ISBARR The purpose of this project is to practice formulat.docx
Paramedic Chiefs Canada Poster
1. Utilisation of non-transport Low Acuity Pathway (LAP) Protocols by
NSW Ambulance paramedics in the rural and regional setting
INTRODUCTION
Management of low acuity patient presentations is an important issue for
many ambulance services, arsing from the increased demand in these patient
presentations(1-4)
, which impact on both ambulance and Emergency Department (ED)
service delivery.
NSW Ambulance trialled the Clinical Assessment and Referral pilot project in
metropolitan and major regional centres, with evaluation of the project in 2010
identifying positive outcomes, including increased proportion of patients non-
transported and reduced case cycle times of 34 minutes(5)
. In 2011, NSW Ambulance
transitioned the Clinical Assessment and Referral pilot project into clinical practice
for all qualified paramedics, becoming known as Low Acuity Pathways, with training
completed in June 2012(6)
.
Low Acuity Pathways provide patients presenting with specific low acuity
conditions(1)
, treatment and referral pathways rather than transportation to an
ED. Patients are identified suitable for non-transport through the application of
systematic patient assessments, generic exclusions and protocol specific exclusion
criteria(5, 7, 8)
.
The Low Acuity Pathway program is the ‘flagship’ clinical initiative by NSW
Ambulance for addressing the issue of low and sub-acute patient presentations
to qualified paramedics. Extended Care Paramedic specialists provide qualified
paramedics a clinical referral option, clinical support systems and access to health
networks, in addition to their extended scope of clinical practice.
The introduction of new clinical practice radically different to previous practice needs
to be evaluated in order to ascertain whether the perceived and desired outcomes
are being met. As rural and remote areas have distinctively different health demands,
needs and resources, it is important to understand how Low Acuity Pathway
protocols are being utilised in these areas.
AIM
To describe Low Acuity Pathway utilisation in rural and remote regions since their
integration into standard paramedic practice in NSW Ambulance.
METHODS
• A retrospective cohort study analysing routinely collected clinical data documented
by NSW Ambulance paramedics was undertaken.
• Inclusion Criteria: 1) Patient participants had an emergency or urgent (priority 1 or
2) ambulance response between March 1 2011 and February 29 2012; 2) aged >16
years; and 3) had a recognised low acuity pathway recorded in the protocol section
of their paramedic clinical record.
• This data was linked with computer sided dispatch data and analysed using SAS
9.2 to produce descriptive statistics, compare proportions and frequencies.
FINDINGS
• Of the 568,927 cases analysed, 97,509 resulted non-transport disposition after
assessment by paramedics, reporting a non-transport rate of 16.8%.
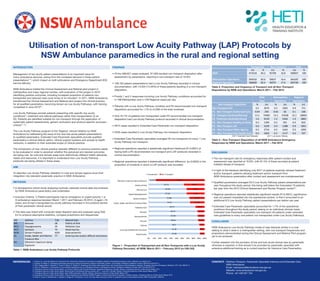
• 108,163 patient presentations had a Low Acuity Pathway recorded in clinical
documentation, with 13,504 (14.26%) of these patients resulting in a non-transport
disposition.
• Priority 1 and 2 responses involving Low Acuity Pathway conditions accounted for
n=188 Metropolitan and n=109 Regional cases per day.
• Patients with a Low Acuity Pathway condition and P5 recommended non-transport
disposition accounted for <1% (n=3,239) of the total workload.
• Only 44.7% of patients non-transported under P5 recommended non-transport
disposition had Low Acuity Pathway protocol recorded in clinical documentation.
• 2674 cases resulted in Extended Care Paramedic non-transport disposition.
• 3239 cases resulted in Low Acuity Pathway non-transport disposition.
• Extended Care Paramedic specialists averaged 46 non-transports for every 1 Low
Acuity Pathway non-transport.
• Regional operations reported a statistically significant likelihood (P<0.0001) of
having both a P5 recommended non-transport and LAP protocols recorded in
clinical documentation.
• Regional operations reported a statistically significant difference (p=0.0003) in the
proportion of incidents in which a LAP protocol was recorded.
DISCUSSION
• The non-transport rate for emergency responses after patient contact and
assessment was reported at 16.8%, with 87.4% of these recorded at patient
initiated refusal of transport.
• In light of the literature identifying only 8%(9)
of patients explicitly refused treatment
and/or transport, patients refusing treatment and/or transport from
NSW Ambulance paramedics after contact and assessment are overrepresented.
• Qualified paramedics averaged 33.3 Low Acuity Pathway patient presentations per
year throughout the study period, this being well below the forecasted 70 patients
per year from the 2010 Clinical Assessment and Review Program review(5)
.
• Regional operations reported statistically significant results (P<0.0001), significance
was not present translated into the operational context, in that it amounted to an
additional 8.3 Low Acuity Pathway patient presentations per station per year.
• Extended Care Paramedic specialists accounted for 1.7% of the operational
workforce throughout the study period, seeing on an individual clinician basis
Extended Care Paramedic specialists non-transport 46 patients under extended
care guidelines to every one patient non-transported under Low Acuity Pathways.
