Allergy Induced Acute Coronary Syndrome - Kounis Syndrome

Allergy Induced Acute Coronary Syndrome - Kounis Syndrome: Case Report. Poster used in CMC MAC 2021. OBJECTIVE: To discuss a rare occurrence of allergic reaction to NSAID causing Myocardial Infarction. BACKGROUND: A 21-year-old obese female with no other comorbidities was referred to us with history of chest pain, generalized urticarial rashes and itch suddenly following Inj.IM Diclofenac, which was given for heel pain relief. She was hemodynamically stable, but tachypneic, orthopneic and was having bilateral basal crepitations. ECG revealed significant ST depression & T inversion in II,III,aVF and V2-V6 and ST elevation in aVR. CXR showed pulmonary edema. Diagnosed as ACS following anaphylaxis and loading dose was given along with IM adrenaline, antihistamines, and steroids. Echo revealed global hypokinesia of LV. Cardiac enzymes were elevated. Meanwhile, she had a prompt relief of chestpain, but dyspnea worsened and warranted NIV support. Repeat ECG revealed regression of ST changes correlating with chest pain relief. After 2 days of NIV, patient’s dyspnea improved and weaned from NIV. CAG revealed normal epicardial coronaries. Serial cardiac enzyme levels showed falling trend and ECG was completely normal with no significant ST-T changes. Pre-discharge, repeat echo showed persistence of global hypokinesia. 2weeks later, repeat echo showed dramatic improvement with normal LV systolic function suggesting recovery from myocardial stunning. RESULTS: This qualifies for the diagnosis of MINOCA (Myocardial Infarction with No Obstructive Coronary Arteries). In the setting of allergic trigger, vasospasm or coronary hypersensitivity is the underlying mechanism- described as KOUNIS SYNDROME. CONCLUSION: ECG changes and chest discomforts that occur in allergic reactions are not always secondary to distributive/anaphylactic shock. Sometimes heart could be the primarily affected organ by the allergic reaction as in this case. Although <200cases reported globally until 2017, it’s suspected to be frequently overlooked, hence likely to be more prevalent.
Recommended

Recommended
More Related Content
Similar to Allergy Induced Acute Coronary Syndrome - Kounis Syndrome
Similar to Allergy Induced Acute Coronary Syndrome - Kounis Syndrome (20)
More from Manievelraaman Kannan
More from Manievelraaman Kannan (11)
Recently uploaded
Recently uploaded (20)
Allergy Induced Acute Coronary Syndrome - Kounis Syndrome
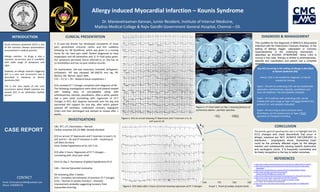
- 1. Dr. Manievelraaman Kannan, Junior Resident, Institute of Internal Medicine, Madras Medical College & Rajiv Gandhi Government General Hospital, Chennai – 03. CLINICAL PRESENTATION INVESTIGATIONS CONCLUSION DIAGNOSIS & MANAGEMENT REFERENCES Figure 1. ECG on arrival showing ST depression and T inversion in II, III, aVF and V2-V6 INTRODUCTION CONTACT KOUNIS SYNDROME Allergy induced Myocardial Infarction – Kounis Syndrome Email: drmvraaman1994@outlook.com Phone: 9789999778 This qualifies for the diagnosis of MINOCA (Myocardial Infarction with No Obstructive Coronary Arteries). In the setting of allergic trigger, vasospasm or coronary hypersensitivity is the underlying mechanism - described as KOUNIS SYNDROME. Since CAG is normal in this case, therapy is limited to antihistamines, steroids and vasodilators and patient had a complete recovery. CBC, RFT, LFT, Electrolytes – Normal Cardiac enzymes (CK,CK-MB): Serially elevated ECG on arrival: ST depression and T inversion in lead II, III, aVF and V2 – V6 and ST elevation in aVR – localising to Left Main territory Echo: Global hypokinesia of LV; IVC:2 cm ECG after 2 hours: Regression of ST-T changes – correlating with chest pain relief Echo on day 2: Persistence of global hypokinesia of LV CAG – Normal Epicardial coronaries On reviewing after 2 weeks: ECG – Complete normalisation of previous ST-T changes Echo – Normal LV systolic function – dramatic improvement probably suggesting recovery from myocardial stunning. The primary goal of reporting this case is to highlight that the ECG changes and chest discomforts that occur in allergic reactions are NOT ALWAYS SECONDARY to distributive / anaphylactic shock. Sometimes heart could be the primarily affected organ by the allergic reaction and subsequently causing systolic dysfunction and cardiogenic shock. It is frequently overlooked and its timely recognition is the key to better outcomes. A 21-year-old female has developed complaints of chest pain, generalised urticarial rashes and itch suddenly following Inj. IM Diclofenac, which was given in a nursing home for her heel pain relief. Patient diagnosed to have anaphylaxis and IM adrenaline and 1L IV fluid bolus given. Her symptoms persisted, hence referred to us. She has no co-morbidities and has no past medical records. On examination, she was conscious, oriented, tachypneic, orthopneic. JVP was elevated. BP:100/70 mm Hg, PR: 96/min, RR: 28/min, SpO2: 90%. CVS —S1 S2 +, RS – Bilateral basal crepitations + ECG revealed ST-T changes compliant with diagnosis of MI. The following investigations were done and patient treated with loading dose of anti-platelets along with antihistamines, steroids, vasodilators. After a while, patient had a pain relief correlating with regression of ST-T changes in ECG. But, dyspnea worsened over the day and warranted NIV support for one day, after which patient weaned off ventilator, underwent coronary angiogram (CAG) and then discharged and advised to review after 2 weeks. 1. https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/s12872-017-0670-7 2. https://www.uptodate.com/contents/clinical-syndromes-of-stunned-or-hibernating- myocardium 3. https://www.clinicaltherapeutics.com/article/S0149-2918(13)00078-7/fulltext 4. https://www.uptodate.com/contents/vasospastic- angina?topicRef=89348&source=related_link 5. https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/s12872-018-0781-9 6. https://www.researchgate.net/publication/21361659_Histamine- induced_coronary_artery_spasm_The_concept_of_allergic_angina 7. Int J Cardiol. doi:10.1016/j.ijcard.2019.06.002 8. https://www.internationaljournalofcardiology.com/article/S0167-5273(05)01050-8 /abstract Acute coronary syndrome (ACS) is one of the common disease presentations encountered in medical practice. Allergic reaction to drugs is also a common occurrence and it manifests with wide range of symptoms and signs. However, an allergic reaction triggering ACS is a very rare occurrence and is described in literature as Kounis Syndrome (KS). This is the case report of one such occurrence where NSAID injection has caused ACS in an otherwise healthy person. Graph 1. Trend of cardiac enzyme levels Figure 2. ECG taken after 2 hours of arrival showing regression of ST-T changes Figure 3. CT Chest taken on Day 1 showing features of pulmonary edema – perihilar opacities Any ACS occurring in the setting of allergy is described as Kounis Syndrome (KS). Hence, CAG is not needed for diagnosis. It may be needed for therapy. Type1 – KS with no underlying CAD; can be treated with adrenaline, antihistamines, steroids, vasodilators and mast cell stabilizers. No anti-platelets indicated. Type2 – KS in patients with underlying CAD; can be treated with same drugs as Type 1 KS PLUS standard ACS protocol (i.e. anti-platelets indicated). Type3 – KS occurring as post procedure stent thrombosis; can be treated same as Type-2 PLUS aspiration of intrastent thrombus.