Brugada Syndrome - A Cardiac Channelopathy: Case Report

Case Report: Brugada Syndrome - A Cardiac Channelopathy. Poster used for presentation in CMC MAC 2021. OBJECTIVE: To discuss an interesting case of Brugada syndrome presenting as seizures. BACKGROUND: A 25-year-old well-informed male presented to us with complaints of seizure on day 3 of an acute febrile illness. He was conscious, oriented, GCS15/15 and system examinations were unremarkable. He had a similar history of seizure during fever 1 year back and was started on anti-epileptics since then and was treated with empirical antibiotics and CSF analysis, MRI brain with seizure protocol and EEG were completely normal during that episode. As described by patient, both episodes were very similar and was like darkening of visual field followed by LOC and bystanders witnessed few jerks involving both sides of body followed by regaining consciousness. This raised suspicion for syncope and ECG revealed RBBB-rSR’ pattern and saddleback STE in V1-V3(type2-brugada pattern-not diagnostic on its own). But on probing, patient revealed SCD in his father at age 42. RESULTS: Echo revealed structurally normal heart. Expert opinion sought and flecainide challenge test revealed the classical type1 brugada pattern (diagnostic) with coved STE and T inversion in V1-V3 clinching the diagnosis of BRUGADA SYNDROME. Genetic testing for channelopathy was unremarkable. Type 1 Brugada pattern (on provocative testing) along with syncopal event and family history strongly warranted AICD insertion and patient opted for subcutaneous ICD. 6 months later, ICD interrogation revealed occurrence of 1 episode of NSVT, which fell below the ICD intervention threshold. CONCLUSION: Brugada syndrome is a rare cardiac channelopathy with high risk of SCD in the absence of intervention. Events during fever and family history are very classical. It has male preponderance and more seen in Southeast Asia. All cases of suspected syncopal attacks warrant a thorough search for ECG markers of SCD.

Recommended
More Related Content
Similar to Brugada Syndrome - A Cardiac Channelopathy: Case Report
Similar to Brugada Syndrome - A Cardiac Channelopathy: Case Report (20)
More from Manievelraaman Kannan
More from Manievelraaman Kannan (11)
Recently uploaded
Recently uploaded (20)
Brugada Syndrome - A Cardiac Channelopathy: Case Report
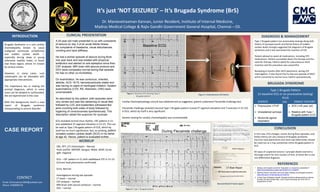
- 1. Dr. Manievelraaman Kannan, Junior Resident, Institute of Internal Medicine, Madras Medical College & Rajiv Gandhi Government General Hospital, Chennai – 03. CLINICAL PRESENTATION WORKUP CONCLUSION DIAGNOSIS & MANAGEMENT REFERENCES Figure 1. Baseline ECG showing Type 2 Brugada pattern Figure 2. Type 1 Brugada pattern INTRODUCTION CONTACT BRUGADA SYNDROME It’s just ‘NOT SEIZURES’ – It’s Brugada Syndrome (BrS) Email: drmvraaman1994@outlook.com Phone: 9789999778 Cardiac Electrophysiology consult was obtained and as suggested, patient underwent Flecainide challenge test. Flecainide challenge revealed classical Type 1 Brugada pattern (coved ST segment elevation and T inversion in V1-V2) in ECG, which by itself is very significant. Genetic testing for cardiac channelopathy was unremarkable Type 1 Brugada pattern (on provocative testing) along with history of syncopal events and family history of sudden cardiac death strongly suggested the diagnosis of Brugada syndrome and it also warranted the insertion of ICD. Patient advised to avoid all medications, including OTC medications. Patient counselled about the therapy and the need for therapy. Patient opted for subcutaneous AICD insertion and the procedure was uneventful. Reviewing 6 months after AICD placement, during ICD interrogation, it was found that he had one episode of NSVT which converted to normal sinus rhythm spontaneously. CBC, RFT, LFT, Electrolytes – Normal Fever profile: (MP/MF, Dengue, Widal, MSAT, Scrub IgM- negative ECG – rSR’ pattern in V1 with saddleback STE in V1-V2 (Correct lead placements confirmed) Echo: Normal Investigations during last episode: CT brain – normal CSF analysis – normal MRI brain with seizure protocol – normal EEG – normal In this case, ECG changes, events during fever episodes, and family history are very classical of Brugada syndrome. Incorrect lead placements and chest wall deformities should be ruled out as it may sometimes mimic Brugada pattern in ECG. All cases of suspected seizure / syncopal attacks warrant a thorough search for ECG markers of SCD, of which BrS is one rare differential diagnosis. A 25-year-old male presented to us with complaints of seizure on day 3 of an acute febrile illness. No complaints of headache, visual disturbances, vomiting and neck stiffness. He had a similar episode of seizure during fever one year back and was treated with empirical antibiotics and started on anti-epileptics since then. CSF analysis, MRI brain with seizure protocol and EEG were completely normal during that episode. He has no other co-morbidities. On examination, he was conscious, oriented, afebrile, GCS 15/15, hemodynamically stable and was having no signs of meningeal irritation. System examinations (CVS, RS, Abdomen, CNS) were unremarkable. As described by the patient, both episodes were very similar and was like darkening of visual field followed by LOC and bystanders witnessed few jerks involving both sides of body followed by regaining of consciousness spontaneously. This description raised the suspicion for syncope. ECG revealed normal sinus rhythm, rSR’ pattern in V1 and saddleback ST segment elevation in V1-V2. This can be read as Type 2 Brugada pattern of ECG, which by itself has no much significance. But, on probing, patient revealed sudden cardiac death (SCD) in his father at age 42. Hence, patient is evaluated further. 1. Epilepsy and brugada syndrome: Association or uncommon presentation? https://www.heartviews.org/text.asp?2020/21/2/114/288327 2. Electrical Storm in the Brain and in the Heart: Epilepsy and Brugada Syndrome https://doi.org/10.1016/j.mayocp.2013.06.019 3. A Fatal Case of Mistaken Identity: Brugada Syndrome Masquerading as Seizure Disorder (P2.264) Claribel Wee, Julius Latorre Neurology Apr 2018, 90 (15 Supplement) P2.264 Subcutaneous ICD device Brugada Syndrome is a rare cardiac channelopathy known to cause malignant ventricular arrhythmias and sudden cardiac death — especially during sleep in young otherwise healthy males, in South East Asian region, where it’s known by various names. However, in many cases, such catastrophe can be alleviated with appropriate interventions. The importance lies in making the prompt diagnosis, which in some cases can be delayed or confounded, like we experienced in this case. With this background, here’s a case report of Brugada syndrome masquerading as seizure disorder. Type 1 Brugada Pattern (in baseline ECG or on provocative testing) PLUS EVENTS (OR) FAMILY HISTORY Polymorphic VT/VF Unexplained syncope Nocturnal agonal respiration SCD (<45 year old) Relative with Type 1 Brugada pattern ECG Normal EEG & CT brain report Figure 3. Subcutaneous ICD device