2. OBJECTIVES
• Describe shock and underlying pathophysiology
• Compare clinical findings of compensatory, progressive, and irreversible stages of shock
• Describe differences and similarities in shock states related to hypovolemia,
cardiogenic, neurogenic, anaphylaxsis and sepsis
• Discuss complications of shock
• Discuss nursing interventions and evaluate outcomes of patients experiencing shock
3. SHOCK… A CLINICAL SYNDROME
• Life threatening response to alterations in circulation… hemodynamic changes
• Inadequate tissue perfusion
• Imbalance between cellular O2 supply & demand
• Inadequate end-organ perfusion (liver, kidney, intestine, heart, lungs, brain)
• Results in ↓ supply of O2 & nutrients required to sustain normal cellular metabolism.
IMPACTS ALL BODY SYSTEMS MOF DEATH
Influenced by...
• Functioning of compensatory mechanisms
• Successful /timely interventions
4.
5. CARDIOVASCULAR SYSTEM
Closed system: heart, blood, vascular bed
• Vascular bed: arteries, arterioles, capillaries, venules, veins
Functions:
• Delivery of oxygen and nutrients to cells
• Removal of metabolic waste products
• Regulation of blood volume, HR, BP
• Constricts/dilates to regulate blood flow
6. PATHOPHYSIOLOGY:
• Shock begins with CARDIOVASCULAR SYSTEM FAILURE.***
Alterations in at least ONE of four components:
• Blood volume (preload)
• Myocardial contractility CO
• Blood flow
• Vascular Resistance / Afterload (vasoconstriction vs. vasodilation)
7. REGULATION OF BLOOD FLOW:
• BP= product of CO & SVR
• When CO or SVR is low… BP ↓
Decreases in BP = Decreases in CO / SVR
• Leads to vasoconstriction
(attempting to ↑ venous return / BP)
• ↓ flow through the vessel resulting in the
inability to keep the vessel open.
• Compensatory mechanisms:
vasoconstriction, ↑ HR
32. ASSESSMENT:
CNS
• Most sensitive to early changes…
first system affected by changes in
cellular perfusion.
• Initial stage: restless, agitation,
anxiety r/t hypoxemia
• Late stage: confusion, lethargy,
coma r/t inadequate perfusion
33. ASSESSMENT: CARDIOVASCULAR
Initial compensatory stages—
• Normal or slightly elevated SBP
• Diastolic has to work harder at rest (↑ DBP)
=Narrow pulse pressure
Late stages—
• Drop in SBP
• Pulses: weak, thready r/t peripheral vasoconstriction
• Delayed capillary refill
34.
35.
36. GENERAL MANAGEMENT
OF SHOCK:
General management of shock:
• Treat underlying cause*
• Reverse altered circulatory component
COMBINATION THERAPY:
• Fluid
• Pharmacotherapy
• Mechanical therapy (mechanical ventilation)
• Minimize oxygen consumption
37.
38.
39. GENERAL MANAGEMENT
OF SHOCK:
MAINTAIN CIRCULATING VOLUME… Correct alterations in fluid balance.
• IV fluids to restore volume
• Maintain oxygen carrying capacity supplemental O2 or mechanical ventilation
• Restore hemodynamic stability vasopressors
• Choice of fluid, volume, and rate of infusion:
-Depend on fluid lost & current hemodynamic status
-FVO vs FVD, treated very differently.
40.
41. FLUID RESUSCITATION:
BLOOD PRODUCTS: PRBCs, FFP, Platelets, cryoprecipitate
• Treat major blood loss & provide clotting factors
CRYSTALLOIDS:
• 0.9% NS, 0.45% NS, LRs, 3% hypertonic saline, 5% Dextrose
- Inexpensive and readily available
- Classified by tonicity (volume expanders, etc)
- Large volumes precipitate hemodilution… assess Hgb/Hct
- Need to give blood products along with crystalloids to
prevent hemodilution.
COLLOIDS: Albumin
- Avoided w. ↑ capillary permeability.
2 Large-Bore IVs:
• Peripheral: 14 / 16 gauge
• Central Access
42.
43.
44. HEMODYNAMICS
Physical Factors Regulating Blood Flow…
Cardiac Output (CO):
• Amount of blood pumped by the heart per minute.
• (Normal: 4-8 L/min)
Cardiac index (CI):
• Amount of blood pumped by the heart per minute per BSA (height/weight)
• (Normal: 2.4-4 L/min/m2)
• More accurate, individualized.
Stroke Volume (SV):
• Amount of blood pumped out the heart with each beat.
• Measured by a PAC and is reported as C.O.
45. Five factors influence blood pressure:
• Cardiac output
• Peripheral vascular resistance
• Volume of circulating blood
• Viscosity of blood
• Elasticity of vessels walls
HEMODYNAMICS
BP INCREASES WITH…
↑ C.O.
↑ PVR
↑ BV
↑ blood viscosity
↑ rigidity / stenosis of vessels
46. C.O. = HR x SV
CI = (HR x SV) / BSA
• Both HR & SV affect C.O.
• Sepsis = initially ↑ C.O.
(Fever, vasodilation = less SVR).
• As sepsis progresses…SVR ↑ + C.O. ↓
HEMODYNAMICS
↑ HR, SV is unchanged = ↑ CO
47. COMPENSATORY CHANGES:
HEMODYNAMICS
Stroke volume: preload, afterload, contractility
PRELOAD:
Amount of stretch of the myocardium prior to contraction.
End diastolic pressure (EDBP)
Measured by PAC
• Right heart preload: CVP
Normal: 0-8 mmHg
• Left heart preload: PAOP/PAWP
Normal 8-12 mmHg
Tells us the FX of left-side of heart.