CONCLUSION
NSW Ambulance Low Acuity Pathway model of care behaves similar in a rural
setting to what it does in a metropolitan setting, with non-transport frequencies and
proportions demonstrated during the Clinical Assessment and Referral Pilot program
yet to be achieved.
Further research into the provision of low and sub-acute clinical care by paramedic
clinicians is required, in that should it be provided by paramedic specialist with
extensive additional training as is current practice for Intensive Care Paramedics.
M4 Asthma T18 Wound Care
M9 Seizures S8 Elderly at Risk
M11 Hypoglycaemia S9 Palliative Care
M17 Epistaxis T4 Head Injuries
M18 Dental Problems M29 Gastroenteritis
E6 Snake, Spider and Marine
Creature Bite
T7 Limb Injuries and/or difficult extrication
D4 Oleoresin Capsicum Spray
Exposure
91.66
91.46
90.6
88.46
87.68
87.27
83.77
74.22
72.88
67.92
67.89
63.13
12.29
8.34
8.54
9.4
11.54
12.32
12.73
16.23
25.78
27.12
32.08
32.11
36.87
87.71
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Head Injuries
Limb injuries/Difficult Extrication
Asthma
Seizures
Gastroenteritis
Epistaxis
Palliative Care
Snake, Spider and Marine Creature Bites
Dental Problems
Hypo/Hyperglycaemia
Wound Care
Elderly At Risk
Oleoresin Capsicum Spray Exposure
Transported Non-Transport
Table 1. NSW Ambulance Low Acuity Pathway Protocols
Figure 1 - Proportion of Transported and all Non-Transports with a Low Acuity
Pathway Recorded, all NSW, March 2011 – February 2012 (n=108,163)
Transported Non-Transport Total
(n) % (n) % (n) %
NSW 473218 83.2 95709 16.8 568927 100
Metropolitan Operations 304550 83.6 59637 16.4 364187 100
Regional Operations 168668 82.4 36072 17.6 204740 100
Table 2. Proportion and frequency of Transport and all Non-Transport
Dispositions by NSW and Operations, March 2011 – Feb 2012
NSW
Total
Metropolitan
Operations
Regional
Operations
Non-transport disposition % (n) % (n) % (n)
Non-Transport ECP 0.5 2674 0.5 1963 0.4 711
P1 - Non Transport Authorised Care 0.04 250 0.02 82 0.1 168
P2 - Transport Declined/Refused 13.1 74483 13.1 47638 13.1 26845
P2- Treatment declined/refused 1.6 9129 1.5 5264 1.9 3865
P3 - Non Transport Healthy at Home 0.3 1394 0.5 561 0.4 833
P5 - Non Transport LAP 0.6 3239 0.4 1388 0.9 1851
P6 – Non Transport Other Agency 0.5 2716 0.5 1624 0.5 1092
P7 – Non Transport Non Health Issue 0.3 1824 0.1 1117 0.4 707
ECP = Extended Care Paramedic LAP = Low Acuity Pathway
Table 3 – Non-Transport Disposition of all NSW Ambulance Emergency
Responses by NSW and Operations, March 2011 – Feb 2012
1. Haines CJ, Lutes RE, Blaser M, Christopher NC. Paramedic initiated non-transport of pediatric patients. Prehospital Emergency Care. 2006 Apr-Jun;10(2):213-9.
2. Squires JP, Mason S. Developing alternative ambulance response schemes: analysis of attitudes, barriers, and change. Emergency Medicine Journal. 2004 Nov;21(6):724-7.
3. Girio-Fragkoulakis C, Gardner C, Cross S, Mason S, Walters S. Assessing the impact older people from care homes place on the emergency services. European Journal of Emergency Medicine. 2011 Apr;18(2):81-5.
4. Gray JT, Wardrope J. Introduction of non-transport guidelines into an ambulance service: a retrospective review. Emergency Medicine Journal. 2007 Oct;24(10):727-9.
5. Ambulance Service of New South Wales. Low Acuity Patient (LAP) Clinical Pathways: Operational Resource. Rozelle, Sydney: Ambulance Service of New South Wales; 2011.
6. Ambulance Service of New South Wales. Study Guide to Scheduled Training January 2011 - June 2012. Rozelle, Sydney: Ambulance Service of New South Wales; 2010.
7. Ambulance Service of New South Wales. Dear CARE paramedic. Rozelle, Sydney: Ambulance Service of New South Wales; 2011.
8. Ambulance Service of New South Wales. Clinical Assessment and Referral (CARE) Program: Central Coast Sector Evaluation. Rozelle, Sydney: Ambulance Service of New South Wales; 2010.
9. Shaw D, Dyas JV, Middlemass J, Spaight A, Briggs M, Christopher S, et al. Are they really refusing to travel? A qualitative study of prehospital records. BMC Emerg Med. 2006;6:8.
REFERENCES: CONTACT: Matthew Simpson, Paramedic Specialist Intensive and Extended Care
NSW Ambulance
Email: mjsimpson@ambulance.nsw.gov.au
Website: www.ambulance.nsw.gov.au
Phone: +61 429 047 754