A study on prescription pattern and rational use of statins in tertiary care ...
Absolute Final PIP poster!!
1. Nursing and Beers Criteria:
An Intervention to Reduce Potentially Inappropriate Medication Use for
Patients in a Long-term Care Facility
N. Farkas, A. Hall, R. Ober, K. Robinson, A. Sansone, G. Smith
Pace University College of Health Professionals, Lienhard School of Nursing
Table 1 (continued from page 1)
Table 1 (continued on page 3)PAGE 2
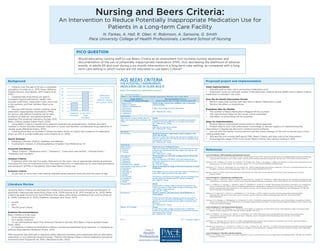
TABLE 1: 2012 AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults
Organ System/
Therapeutic Category/Drug(s)
Recommendation, Rationale,
Quality of Evidence (QE) & Strength of Recommendation (SR)
Antispasmodics
Belladonna alkaloids
Clidinium-chlordiazepoxide
Dicyclomine
Hyoscyamine
Propantheline
Scopolamine
Avoid except in short-term palliative care to decrease
oral secretions.
Highly anticholinergic, uncertain effectiveness.
QE = Moderate; SR = Strong
Antithrombotics
Dipyridamole, oral short-acting* (does not
apply to the extended-release combination with
aspirin)
Avoid.
May cause orthostatic hypotension; more effective alternatives
available; IV form acceptable for use in cardiac stress testing.
QE = Moderate; SR = Strong
Ticlopidine* Avoid.
Safer,effective alternatives available.
QE = Moderate; SR = Strong
Anti-infective
Nitrofurantoin Avoid for long-term suppression; avoid in patients with
CrCl <60 mL/min.
Potential for pulmonary toxicity; safer alternatives available; lack of
concentration in the urine.
QE = Moderate; SR = Strong
Cardiovascular
Alpha1
blockers
Doxazosin
Prazosin
Terazosin
Avoid use as an antihypertensive.
High risk of orthostatic hypotension; not recommended as routine
treatment for hypertension; alternative agents have superior risk/
QE = Moderate; SR = Strong
Alpha agonists
Clonidine
Guanabenz*
Guanfacine*
Methyldopa*
Reserpine (>0.1 mg/day)*
-
ers as listed.
High risk of adverse CNS effects; may cause bradycardia and
orthostatic hypotension; not recommended as routine treatment
for hypertension.
QE = Low; SR = Strong
Antiarrhythmic drugs (Class Ia, Ic, III)
Amiodarone
Dofetilide
Dronedarone
Flecainide
Ibutilide
Procainamide
Propafenone
Quinidine
Sotalol
harms than rhythm control for most older adults.
Amiodarone is associated with multiple toxicities, including thyroid
disease, pulmonary disorders, and QT interval prolongation.
QE = High; SR = Strong
Disopyramide* Avoid.
Disopyramide is a potent negative inotrope and therefore may
induce heart failure in older adults; strongly anticholinergic; other
antiarrhythmic drugs preferred.
QE = Low; SR = Strong
Dronedarone
heart failure.
Worse outcomes have been reported in patients taking drone-
general, rate control is preferred over rhythm control for atrial
QE = Moderate; SR = Strong
Digoxin >0.125 mg/day Avoid.
In heart failure, higher dosages associated with no additional
may increase risk of toxicity.
QE = Moderate; SR = Strong
AGS BEERS CRITERIA
FOR POTENTIALLY INAPPROPRIATE
MEDICATION USE IN OLDER ADULTS
FROM THE AMERICAN GERIATRICS SOCIETY
Literature Review
Using the Beers Criteria can decrease the incidence of adverse drug events through identification of
potentially inappropriate prescribing (Ryan et al., 2009; Kojima et al., 2012; Kanaan et al., 2013). Beers
Criteria has been found to be more effective than other prescription screening tools such as (Ryan et
al., 2009; Vishwas et al., 2012) (Stafford, Alswayan, and Tenni, 2011):
• STOPP
• IPET
• The McLeod Criteria
Guideline Recommendations:
Beers Criteria is to be used:
• As an educational tool
• As a quality measure
• On an individualized basis (The American Geriatrics Society 2012 Beers Criteria Update Expert
Panel, 2012).