48. Afterload: the amount of work the heart has to do to eject blood.
• Resistance the heart encounters is from the blood vessels.
• Heart and lung afterload determined by:
- Diameter of the vessel
- Vasodilation / vasoconstriction
- Valves, Viscosity, and Flow Patterns
• Systemic vascular resistance (SVR): LEFT side of the heart.
• Pulmonary vascular resistance (PVR): RIGHT side of the heart
COMPENSATORY CHANGES:
HEMODYNAMICS
49.
50. SVR & PVR
• MAP: True driving pressure for peripheral blood flow.
• Normal 60-100 mmHg
• MPAP: Mean pulmonary artery pressure
• SVR: LEFT side of the heart.
• PVR: RIGHT side of the heart
Close relationship btwn. SVR / PVR and C.O.
***When CO ↑…. SVR / PVR ↓
(Vasodilation)
55. AFTERLOAD—
• Vasoconstrictors / vasopressors for TX of LOW afterload.
• ↑ vascular tone = ↑ SVR = ↑ BP
• Contraindicated in hypovolemic shock…
-FVD… don’t have the volume needed to ↑ BP.
• Vasodilators to reduce HIGH afterload.
CONTRACTILITY—
• Positive inotropic agents (dopamine, dobutamine)
• ↑ contractile force
=↑ workload of heart complications
PHARMACOLOGICAL MANAGEMENT:
56. Other medications:
• Sedatives:↓ HR / anxiety
• Analgesics: pain
• Insulin: BS rises when under stress
• Corticosteroids: assess hyperglycemia!
• Antibiotics
• Sodium bicarbonate: tx metabolic acidosis when pH<7.0
PHARMACOLOGICAL MANAGEMENT:
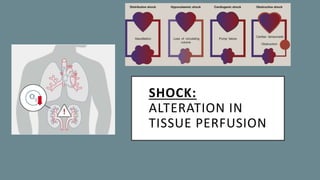
57. TYPES OF SHOCK:
• HYPOVOLEMIC = inadequate intravascular volume, FVD (trauma, surgery) need
volume replacement
• CARDIOGENIC = inadequate myocardial contractility, poor pump, back-up of fluid
• OBSTRUCTIVE = obstruction of blood flow, blockage (tumors, etc)
• DISTRIBUTIVE = (neurogenic, anaphylactic, sepsis): inadequate vascular tone
- Maldistribution of circulating blood.
- Have right amt of volume, it’s just not in the right place.
- ↓ vagal tone.
Each has a unique mechanism causing an…
Alteration in Tissue Perfusion
58.
59.
60. HYPOVOLEMIC SHOCK
• Overall ↓ in vascular volume
• The most common shock syndrome
• Blood volume is insufficient to fill the intravascular space
ACTUAL HYPOVOLEMIA: EXTERNAL fluid loss, actual volume loss.
• Hemorrhage, surgery, trauma, diarrhea, diuresis, burns.
RELATIVE HYPOVOLEMIA: INTERNAL FLUID SHIFT from the
intravascular space into the interstitial or intracellular space.
• Third spacing, leaky capillary syndrome, pleural effusion
• Fluid moves out of vessels into tissues ANASARCA
61.
62. HYPOVOLEMIC SHOCK:
CLINICAL PRESENTATION
↓ BP
↓ CO, ↓CI
↓ RAP, PAP, PAOP
↓ SvO2
↓ Hct (if from blood loss)
↓ urine output
↑ HR
↑SVR
↑ RR
↑ Hct (if from dehydration)
• Oliguria
• Cool, pale skin
• Altered LOC
• Flat neck veins
64. MILD:
• Blood volume deficit of 0-10% or 500cc.
• ↓ venous return, ↓ CO
• ANS compensates: vasoconstriction & inc. myocardial
contractility to maintain MAP and CO.
MODERATE:
• Blood volume ↓ by 15-20% = ↓ CO and arterial pressure
• ↓ blood flow to the liver, pancreas, kidneys, GI tract:
• Oliguria, kidney failure, high BUN/creatinine
• Hypoactive bowel sounds, abd. distention
• Generalized venoconstriction: helps ↑ venous return
• Tachycardia (>100bpm) in attempts to ↑ blood volume
• Tachypnea
• ↓ pulse pressure
• Cool / clammy , mottled skin,↓ cap refill
• Anxiety = acidosis, low cerebral perfusion
SEVERE:
• Blood volume deficit >25%
• Other small losses create major
↓ in CO, BP, and tissue perfusion.
• Brain and myocardium are subject
to a fall in perfusion.
• All compensatory mechanisms are
functioning at MAX CAPACITY!!
• Significant tachycardia (>140 bpm)
• Increase RR respiratory failure
• Severe hypotension
• Anuria
• Confusion, anxious, agitated,
obtunded, eventually comatose.
65.
66. NURSING INT:
HYPOVOLEMIC SHOCK
• Modified trendelenburg
• Control hemorrhage, apply pressure
• Infusion of blood products (O-neg universal donor)
FLUID REPLACEMENT:
• ISOTONIC CRYSTALLOIDS: ↑ preload, ↑ SV, ↑ CO
• NS (can cause ↑ Na+/Cl-) or LRs (can cause buildup
of lactate)
**will often switch btwn the two to avoid these issues.
• Colloidal solution (ALBUMIN):
• Pulls fluid back into intravascular space.
• Volume expander
67. 3:1 RULE FOR CRYSTALLOIDS:
• For every 1 mL of approximate blood
loss, 3 mL of crystalloid solution is
given.
• PRBCS: helps replace fluid and provides
Hgb, which will carry O2 to deprived cells
• Platelets: for uncontrolled bleeding to
help with thrombocytopenia.
