getpdf
- 2. 527
n o v e m b e r / d e c e m b e r 2 0 11 , v o l . 6 9 , n o 11
© Van Zuiden Communications B.V. All rights reserved.
On 6 February 2010, a 50-year-old female patient
was admitted to a local hospital complaining of
sudden dropping of the left eye’s visual acuity. B-scan
ultrasonogram showed retinal detachment but failed to
demonstrate a solid subretinal mass. A few days later, the
same patient complained of hoarseness of her voice. On 6
March 2010, the otolaryngologist found paralysis of the
left vocal cord, through the laryngoscope. The patient was
referred to our hospital for the blurred vision of the left eye
and hoarseness of her voice. Her visual acuity was 20/20 in
the right eye and HM/5 cm in the left eye. Ophthalmoscope
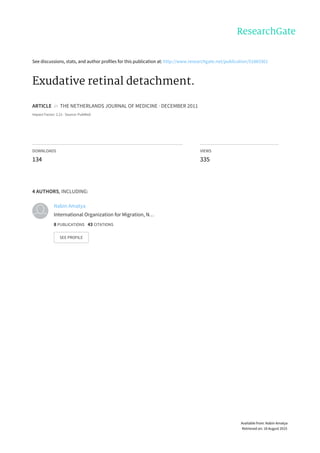
revealed exudative retinal detachment (figure 1). Contrast-
enhanced CT scan confirmed an enhanced lesion on the
temporal side of the left eyeball with a dense central area.
Ultasonography showed a mass of about 21x8 mm, 7 mm
thick, without acoustic shadowing or gradual decay (figure
2). Meanwhile, the ribbon-shaped hyper-zone between
the papilla optica and para-lens were seen. On 9 April
2010, the patient developed a lung infection; computed
tomography (CT) of the chest demonstrated a mass in the
hilum of left lung (figure 3). The biopsy was performed and
the histopathology examination confirmed that the mass
was small lung cell carcinoma.
P h o t o qu i z
Exudative retinal detachment
M. Zhu1
, A. Tang2
, N. Amatya3
, L. Qiu1*
Department of Diagnostic Ultrasound, Ophthalmology, Radiology, West China Hospital of Sichuan
University, Sichuan, China, *
corresponding author: tel.: +86 02881899311, fax: +86 02885423192,
e-mail: zhumengjiaoer@yahoo.com
W h a t i s y o u r d i a g n o s i s ?
See page 530 for the answer to this photo quiz.w
Figure 1. The exudative retinal detachment on the
temporal side of left eyeball without retinal tears
Figure 2. Sonogram of the lesion with hyperecho
ribbon-shaped
Figure 3. Enhanced chest computed tomography revealed
a large mass in the hilum of the left lung. The mass was
diagnosed as small cell lung cancer by bronchoscopic
biopsy
- 3. 530
n o v e m b e r / d e c e m b e r 2 0 11 , v o l . 6 9 , n o 11
© Van Zuiden Communications B.V. All rights reserved.
DIA G NOSIS
Symptomatic choroidal metastases from lung cancer
are only found in a minority of patients.1
Visual loss
with retinal detachment is a rare clinical complication
of small cell lung cancer.2-4
To our best knowledge, this
patient is unique in that she had choroidal metastases and
exudative retinal detachment as the presenting sign of
small cell carcinoma of the lung. The lesion radiologically
mimics choroidal melanoma complicated with retinal
detachment. The diagnosis is confirmed by bronchoscopic
biopsy of the mass, which is shown to be small lung
cell carcinoma through histopathology examination.
The patient responded to systemic chemotherapy and
radioactive plaque therapy. It should not be ignored that
choroidal solitary mass might also originate from the
lung. The aetiology and nature of the lesion should be
well investigated, in particular when the vision loses
expeditiously within a short period.
A n s w e r t o ph o t o qu i z ( pa g e 5 2 7 )
Exu d a t i v e r e t i n a l d e t a chm e n t
R e f e r e n c e s
1. Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520
eyes with uveal metastases. Ophthalmology. 1997;104(8):1265-76.
2. Leys A. Choroidal metastasis and retinal pigment epithelial tear in a
patient with small cell lung carcinoma. Retina. 2000;20(2):216-7.
3. Fernandes BF, Fernandes LH, Burnier MN. Choroidal mass as the
presenting sign of small cell lung carcinoma. Can J Ophthalmol.
2006;41(5):605-8.
4. John VJ, Jacobson MS, Grossniklaus HE. Bilateral choroidal metastasis
as the presenting sign of small cell lung carcinoma. J Thorac Oncol.
2010;5(8):1289.
Dabigatran etexilaat (Pradaxa®
, Boehringer Ingelheim) is
een nieuwe orale directe, reversibele trombineremmer die
sinds enkele jaren wordt gebruikt voor primaire preventie
van veneuze trombo-embolische (VTE) aandoeningen
bij volwassen patiënten na een electieve totale heup- of
knievervangende operatie. Sinds augustus 2011 is het middel
tevens geregistreerd voor de preventie van beroerte en
systemische embolie bij patiënten met atriumfibrilleren*.
Momenteel bestaat nog relatief weinig klinische ervaring
met dabigatran bij atriumfibrilleren. Echter, artsen worden in
toenemende mate geconfronteerd met patiënten die dit middel
gebruiken, waarmee zij voor nieuwe klinische situaties kunnen
komen te staan. Om artsen bij deze soms nog ongewone
klinische situaties te ondersteunen heeft een multidisci-
plinaire klankbordgroep van medisch specialisten het Zakboek
dabigatran ontwikkeld.
Dit zakboek vormt een praktische leidraad bij bijzondere
vragen en situaties die zich kunnen voordoen tijdens het
gebruik van dabigatran. Zo worden onder meer pragmatische
adviezen gegeven over hoe te handelen bij noodsituaties zoals
acute chirurgische ingrepen, bloedingen of een verdenking op
overdosis. Door de insteek vanuit de dagelijkse praktijk vormt
het Zakboek dabigatran een nuttige aanvulling op de reguliere
productinformatie. Gebruik van de leidraad wordt dan ook van
harte aanbevolen aan alle artsen die vanuit hun specialisme in
aanraking kunnen komen met patiënten die worden behandeld
met dabigatran.
Prof. dr. H.R. Büller,
internist AMC Amsterdam en voorzitter Klankbordgroep dabigatran
Meer informatie
Het Zakboek dabigatran is online beschikbaar en aan te vragen
via www.zakboek-dabigatran.nl.
*Non-valvulair atriumfibrilleren en één of meer risicofactoren
ONLAN G S V ERS C H ENEN
Zakboek dabigatran
Een leidraad voor gebruik in bijzondere situaties