• In instances of planning medication initiation, reviewing established drug regimens, or changing an
existing drug regimen (Bergman-Evans, 2012).
PIMs should be discontinued or adjusted unless deemed necessary and substituted with an alternative
medication or non-pharmacological therapy. Patients still taking a Beers criteria medication should be
monitored more frequently for ADEs (Bergman-Evans, 2012).
Proposed project and Implementation
Initial Implementation:
• Educate staff on their role in preventing medication error
• Implement a pop up reminder system in the electronic medical record (EMR) when a Beers Criteria
medication is entered in the chart
Over the Six-Month Intervention Period:
• Monitor steps that nursing staff take when a Beers medication is used
• Monitor the effect on prescribing
Evaluation after Six Months:
• The number of Beers medications flagged will be counted
• The interventions taken by the nurses will be evaluated
• The effect on prescribing will be analyzed
Steps for Implementation:
• Present idea to institutional review board to obtain approval
• Present idea to Arch Care Information Technology to discuss logistics of implementing the
intervention in SigmaCare electronic medical record software
• Discuss with the facility nursing director and the nurse manager of the unit to secure buy-in from
nursing leadership
• Educate the unit nursing staff about PIMs, Beers Criteria, and their role in the intervention
• Encourage the usage of the most recent Beers Criteria: new version coming in 2015
References
Level of Evidence I: EBP Guidelines and Systematic Reviews
The American Geriatrics Society 2012 Beers Criteria Update Expert Panel (2012). American Geriatrics Society Updated Beers Criteria for Potentially
Inappropriate Medication Use in Older Adults. Journal of the American Geriatrics Society, 60, 616–631. doi: 10.1111/j.1532-5415.2012.03923.x
Patterson, S.M., Cadogan, C.A., Kerse, N., Cardwell, C.R., Bradley, M.C., Ryan, C., & Hughes, C. (2014). Interventions to improve the appropriate use of
polypharmacy for older people. The Cochrane Library, 10, 1-117. doi: 10.1002/14651858.CD008165.pub3
Kaufmann, C.P., Tremp, R., Hersberger, K.E., & Lampert, M.L. (2014). Inappropriate prescribing: a systematic overview of published assessment tools.
European Journal of Clinical Pharmacology, 70(1), 1-11. doi: 10.1007/s00228-013-1575-8.
Bergman-Evans, B. (2012). Improving medication management for older adult clients. Retrieved from http://www.guideline.gov/content.
aspx?id=37826
Level of Evidence II: Randomized controlled trials:
Kojima, G., Bell, C., Tamura, B., Inaba, M., Lubimir, K., Bianchette, P.L., Iwasaki, W., & Masaki, K. (2012). Reducing cost by reducing polypharmacy: the
polypharmacy outcomes project. Journal of the American Medical Directors Association, 13(9), 818.e11-818.e15. doi: 10.1016/j.jamda.2012.07.019
Ryan, C., O’Mahony, D., Kennedy, J., Weedle, P., Barry, P., Gallaghert, P., & Byrne, S. (2009). Appropriate prescribing in the elderly: an investigation
of two screening tools, Beers criteria considering diagnosis and independent of diagnosis and improved prescribing in the elderly tool to
identify inappropriate use of medicines in the elderly in primary care in Ireland. Journal of Clinical Pharmacy and Therapeutics, 34, 369-376.