• Fresh Frozen Plasma: for when the
patient needs clotting factors.
MONITOR FOR FVO:
• Elevated CVP or PAWP
• Crackles
• Edema
• JVD Collect labs:
Hgb/Hct, lactate level (status of cell’s metabolism),
blood gases (acidosis?), electrolytes, BUN/
68.
69. CARDIOGENIC SHOCK:
Primary dysfunction: inadequate
myocardial contractility / weak
pumping action of heart.
• Approx 80% of cases of cardiogenic
shock are fatal.
Most common etiology:
Damage from MI & impairment of the
myocardial pumping ability.
• Left ventricle is the primary pump
Left ventricular dysfunction:
• Measured by PAP/PAOP
• ↓ CO
• Blood backs up in to pulmonary system
• Pulmonary congestion occurs
Right ventricular dysfunction:
• Measured by RAP/CVP
• Blood backs up into venous circulation
• Reduces available SV for each heartbeat
• Systemic congestion occurs
70. CARDIOGENIC SHOCK:
CAUSES
• Myocardial infarction
• Cardiomyopathy
• Dysrhythmias:
- ↓ efficiency of myocardial contractions.
- ↓ amt of blood pumped out of the ventricle
per minute = inadequate organ perfusion
• CHF
• VSD
• Rupture of ventricular wall
• Disorder of the myocardium, valves, or
electrical conduction system
• Valvular dysFX
• In cardiogenic shock,
there is NOT an issue
with a loss of blood
volume.
• Blood volume is
normal.
• However, bc the heart is
not FX properly…blood
volume starts to back
up:
• Causes congestion in
the lungs & the right
71. CARDIOGENIC SHOCK:
PATHO. & HEMODYNAMICS
• Heart is unable to provide adequate SV and CO/CI
• ↓ SV = ↓ CO = ↓ TISSUE PERFUSION
SV: amt/ of blood pumped out of the heart with each beat… 65-135 ml)
• ↑ SVR
• Compensatory mechanisms (catecholamine release)
• ↑ PAOP (volume in the left ventricle at end of filling time)
• Distention of ventricle
• Transmits to pulmonary bed (↑ PAP and ↑ PAOP)
• JVD (backing all the way up into right side), peripheral
edema, systemic effects.
• Oxygen supply does not meet demand
• End-organ failure
74. ↑ PAOP/PAWP (>18 mmHg):
• Normal 8-12 mmHg
• Swan-Ganz catheter is inserted through the right side of the heart &
wedged in pulmonary artery.
• Balloon is temporarily inflated to measure LEFT ATRIAL FILLING PRESSURE.
• >18 mmHg in cardiogenic shock bc blood is backing up in the heart & lungs
= HIGH PRESSURE IN LEFT ATRIUM.
↑ CVP/ RAP:
• Catheter used to measure the pressure in the right atrium and SVC.
• Normal: 2-8 mmHg
• Backflow of blood to the right side of the heart (right atrium into venous
circulation) leads to VENOUS CONGESTION = ↑ CVP.
77. CARDIOGENIC SHOCK—
DIAGNOSTICS
• CBC—assess Hgb / Hct levels
• EKG –assess area of heart being effected
• ABG –to correct imbalances
• Type and cross-match
• Blood chemistry (electrolytes)
-Hypokalemia: dysrhythmias
-Hyperkalemia: Peaked T-waves,indicates renal failure.
• Coronary angiography—assess obstructions in coronary
arteries, do they need a stent to inc. perfusion to
myocardium?
• Echocardiogram—structures / blood flow / valve FX /
myocardial contractility / size of chambers / estimates EF
• Nuclear scans
78. CARDIOGENIC SHOCK—
NURSING INT.
• HOB elevated –reduce afterload
• Bedrest: ↓ cardiac demand
• Supplemental O2: ↓ cardiac workload by reducing tissue demands, maintain oxygenation
due to pulmonary edema
• IV fluids (used with caution) – optimize preload
• Inotropic agents:↓ afterload & improves myocardial contractility = ↑SV, ↑CO
• Diuretics: ↓ pulmonary congestion & FVO.
• Use torsemide for pts who are insensitive to Lasix.
• Pain medication (morphine) vasodilation
DO NOT PUT IN TRENDELENBURG… due to ↑ pulmonary congestion.
• This ↑ resistance for the heart to beat against (uphill)
• Will worsen tissue perfusion and pulmonary edema.
79. DIURETICS: cardiogenic shock doesn’t have a ↓ in blood volume. (same with neurogenic shock)
• Fluid backs up into lungs from an injured heart that is failing to pump blood forward.
• Furosemide (K+ wasting, monitor for hypokalemia): HELPS REMOVE EXCESS FLUID.
• ↓ preload = ↓ workload of heart
• Monitor for FVD and worsening hypotension
VASOPRESSORS: cause vasoconstriction = ↑ preload (venous return) = ↑ SV & CO
• Norepinephrine: ↑ tissue perfusion by ↑ BP
- Doesn’t cause tachydysrhythmias.
• Dobutamine: ↑ contractility & CO
- Can cause vasodilation worsening hypotension
• Dopamine: ↑ contractility / BP / MAP
- Monitor for tachydysrhythmias
80. VASODILATORS: ↓ preload / afterload = ↑ SV = ↑ CO
• ↓ workload of heart by dilating the coronary arteries.
• CAN CAUSE HYPOTENSION!!! MONITOR BP CLOSELY!
• May not be used if the pt is severely hypotensive
• Nitroglycerin or Sodium Nitroprusside
IV FLUIDS: used with EXTREME CAUTION r/t pulmonary edema!!!
