes congenital central hypoventilation syndrome (CCHS) in humans
- 24. Control of ventilation: Health & Disease- Dr M A Nazrul 24 OBESITY The obesity-related disorders of obstructive sleep apnea and hypoventilation are fairly well defined, obesity also impacts other conditions such as asthma and chronic obstructive pulmonary disease.
- 25. Control of ventilation: Health & Disease- Dr M A Nazrul 25 Summary 1. History 2. Controller 3. Effector 4. Sensor 5. Loop gain 6. Sleep state and disorders 7. Several factors
- 26. Control of ventilation: Health & Disease- Dr M A Nazrul 26 THANK YOU