doi: 10.1111/j.1365-2710.2008.01007
Dedhiya, S. D., Hancock, E., Craig, B. A., Doebbeling, C. C., & Thomas, J. (2010). Incident use and outcomes assosciated with potentially
inappropriate medication use in older adults. American Journal of Geriatric Pharmacotherapy, 8(6), 562-570. doi:10.1016/S1543-
5946(10)80005-4
Vishwas, H. N., Harugeri, A., Parthasarathi, G., & Ramesh, M. (2012). Potentially inappropriate medication use in Indian elderly: comparison of Beers’
criteria and Screening Tool of Older Persons’ potentially inappropriate prescriptions. Geriatric & Gerontology International, 12(3), 506-514. doi:1
0.1111/j.1447-0594.2011.00806
Level of Evidence IV: Non-Experimental Research
Curtain, C.M., Bindoff, I.K., Westbury, J. L., & Peterson, G.M. (2013). A comparison of prescribing criteria when applied to older community based
patients. Drugs & Aging, 30, 935-943. doi: 10.1007/s40266-013-0116-6
Desai, R., Williams, C.E., Greene, S.B., Pierson, S., and Hansen, R.A. (2011). Medication errors during patient transitions into nursing homes:
characteristics and association with patient harm. American Journal of Geriatric Pharmacotherapy, 9(6), 413-422. doi: 10.1016/j.
amjopharm.2011.10.005
Stafford, A. C., Alswayan, M. S., & Tenni, P. C. (2011). Inappropriate prescribing in older residents of Australian care homes. Journal of Clinical
Pharmacy and Therapeutics, 36, 33–44 doi:10.1111/j.1365-2710.2009.01151.x
Kanaan, A. O., Donovan, J. L., Duchin, N. P., Field, T. S., Tjia, J., Cutrona, S. L., & ... Gurwitz, J. H. (2013). Adverse Drug Events After Hospital Discharge
in Older Adults: Types, Severity, and Involvement of Beers Criteria Medications. Journal Of The American Geriatrics Society, 61(11), 1894-1899.
doi:10.1111/jgs.12504
Level of Evidence V: Narrative Literature Review
Wittich, C.M., Burkle, C.M., & Lanier, L.M. (2014). Medication errors: an overview for clinicians. Mayo Clinic Proceedings, 89(8), 1116-1125. doi: 10.1016/j.
mayocp.2014.05.007
Would educating nursing staff to use Beers Criteria as an assessment tool increase nursing awareness and
documentation of the use of potentially inappropriate medication (PIM), thus decreasing the likelihood of adverse
events, in adults 65 and over during a six-month intervention in a long term care setting, as compared with a long
term care setting in which nurses are not educated to use Beers Criteria?
PICO QUESTION
• Patients over the age of 65 are a vulnerable
population (Curtain et al., 2013; Desai, Williams,
Greene, Pierson, and Hansen, 2011; Kojima et al.,
2012).
• Inappropriate prescribing can lead to
increased hospital admissions, health care
provider staff times, medication costs, and costs
to the patients and their families (Ryan et al.,
2009).
• Nursing staff should monitor patients using
potentially inappropriate medications (PIMs)
for serious side effects including risk for falls,
incidence of delirium, and gastrointestinal
bleeding (The American Geriatrics Society 2012
Beers Criteria Update Expert Panel, 2012).
• Using Beers Criteria is beneficial for patients experiencing polypharmacy, multiple providers,
multiple or recent transfers between long term or acute care facilities, complicated drug regiments or
unclear goals (Bergman-Evans, 2012).
• Training physicians to use Beers Criteria has been shown to reduce the incidence of medication
errors as well as overall healthcare costs (Kojima et al., 2012)
Search Strategy:
• Databases utilized: CINAHL, PubMed, and Medline.
• 5 systematic reviews, 2 clinical guidelines included; Total References: 14
Keywords and phrases:
• “Beers Criteria”; “Medication error”; “Geriatrics”; “Long-term care facility”; “Nursing home”;
“Morbidity and mortality”
Inclusion Criteria:
• Published within the last five years; Relevance to the topic; Use of appropriate statistical analyses;
Discussed the cost of medication errors; Discussed reduction in medication error; Described prevalence
and predictors of PIMs in the elderly; Described Beers Criteria use;
Exclusion criteria:
• Acute-care or short-term care setting; Samples where patients were less than 65 years of age.
Background
0
Inpatient
Facilities
Long-Term
Care
Facilities
2
4
6
8
10
12
14
Medication
Error Rate
(Wittich, Burkle,
and Lanier, 2014)