• Normal saline (if even used)
• A fluid challenge is majorly used for the other types of shock when blood volume is the issue…
…remember in cardiogenic shock blood volume is NOT the issue.
Heart is a weak pump!! IABP for mechanical support
81. CARDIOGENIC SHOCK—
NURSING INT.
High cardiac markers:
• ↑ troponin: released if there is injury to heart cells.
• ↑ BNP: released by the cells that make up the ventricles when they stretch due to high BV.
• Pulmonary edema on chest x-ray
• Echocardiogram will show a low E.F.
• Acid-base levels will demonstrate acidosis
• Serum lactate >4 mmol/L
• Cells switch from aerobic anaerobic metabolism, which will produce lactic acid.
• pH <7.35
• ↑ lactic acid = ↓ O2 perfusion
82. Intra-aortic balloon pump (IABP):
• Mechanical device used to ↓ myocardial
oxygen demand while ↑ CO.
• ↑ CO = ↑ coronary blood flow and
myocardial oxygen delivery.
• Used in cardiogenic & other shock states.
↓ workload of heart
↓ afterload
↓ myocardial oxygen consumption
↑ CO
↑ coronary artery perfusion
INFLATES during diastole:
displaces / pushes blood out to coronary arteries.
DEFLATES during systole:
helps empty coronary arteries
83. OBSTRUCTIVE SHOCK:
• Blockage (physical obstruction) of circulation
prevents venous return.
↓ preload (venous return) = ↓ CO
• No ↓ in intravascular volume or vasodilation
of the intravascular space.
• ↓ CO from a drop in preload
(rather than myocardial dysfunction).
• Impaired venous return because of high
pressure surrounding right atrium.
• Need to alleviate or repair the obstruction.
Mostly surgical interventions.
Examples:
- P.E.
- Dissecting aortic aneurysm
- Atrial tumor
- Pericardial tamponade
creates pressure around heart
- Tension pneumothorax
displaces great vessels,
tracheal shift, ↑ ITP = ↓ CO
- Ruptured diaphragm with
evisceration of contents into
the abdominal cavity:
**will hear bowel sounds
in the chest.
84.
85. ↑ HR
↑ or normal RAP, PAP, PAOP
↑ PVR and SVR
↓ BP
↓ CO / CI
↓ SvO2
↓ urine output
↓ LOC
• Dyspnea
• Dysrhythmias
• Chest pain
• Oliguria (↓ kidney perfusion)
• Cool, pale skin
• JVD
OBSTRUCTIVE SHOCK:
CLINICAL PRESENTATION
87. P.E.
• Right ventricular failure
• SOB
• Hemoptysis
• TX: fibrinolytics & anticoagulants
AORTIC DISSECTION:
• Ripping chest pain
• Pulse difference btwn left & right side
• Widened mediastinum
OBSTRUCTIVE SHOCK:
CLINICAL PRESENTATION
88. DISTRIBUTIVE / VASOGENIC SHOCK:
Septic, Neurogenic, Anaphylactic:
• Systemic vasodilation = ↓ SVR
• Maldistribution of blood flow / intravascular volume
• Loss of intravascular volume from ↑ capillary permeability and ↓ vascular tone
Massive vasodilation = larger vascular capacity = RELATIVE HYPOVOLEMIA =
↓ preload = ↓ CVP, ↓ PAOP = ↓ CO
• Major goal: stop the cause of vasodilation & return the circulating volume to the intravascular
space to improve tissue perfusion.
• FLUID RESUS. FIRST…THEN VASOPRESSORS (want vessels to constrict to ↑ tissue perfusion)
90. Loss of sympathetic vasoconstrictor tone in
the vascular smooth muscle
• Impaired autonomic function
• Body unable to use compensatory
mechanisms (increasing HR) r/t a
sympathetic blockade and dominance of
the PSNS.
Bradycardia ONLY SHOCK
STATE WITH BRADYCARDIA.
• ↓ preload (venous return) = ↓ SV and CO
NEUROGENIC SHOCK:
91.
92. CAUSES: Disease / injury to the spinal cord an interruption of impulses from the SNS.
• SCI at or above T6
• General or spinal anesthesia, epidural block
• Drugs that cause CNS depression: barbiturates, phenothiazines, etc.
• Severe pain
• Hypoglycemia
FIRST-LINE TX:
• Fluid replacement (monitor carefully)
• Maintain MAP >65: higher than other shock states bc we really want to ↑ cerebral perfusion
• Epi/ N.E. –stimulate SNS to ↑ HR & BP through vasoconstriction
NEUROGENIC SHOCK:
93. • Bradycardia with hypotension
• Warm, dry, flushed skin due to lack
of vascular tone vasodilation
• Hypothermia due to impaired
thermoregulation (damaged
hypothalamus)
NEUROGENIC SHOCK:
CLINICAL PRESENTATION
↓ HR
↓ BP
↓ temp.
↓ CO/CI
↓ RAP, PAP, PAOP
↓ SVR
↓ SvO2
↓ urine output
94. • Immobilization of spinal injuries (backboard, cervical collar)
• Maintain MAP and adequate HR
• IV fluids for hypotension
• Vasopressors (only after volume replaced)
• Slow rewarming to prevent further vasodilation EVEN LOWER BP.
• VTE prophylaxis
NEUROGENIC SHOCK:
NURSING INT.
95. ANAPHYLACTIC SHOCK:
Acute / potentially life-threatening massive allergic reaction:
• Sensitized person is exposed to an antigen.
• Reaction causes direct damage to the vascular wall.
• Cells throughout the body release vasoactive mediators (histamines &
prostaglandins) that trigger a systemic response.
