National TB Control Program (DOTS) Lecture Notes
•
37 likes•3,783 views

The document summarizes key information about tuberculosis (TB) and the Philippines' National TB Control Program (NTP). It outlines the program's vision, mission, goals and objectives, which aim to reduce TB prevalence and mortality. It describes TB transmission, signs/symptoms, diagnosis, treatment regimens and dosages. It also covers management of childhood TB, including case finding, prevention through BCG vaccination, and treatment approaches like DOTS. Nursing responsibilities in childhood TB are also defined.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to National TB Control Program (DOTS) Lecture Notes
Similar to National TB Control Program (DOTS) Lecture Notes (12)
More from MarkFredderickAbejo
More from MarkFredderickAbejo (16)
National TB Control Program (DOTS) Lecture Notes
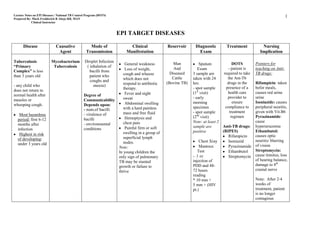
- 1. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 1 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor EPI TARGET DISEASES Disease Causative Mode of Clinical Reservoir Diagnostic Treatment Nursing Agent Transmission Manifestation Exam Implication Tuberculosis Mycobacterium Droplet Infection General weakness Man Sputum DOTS Pointers for “Primary Tuberculosis ( inhalation of And - patient is teaching on Anti- Loss of weight, Exam Complex” is less bacilli from cough and wheeze Diseased 3 sample are required to take TB drugs: than 3 years old patient who which does not Cattle taken with 24 the Ant-Tb coughs and respond to antibiotic (Bovine TB) hrs: drugs in the Rifampicin: taken - any child who sneeze) therapy. - spot sample presence of a befor meals, does not return to Fever and night (1st visit) health care causes red urine normal health after Degree of sweat - early provider to urine measles or Communicability Abdominal swelling morning ensure Isoniazide: causes whooping cough. Depends upon: with a hard painless specimen compliance to peripheral neuritis, - num.of bacilli mass and free fluid - spot sample treatment given with Vit.B6 Most hazardous - virulence of Hemoptysis and (2nd visit) regimen Pyrazinamide: period: first 6-12 bacilli chest pain Note: at least 2 cause months after - environmental Painful firm or soft sample are Anti-TB drugs: hyperurucemia infection conditions swelling in a group of positive (RIPES) Ethambutol: Highest in risk Rifampicin causes optic of developing: superficial lymph nodes. Chest Xray Isoniazid neuritis/ blurring under 3 years old of vision Note: Mantoux Pyrazinamide In young children the Test Ethambutol Streptomycin: only sign of pulmonary - .1 cc Streptomycin cause tinnitus, loss TB may be stunted injection of of hearing balance, growth or failure to PDD and 48- damage to 8th thrive 72 hours cranial nerve reading * 10 mm + Note: After 2-4 5 mm + (HIV weeks of pt.) treatment, patient is no longer contagious
- 2. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 2 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor The National Tuberculosis Control Program Objective C: Increase and sustain support and financing for TB control activities Vision: A country where Tb is no longer a public health problem Mission: Ensure that TB DOTS services are available, accessible and Strategies: affordable to the communities in collaboration with the LGU’s Facilitate implementation of TB-DOTS Center certification and and other partners accreditation Goal: To reduce prevalence and mortality from TB by half the year 2015 ( Millennium Development Goal ) Build TB coalitions among different sectors Targets: Advocate for counterpart input from local government units 1. Cure at least 85% of the sputum smear- positive TB patient discovered. Mobilize/extend other resources to address program limitations 2. Detect at least 70% of the estimated new sputum smear-positive TB cases. Objective D: NTP Objectives and Strategies Strengthen management (technical and operational) of TB control services at all levels Objective A: Improve access to and quality of services provided to TB patients, TB Strategies: symptomatics and communities by health care institutions and providers Enhance managerial capability of all NTP program managers at all levels Strategies: Establish an efficient data management system for both public and Enhance quality of TB diagnosis. private sectors. Ensure TN patient’s treatment compliance. Implement a standardized recording and reporting system. Ensure public and private health care providers adherence to the Conduct regular monitoring and evaluation at