↑ capillary permeability = mvmt of fluid into the interstitial space =
RELATIVE HYPOVOLEMIA
• Vasodilation = ↓ BP = ↓ CO = hypoperfusion
• Bronchospasms may occur from release of chemical mediators
99. SEPTIC SHOCK
• Most common type of
circulatory shock.
• 750,000 cases of
sepsis/septic shock per year
• Incidence is on the rise.
• 30 % mortality rate
• Nosocomial infection
• Critically ill pts at high risk
INCREASING INCIDENCE R/T…
• Elderly
• Immunocompromised pts
• Comorbidities
• More extensive utilization of long-
& short-term invasive devices
(catheters, indwelling devices,
central lines)
• Resistant organisms
100. SEPTIC SHOCK
• Microorganism invades the body
• Triggers immune response activation of
biochemical inflammatory mediators
• Inflammation = ↑ capillary permeability
fluid seeping from the capillaries
• Vasodilation & ↓ BP = inadequate perfusion =
↓ O2 and nutrients to the cells MODS
101. WARM STAGE:
Hyperdynamic / Progressive
• ↑ CO
• ↑ HR
• ↑ RR
• Systemic vasodilation
• Hyperthermia / febrile / flushed
• Mental Status changes
• U/O normal or ↓
• GI: N/V/D, hypoactive bowel sounds
COLD STAGE:
Hypodynamic / Irreversible
• Low CO
• Rapid HR/RR
• Vasoconstriction, hypoTN (↓BP)
• Skin cool and pale
• ↓ temp.
• Oliguria (<400cc/day) Anuria
• MSOF: can lead to cardiogenic shock!!!
-The more organs that begin to fail, the
higher the morbidity/mortality rate.
TWO PHASES OF SEPSIS:
102.
103.
104. SEPTIC SHOCK:
ASSESSMENT
PULMONARY:
• Respiratory failure may require
mechanical ventilation
• ↓ O2 sats (SaO2)
• Breath sounds:
• crackles and wheezes r/t
pulmonary congestion.
• Assess pt response to mechanical
ventilation & ventilator changes.
• ABGs
CARDIOVASCULAR:
• Persistent hypoTN: SBP <90 or
dropped 40 from baseline SBP)
• Pale / Cool / clammy skin
• ↓ capillary refill
• ↑ CO
• ↓ SVR
Progressive sepsis:
• ↓ CO, ↑ CVP, ↑ PAP caused
by fluid backup in lungs
105. SEPTIC SHOCK:
ASSESSMENT
HEMATOLOGIC:
• Hypocoagulable state bc using up all
the clotting factors.
• Increased risk bleeding, immature
clotting factors DIC
• Bruising, petechiae
• Hematuria
• Guaic stool (can have GI bleeding)
• ↓ Hgb/Hct
RENAL:
• Monitor U/O q1-2h
• Assess peripheral edema
• Monitor BUN/Creatinine, GFR
• Is kidney FX improving?
Getting worst?
• Dehydration can cause elevated
BUN / creatinine IVF
• If creatinine continues to ↑…
there is ↓ in KIDNEY PERFUSION.
106. SEPTIC SHOCK:
ASSESSMENT
GI: FX is interrupted
• Sepsis hyperglycemia DKA / HHS
• Elevated bilirubin, glucose and LFT’s from liver dysfx hematological changes
• NUTRITION IS A PRIORITY enteral preferred over parenteral
• Enteral gives bacteria in gut something to work on.
• Prevents bloodstream infections from GI bacteria.
• Assess residual should be <300cc
• If ↑ residual… stop tube feeding, then reassess volume.
• If ↓ residual… run tube feeding at a lower rate.
• Consult w dietician… what type of enteral feedings will be best for this pt?
107. SURVIVING
SEPSIS
CAMPAIGN
CARE BUNDLES
WITHIN 3 HRS OF SEVERE SEPSIS…
1. Measure lactate levels to determine the
presence of tissue hypoperfusion.
• Normal: 0.3-0.8 mmol/L
• Lactic acidosis > 4mmol/L
2. Obtain blood cultures x2 BEFORE administration of ABX.
3. Administer broad-spectrum ABX
• Covers both gram+ and gram-
• Adjust ABX when results of culture & sensitivity are in.
4. Give 30 mL/kg crystalloids for hypotension or lactate >4
• 2.5L of fluid usually required
108. SURVIVING
SEPSIS
CAMPAIGN
CARE BUNDLES
WITHIN 6 HRS OF INITIAL S&S OF SEPTIC SHOCK…
5. Administer vasopressors for…
• hypoTN that does not respond to initial fluid resuscitation
to maintain MAP ≥ 65.
• MUST BE GIVEN VIA CENTRAL LINE…caustic to veins.
• Hemodynamic monitoring in place.
6. In the event of persistent arterial hypotension despite
volume resuscitation (septic shock) or initial lactate ≥4
mmol/L (36 mg/dL):
• Measure CVP & central venous O2-sat
7. Remeasure lactate level if initial level was elevated.
• LACTATE SHOWS PERFUSION. Did the fluids help?
Goal of fluid resuscitation:
• CVP >8 mmHg
• central venous O2-sat of >70%
• return of lactate level to normal.
109.
110. • Hand Hygiene
• Aseptic technique
• Identify cause of infection (culture blood, body fluids, devices, catheter tips, etc).
• Remove / replace access devices
• Antibiotic therapy
• Fluid replacement
• Drain abscesses (drains)
• Goal directed therapy
GREATEST RISK: immunocompromised & the elderly
SEPTIC SHOCK: MANAGEMENT
111. QSOFA—HELPS NURSES IDENTIFY
PTS WITH SUSPECTED SEPSIS.
• Quick
• Sepsis-Related
• Organ
• Failure
• Assessment
Measured by 3 Criteria:
• Altered Mental Status
• Increased RR
• Decreased BP
113. • Physiologic imbalance btwn. compensatory inflammatory &
anti-inflammatory response to immune system activation
Three main processes occur:
• Inflammation
• Hypercoagulation
• Impaired fibrinolysis
• Endothelial activation
SEPTIC SHOCK: PATHO.
114. • WBCs release cytokines
• Myocardial depressant factor (MDF) released
causes ↓ E.F.
• ↓ response to fluid resuscitation
• Excessive inflammation and coagulation
damages the endothelium resulting in
capillary leak.
• Fluid shifts into the tissues causing more
inflammation and edema.
• Difficulty maintaining homeostasis
• Resulting organ dysfunction
1) INFLAMMATION
115. • Inflammation initiates coagulation cascade
• Endothelial injury and cytokine release
• Thrombin production
• Further inflammation
• Unregulated thrombin
• Thrombin transforms soluble fibrinogen into fibrin
• Fibrin combines with circulating platelets to form clots
• Clots become microemboli
Fibrin + platelets clot formation microemboli clogging
up capillaries necrosis of digits
2) HYPERCOAGULATION
116. • Epithelial injury in sepsis impairs fibrinolysis.
• The balance between clot removal and clot
development is delayed.
• Alteration of coagulation cascade leads to DIC
3) IMPAIRED FIBRINOLYSIS
121. SYSTEMIC INFLAMMATORY
RESPONSE SYNDROME (SIRS)
• Widespread systemic inflammatory response
Associated with diverse disorders:
• Infection
• Trauma
• Shock
• Pancreatitis
• Ischemia
**Most frequently associated with sepsis.
SIRS is a precursor to MOFS
122. SYSTEMIC INFLAMMATORY
RESPONSE SYNDROME (SIRS)
• Normally localized process becomes systemic.
• SIRS is a precursor to MOFS
• Release of mediators:
• ↑ endothelial & capillary permeability
• Fluid shifts into intravascular spaces
• ↓ intravascular volume = RELATIVE
HYPOVOLEMIA
123. SIRS
CRITERIA:
• Tachycardia (HR>90)
• RR >20 or PaCO2 < 32 mmHg
• Hyperthermia (>38 C) or Hypothermia(<36 C)
• WBC count >12,000 or <4,000
• Hypotension
• Hyperglycemia
• ↓ U/O
• Peripheral edema
• Mottling (r/t vasoconstriction in skin)
• Mental status changes
(poor brain perfusion irritability, confusion)
AT RISK POPULATIONS:
• <1 y.o. and >85 y.o.
• Immunocompromised
• Trauma
• Intra-abdominal surgery
• Gastric bypass**
• Pancreatitis
• Cirrhosis
• Meningitis
• Chronic disease (CV, renal, diabetes)
• Cellulitis
• UTI
• Burns
124. DISSEMINATED INTRAVASCULAR
COAGULOPATHY (DIC)
• Acquired Syndrome
• Secondary to another primary illness
• Intravascular stimulation (activation)
of the clotting cascade
• Severe Thrombosis
• Depletion of mature clotting factors
hemorrhage
125. DIC: PATHO.
• Systemic disorder
• Generation of intravascular fibrin with the consumption of coagulation factors / platelets
• Initiation of coagulation through endothelial or tissue injury
• Clots are formed in the absence of injury, thrombin production is uncontrolled
• Stable clotting cannot form hemorrhage
• Platelet aggregation
• Consumption of coagulation factors
• Excessive plasmin is produced in response to intravascular thrombi
• Degradation of fibrinogen, fibrin, and other coagulation factors
• Fibrinolysis enhances hemorrhage
Positive D-dimer: evidence that DIC is present
129. ACUTE:
• Sepsis
• Massive trauma
• Rapid initiating event
• Rapid change in lab values
• Generalized bleeding
• Petechiae to exsanguination
• Microcirculatory &
macrocirculatory thrombosis
• Hypoperfusion, infarction,
and organ damage
CHRONIC:
• Retained dead fetus
• Cancer
• Large abdominal aneurysm
• Mildly reduced platelets
• Slightly increased D-dimer level
• May have little bleeding or no
symptoms at all.
DIC: ACUTE VS CHRONIC
130. ASSESSMENT OF DIC:
Overt bleeding or oozing:
• Epistaxis
• Hematuria
Signs of platelet deficiency:
• Petechiae
• Ecchymosis / Mottling
• Microhemorrhages
• Broken blood vessels
• Pinpoint red dots
Hypoperfusion of organs:
• Mental status changes
• Infarction of tissues in extremities
• Hemodynamic instability / shock
131. • ↓ platelets
• ↓ fibrinogen
• Prolonged PT, aPTT, thrombin time
• Elevated FDP & FSP
• ↓ in coagulation factors
• ↓ Hgb/Hct
• ↑ d-dimer
DIAGNOSTICS OF DIC:
132.
133. • Correct underlying cause
• Administer blood products
- Platelets
- FFP
- RBCs
- Cryoprecipitate (frozen coag. factors)
- Take 20 mins to thaw.
- Thaw bags back-to-back to prevent delay in care.
• Stop abnormal coagulation
• Prevent injury & bleeding
TREATMENT OF DIC:
134. MULTIPLE ORGAN DYSFUNCTION
SYNDROME (MODS)
• Altered organ function
Primary MODS:
• Direct tissue insult…leads to impaired perfusion or ischemia.
Secondary MODS:
• Inadequate tissue perfusion r/t secondary disease process.