all levels. implementation of national standards of care for TB patients. Advocate for political support through effective local governance Improve access to services through innovative service delivery mechanisms for patients living in challenging areas. KEY POLICIES Objective B: Case Finding Enhance the health-seeking behavior on TB by communities, especially the TB symptomatics 1. DSSM ( Direct Sputum Smear Microscopy ) shall be the primary diagnostic tool in NTP case finding. Strategies: Note: No TB diagnosis shall be made based on Xray result alone Develop effective, appropriate and culturally-responsive IEC/communication likewise materials. result of PDD skin test (Mantoux Test) Organize barangay advocacy groups 2. All TB symptomatic identified shall undergo DSSM for diagnosis before start of treatment Note: Only contraindication for sputum collection is hemoptysis
- 3. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 3 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor 3. After three sputum specimen yielding negative result X-ray and culture are necessary RECOMMENDED CATEGORY OF TREATMENT REGIMEN Note: Diagnosis based on Xray shall be made by the TB Diagnostic Committee. Category Type of TB Treatment Regimen 4. Only trained medical technologist or microscopist shall perform DSSM. Patient Intensive Continuation Total Phase Phase Period Patients with the following conditions shall be recommended for New smear hospitalization: positive PTB massive hemoptysis New smear pleural effusion I positive PTB 2 RIPE 4 RI 6 military TB ( TB of the Spine “Pot’s Disease”) with extensive mos. TB meningitis parenchymal TB pneumonia lesion and those requiring surgical intervention EPTB and Severe Anti-TB drugs: concomitant (RIPES) HIV disease Rifampicin Treatment Isoniazid Failure Pyrazinamide II 2 RIPES 5 RIE 8 Relapse Ethambutol Return after /1 RIPE mos. Streptomycin default Two Formulation of Anti-TB Drugs New smear- 1. Fixed-Dose Combination ( FDCs) – two or more first line anti-TB drugs negative PTB are combined in one tablet. There are 2,3, or 4 drug fixed dose III 2 RIP 4 RI 6 With minimal combinations. parenchymal mos. 2. Single Drug Formulation (SDF) – each drug is prepared individually. lession Isoniazid, Pyrazinamide and Ethambuto are in tablet form while Chronic ( still Refer to Specialized facility Rifampicin is in capsule form and streptomycin is injectable. smear-positive or DOTS Plus Center refer IV after supervised to City Provincial NTP re-treatment ) Coordinator
- 4. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 4 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor DOSAGE PER CATEGORY OF TRATMENT REGIMEN B. Single Dose Formulation ( SDF ) A. Fixed-Dose Combination Formulation Simply add 1 tablet of Isoniazid ( 100mg) , Pyrazinamide The number of tablets of FDCs per patient will depend on the body (500mg) and Ethambutol ( 400mg) each for the patient weighing more weight. than 50kg before treatment initiation. Modify drug dosage within acceptable limits according to patient’s body weight, particularly those weighing less than 30 kg at the time of diagnosis. Categories I and III : 2 RIPE / 4 RI ( FDC) Categories I and III: 2 RIPE / 4 RI (SDF) Body Weight No.of tablets per day No. of tablets per day (kg) Intensive Phase Continuation Phase Anti-TB Drugs No. of tablets per day No. of tablets per day ( 2 months ) ( 4 months ) Intensive Phase Continuation Phase FDC-A ( RIPE) FDC-B (RI) ( 2 months ) ( 4 months ) 30 - 37 2 2 Rifampicin 1 1 38 – 54 3 3 Isoniazid 1 1 55 – 70 4 4 Pyrazinamide 2 More than 70 5 5 Ethambutol 2 Categories II : 2 RIPES / RIPE / 4RIE (FDC) Categories II: 2 RIPES / 1 RIPE / 5 RIE Body Intensive Continuation Phase Anti-TB No. of Tablets / Vial per day No.of Tablets per Weight Phase Drugs Intensive Phase day First Months 3rd FDC-B E (3months ) Continuation Phase Two (2) Month ( RI ) 400 ( 5 months ) mg First 2 months 3rd months FDC-A Streptomycin FDC-A Rifampicin 1 1 1 (RIPE) (RIPE) Isoniazid 1 1 1 30 – 37 2 0.75 g 2 2 1 Pyrazinamide 2 2 38 – 54 3 0.75 g 3 3 2 Ethambutol 2 2 2 55 – 70 4 0.75 g 4 4 3 Streptomycin 1 vial per day More 5 0.75 g 5 5 3 than 70 Note: 56 vials of Streptomycin for two months