• Septic shock
• SIRS
AT RISK PTS:
• advanced age, malnutrition, co-morbidities contribute to development of MODS
135. MULTIPLE ORGAN DYSFUNCTION
SYNDROME (MODS)
Maldistribution of blood flow to various organs:
• Impaired tissue perfusion
• Decreased oxygen supply to cells
Organs severely affected / first organs compromised:
• Lungs
• Splanchnic bed
• Liver
• Kidneys
Respiratory failure kidney failure
138. MODS:
NURSING INT.
• Treat the underlying cause / infection
• Provide adequate oxygenation, may
need mechanical ventilation
• Provide adequate tissue perfusion
• Volume resuscitation
• Placement of a central line
• Support organ function
• Supportive care
• Nutritional support: albumin
142. VASOPRESSORS
NOREPINEPHRINE***
first line TX in most shocks
• Sepsis, cardiogenic shock
• Undifferentiated shock
• 1-30 mcg/min
• ↑ tissue perfusion by ↑ BP
- Doesn’t cause tachydysrhythmias.
143. VASOPRESSIN:
used for shock & with GI bleeds
DOSAGES ARE ENTIRELY DIFFERENT
• Septic shock (2nd line)
• Vascular , GI smooth muscle & anti-
diuretic effects
• Coronary & splachnic constriction
• 0.01-0.04 units/min (no titration)
VASOPRESSORS
144. VASOPRESSORS
DOPAMINE:
• Cardiogenic shock
• Septic shock (2nd line)
• Increased risk tachy-arrhythmias
• 1-20 mcg/kg/min
• Not always best drug…
↑ contractility / workload of heart
High doses: ↑ SVR and BP
Early int: IVF, ABX, Blood products
More cautions with fluid replacement… limited IVF to prevent pulmonary edema & peripheral edema.
Capillaries emboli
Vasoconstriction compensatory mechanism
Dec. CO = dec tissue perfusion
SNS activated : inc renin-angiotensin cycle
Renal: vasoconstriction, conserves water & sodium to inc. preload
ADH helps inc. preload
**risk for MI or HF bc heart is working so hard
END PRODUCT: want to restore tissue perfusion
Correct low BP as quickly as possible (initial)
Correct low BP as quickly as possible (initial)
Frank-Starling principle:
increasing the end-diastolic volume (EDV) results in a corresponding increase in the SV
Anasarca: fluid leaking from skin r/t FVO and inc. pressure
Doesn’t stay in intravascular space, moves into tissues
Dec. fluid in intravascular space = dec. BP
Necrotic bowel r/t dec. perfusion to GI tract
Anasarca: fluid leaking from skin r/t FVO and inc. pressure
Doesn’t stay in intravascular space, moves into tissues
Dec. fluid in intravascular space = dec. BP
Necrotic bowel r/t dec. perfusion to GI tract
Enhanced clotting; using up mature factors very quickly, the only clotting factors left are immature / don’t clot well.
Cardiogenic: too much fluid, heart is not pumping well.
Obstructive: something blocking the blood flow inc. CVP
Respiratory alkalosis to try and correct metabolic acidosis
Metabolic acidosis results from HYPOPERFUSION & BUILD-UP OF LACTIC ACID.
Important to follow lactic acid values to determine perfusion status after interventions.
**Remember that lactic acidosis is a cause of metabolic acidosis.
Epi, N.E., vasopressin IV infusions
-weight based
There is a difference in how these meds are dosed
Limit on IVF administration, will start using vasopressors
Need to be able to deliver large volumes of fluids.
Central access: can’t administer large volumes as quickly
Cordis, thread triple lumen thru it = 4 accesses
SV increasing in importance
High CVP: FVO, heart failure
Low CVP: FVD, need IVF
PAOP: LEFT-SIDED: 16-18 mmHg suggests fluid is backed up in lungs / pulmonary congestion… will hear crackles.
Right side: peripheral edema, JVD ONLY OCCURS WITH COMBINED RIGHT & LEFT HF.
MAP 60: adequate perfusion
Titrate meds based on what the MAP is.
Balloon is not inflated until it’s in R atrium.
Blood flow carries it to pulmonary artery reflective of left-sided heart FX
Fill the tank (give fluid) before you give vasopressors / squeeze it.
Vasopressors ↑ SVR / BP
Relative: fluid isn’t in the intravascular space like it should be
Relative: fluid isn’t in the intravascular space like it should be
Baroreceptors in chest help to inc. BP, but they are short-lived.
AB+ universal recipient
If the stroke volume falls (meaning the heart muscle is NOT pumping blood very well), the cardiac output decreases and this leads to a fall in tissue perfusion.
↓ SV (amount of blood pumped out of the heart with each beat… 65-135 ml)
↑ SVR
↓ blood flow to kidneys activates RAAS retention of Na+ and water, dec. urine output
if preload is increased (which is the amount the ventricle stretches at the end of diastole) the stroke volume will increase hence delivering a higher cardiac output… vasopressors can achieve this by causing vasoconstriction, which will increase venous return to the hear
Intra-aortic balloon pump: dec. workload of heart, inc. coronary artery perfusion
Inflates during diastole: displaces / pushes blood out to coronary arteries
Deflates during systole: helps empty coronary arteries
if preload is increased (which is the amount the ventricle stretches at the end of diastole) the stroke volume will increase hence delivering a higher cardiac output… vasopressors can achieve this by causing vasoconstriction, which will increase venous return to the hear
if preload is increased (which is the amount the ventricle stretches at the end of diastole) the stroke volume will increase hence delivering a higher cardiac output… vasopressors can achieve this by causing vasoconstriction, which will increase venous return to the hear
if preload is increased (which is the amount the ventricle stretches at the end of diastole) the stroke volume will increase hence delivering a higher cardiac output… vasopressors can achieve this by causing vasoconstriction, which will increase venous return to the hear
if preload is increased (which is the amount the ventricle stretches at the end of diastole) the stroke volume will increase hence delivering a higher cardiac output… vasopressors can achieve this by causing vasoconstriction, which will increase venous return to the hear
No problem with vasodilation / vasoconstriction
Dec, in CO r/t drop in preload (rather than myocardial dysFX)
Have right amt of volume, but vessels cant constrict enough to maintain BP.
Vessels are so dilated, there is less resistance / dec. afterload …. =inc. CO
Less resistance, CO will inc.
Vasodilation low SVR inc. CO
Inc. preload, dec. afterload
MODIFIED Trendelenburg: raise the knees (passive leg raise)
Initially will have inc. CO bc dec. SVR
When it progresses… dec CO,
ONLY SHOCK STATE W BRADYCARDIA .
Dec vascular tone… cant vasoconstrict dec SVR
NEUROGENIC SHOCK: want MAP to be higher to inc. cerebral perfusion
Other shocks: MAP = 60
Need to have enough volume on board before vasopressors
Need to have enough volume on board before vasopressors
Shellfish, nuts, eggs
Penicillin, ABX (meds)
Bee stings
RELATIVE HYPOVOLEMIA: Maldistribution of blood flow… have enough volume, its just not in the correct space. (moves into interstitial space)
Elderly pts w comorbidities do not have as reactive of an immune response why there’s an inc. in mortality rate
d/c central lines peripheral IV
Sterile technique is of upmost importance!
AM cares: clean around foley
Elderly pts w comorbidities do not have as reactive of an immune response why there’s an inc. in mortality rate
d/c central lines peripheral IV
Sterile technique is of upmost importance!
AM cares: clean around foley
Inc lactate metabolic acidosis respiratory alkalosis in attempts to compensate for the acidosis
Poor CO, poor tissue perfusion affects kidneys, dec urine output… LOW U/O MAY BE FIRST SIGN OF AN ISSUE.
Noninvasive monitoring is inc.
PAC used to monitor CO, CVP, PA pressures
Dehydration can cause elevated BUN / creatinine IVF
If creatinine continues to rise…there is dec. in KIDNEY PERFUSION.
Ultrasound to assess fluid in jugulars.
Targets for quantitative fluid resuscitation included in the guidelines are a CVP >8 mmHg or greater, central venous oxygen saturation of at
least 70%, and return of lactate level to normal.
Targets for quantitative fluid resuscitation included in the guidelines are a CVP >8 mmHg or greater, central venous oxygen saturation of at
least 70%, and return of lactate level to normal.
MANY MEDS ARE CAUSTIC TO VEINS WHEN GIVEN PERIPHERALLY… central lines may be needed in order to deliver some of these meds
(meds gets diluted in a larger volume & is in a larger vessel than peripheral)
Get peripheral IVs in FIRST before d/c central access.
If on vasopressors… NEED TO BE GIVEN THRU A CENTRAL LINE!!! Need hemodynamic monitoring also.
Monitor for abscesses esp. after GI surgery
CT scan visualize any abscesses
Drains to remove fluid from abscess
A bedside prompt that may ID patients with suspected infection who are at risk for a poor outcome.
Two or more criteria suggests > risk of a poor outcome.
While 1 in 4 infected patients have 2+ QSOFA points, they account for 3 out of 4 deaths
A bedside prompt that may ID patients with suspected infection who are at risk for a poor outcome.
Two or more criteria suggests > risk of a poor outcome.
While 1 in 4 infected patients have 2+ QSOFA points, they account for 3 out of 4 deaths
Damage to endothelium inc. capillary permeability / leaking
Total disruption of coagulation cascade
Fibrin + platelets clots / microemboli necrosis of digits
Microemboli clog up capillaries necrosis of digits
Total disruption of coagulation cascade
Fibrin + platelets clots / microemboli necrosis of digits
Microemboli clog up capillaries necrosis of digits
Hose w pinpoints… leaking fluid out of capillaries into interstitial spaces dec intravascular volume
Want blood sugars <150
>200, may be started on insulin drips
Result of another process
D-dimer used to assess presence of clots
Issues with clotting factors
Using up all mature clotting factors
TX: FFP, platelets, vit. K
D-dimer used to assess presence of clots
Coagulation: apt, pt & INR
D-dimer used to assess presence of clots
***Need to look at all of these to DX
Takes 20 mins to thaw
Thaw bags back-to-back to prevent delay in care… get one after the other.
Maldistribution of blood flow to multiple organs
Maldistribution of blood flow to multiple organs
NX: albumin, total protein values
NX: albumin, total protein values
Have max. doses/rates
VASOPRESSORS: cause vasoconstriction = ↑ preload (venous return) & ↑ CO
Norepinephrine: ↑ tissue perfusion by ↑ BP
Doesn’t cause tachydysrhythmias.
Dobutamine: ↑ contractility & CO
Can cause vasodilation worsening hypotension
Dopamine: ↑ contractility / BP / MAP
Monitor for tachydysrhythmias
NE vasopressin
Vasopressin use for GI bleed: hope the drug constricts bleeding GI vessel to stop bleeding
Have max. doses/rates
VASOPRESSORS: cause vasoconstriction = ↑ preload (venous return) & ↑ CO
Norepinephrine: ↑ tissue perfusion by ↑ BP
Doesn’t cause tachydysrhythmias.
Dobutamine: ↑ contractility & CO
Can cause vasodilation worsening hypotension
Dopamine: ↑ contractility / BP / MAP
Monitor for tachydysrhythmias
Dopamine & dobutamine mostly used in cardiogenic shock… iNOTROPIC AGENTS. Inc workload of heart, can cause tachycardias, and can even worsen hypoTN… monitor these pts closely