- 5. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 5 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor Drug Dosage per Kg. Body Weight All TB symptomatic children 0-9 years old, except sputum positive child shall subject to PDD testing Anti-TB Drugs Dose per Kg Body Weight and Maximum Dose - Only trained nurse and midwife shall do the PDD test and recording - Testing and reading shall be conducted once a week either on Monday Rifampicin 5 ( 4 – 6 ) mg/kg and not to exceed 400 mg daily or Isoniazid 10 ( 8 – 12 ) mg/kg and not to exceed 600 mg daily Tuesday. Pyrazinamide 25 ( 20 – 30 ) mg/kg and not to exceed 2 mg daily Note: 10 children shall be gathered for testing to avoid wastage. Ethambutol 15 ( 15 – 20 ) mg/kg and not to exceed 1.2 g daily Streptomycin 15 ( 12 – 18 ) mg/kg and not to exceed 1 g daily A child shall be suspected as having TB and considered symptomatic if with any three (3) of the following sign and symptoms: D.O.T.S ( Directly-Observed Treatment Shortcourse ) “TuTok Gamutan” cough and wheezing for 2 weeks or more unexplained fever for 2 weeks or more 5 Elements of D.O.T.S loss of appetite, loss of weight, failure to gain weight Sustained political commitment failure to respond to a 2 weeks of appropriate antibiotic therapy Access to quality-assured sputum microscopy failure to regain state of health 2 weeks after a viral infection or after Standardized short-course chemotherapy for all cases of TB having measles. Uninterrupted supply of essential drugs Recording and reporting system enabling outcome assessment of all patients A child shall be clinically diagnosed or confirmed of having TB if he and assessment of overall program performance. has any three (3) of the following condition: positive history of exposure to an adult/ adolescent TB case presence of sign and symptoms suggestive of TB MANAGEMENT OF CHILDREN WITH TB positive Mantoux Test abnormal chest radiograph suggestive of TB Prevention Management BCG vaccination shall be given to all infants. BCG vaccine is moderately effective. It has a protective efficacy of: For children with exposure to TB 50 % against any TB disease 64 % against TB meningitis Should undergo physical examination and PDD testing (Mantoux Test) 74 % against death from TB A child with productive cough shall be referred for DSSM, if found positive, treatment shall be started immediately. PDD testing shall no Case Finding longer needed. Cases of TB in children are reported and identified in two instances: Children without sign/symptoms of TB but with positive Mantoux Test - The patient sought consultation. and those with symptoms of TB but negative Mantoux Test shall - The patient was reported to have been exposed to an adult with TB referred for chest x-ray examination.
- 6. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 6 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor For children with signs and symptoms of TB Continuation Phase 10-15 mg/kg body weight A child to have signs and symptoms of TB with either known or unknown 10-15 mg/kg body weight 4 months Rifampicin exposure shall be referred for Mantoux test. Isoniazid For children with known contact but with negative Mantoux and those unknown contact but with positive Mantoux shall be referred for chest x-ray examination. B. Extra Pulmonary TB For a negative x-ray report, Mantoux test shall be repeated after 3 months. Chemoprophylaxis of Isoniazid for 3 months shall be given to children less Drugs Daily Dose (mg/kg per body weight ) Duration than 5 years old with negative chest x-ray after which Mantoux test shall be Intensive Phase repeated Rifampicin 10-15 mg/kg body weight Isoniazid 10-15 mg/kg body weight Treatment Pyrazinamide 20-30 mg/kg body weight D.O.T.S will still be followed just like in adult 2 Short course regimen: Plus months - at least 3 anti-TB drugs for 2 months ( intensive phase ) Ethambutol 15-25 mg/kg body weight - 2 anti-TB drugs for 4 months ( continuation phase ) OR Streptomycin 20-30 mg/kg body weight * For Extra Pulmonary TB Cases: - 4 anti-TB drugs for 2 months ( intensive phase ) Continuation - 2 anti-TB drugs for 10 months ( continuation phase ) Phase 10-15 mg/kg body weight 10-15 mg/kg body weight 10 Rifampicin Domiciliary treatment shall be the preferred mode of care Isoniazid months No treatment shall be initiated unless the patient and health worker has agreed upon a caseholding mechanism for treatment compliance. Public Health Nurse Responsibilities ( Childhood TB ) Treatment Regimen 1. Interview and open treatment cards for identified TB children. 2. Perform Mantoux testing and reading to eligible children A. Pulmonary TB 3. Maintain NTP records 4. Manage requisition and distribution of drugs Drugs Daily Dose (mg/kg per body Duration 5. Assist the physician in supervising the other health workers of the weight ) RHU in the proper implementation of the policies and guidelines Intensive Phase on TB in children. Rifampicin 10-15 mg/kg body weight 6. Assist in the training of other health workers on Mantoux testing 10-15 mg/kg body weight 2 months and reading. Isoniazid Pyrazinamide 20-30 mg/kg body weight
- 7. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 7 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor EPI TARGET DISEASES Disease Causative Mode of Clinical Reservoir Diagnostic Treatment Nursing Agent Transmission Manifestation Exam Implication Diphteria it is an Corynebacterium Respiratory Nasal Man Schick’s Test Antibiotics Isolate patient acute pharyngitis, diphtheriae Droplets dryness of the - test for the until 2-3 cultures acute upper lip susceptibility to Pen G taken at least nasopharyngitis serosanguinous Diptheria Potassium 24hrs apart are or acute laryngitis secretion in the Erythromycin negative with Pseudo nose Moloney Test Small frequent membrane – - for hyper- grayish white in feeding Pharyngeal sensitivity to color with leathery Promote “Bullneck” Diptheria toxin consistency in the absolute rest appearance throat and on the Use ice collar to because of the tonsil relieve pain of enlarge cervical sore throat lymph nodes. May put on soft diet Laryngeal sore throat hoarseness brassy metallic cough Pertussis Bordetella Airborne – At first, the - 100 days cough Pertussis droplet infected child may - Whooping cough Primarily by have a common Erythromycin Place the patient - “tuspirina” direct contact cold with runny Man Bordet- Gengou Agar Ampicillin on NPO during with he nose, sneezing Plate paroxysmal stage discharge from and mild cough - used for - is given 5-7 days to prevent respiratory Intermittent culture medium aspiration mucous episode of membranes of Position prone paroxysmal for infants and infected person cough followed upright for older by a whoop ending vomiting
- 8. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 8 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor Neonatal Tetanus Clostridium Unhygienic Assess the Tetani cutting of NEWBORN for a umbilical cord history of all 3 of the Blood Culture Penicillin Prevention - which produces following: Erythromycin the exotoxins: Improper CSF analysis Tetracycline Aseptic Tetanolysin handling of cord Normal suck and handling of the Tetanospasmin stump esp. when cry for the first 2 - administered neonatal treated with days of life within 4 hours of umbilical cord contaminated Onset of illness Soil injury Tetanus Toxiod substance between 3 and 28 Intestinal immunization for days canal of mothers Inability to suck animal Active followed by Man immunization of stiffness of the DPT body and convulsion In OLDER CHILDREN, the following may be observed: Trismus – lockjaw Opisthotonus – arching of the neck and back Ridus Sardonicus – sardonic smile
- 9. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 9 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor Poliomyelitis 3 Types of Polio Fecal-oral route Abortive - did not Throat swab Strict Isolation “Infantile Virus progress to systemic Man Hot moist Paralysis” Type I Oral route infection Stool exam through compress to Brunhilde pharyngeal Non-paralytic – Lumbar exam relieve spasm Type II Lansing secretion slight involvement of the CNS Pandy’s test Use protective Type III Leon Contact with - for CSF devices: infected person Poker spine or analysis - handroll to stiffness of the prevent claw hand spinal column Spasms of the - trochanter roll, to hamstring prevent outer With paresis rotation of femur - footboard Paralytic – severe involvement of CNS Hoyne’s Sign – head falls back when he is in supine with shoulder elevated Paralysis Head log/drop Tripod position – extend his arm behind for support when he sits up Kernig’s sign Brudzinski sign
- 10. Lecture Notes on EPI Diseases / National TB Control Program (DOTS) 10 Prepared By: Mark Fredderick R Abejo RR, MAN Clinical Instructor Hepatitis B Prodromal/pre- - it is liver Hepa B Virus 3 P’s icteric Liver infection caused by Symptoms of Man Increase CHO Function Test the B type of Person to person URTI Moderate fat hep.virus. Parenteral Weight loss Low CHON It attacks livers the Placental Anorexia liver often RUQ pain Observed universal resulting in Malaise precaution inflammation Icteric Jaundice Acholic stool bile-colored urine 3 C’s Measles Paramyxo Virus Droplet Conjunctivitis Observe Coryza Man respiratory Cough isolation Koplik’s spot – Should kept out bluish gray spot on of school for at the buccal mucosa. least 4 days after Generalized blotch rash appear rash For Photophobic, darkened room, sunglasses