1. Evaluating an access increasing intervention:
Cost-effectiveness of gas-insufflation-less laparoscopic surgery to increase access to minimally
invasive surgery for abdominal conditions in rural North-East India
Bryony Dawkins (1), Noel Aruparayil (2), Tim Ensor (1), Jesudian Gnanaraj (3), Julia Brown (4), David Jayne (2) and Bethany Shinkins (1)
1. Leeds Institute of Health Sciences, University of Leeds, UK ; 2. Leeds Institute of Medical Research, University of Leeds, UK; 3. Karunya Institute of Technology and Science,
Coimbatore, India; 4. Leeds Institute of Clinical Trials Research, University of Leeds, UK
• Gasless laparoscopy is likely to be a cost-effective alternative to
open surgery for abdominal conditions in rural North-East India
• Scale up of gasless laparoscopy as a means to increase access to
minimally invasive surgery for abdominal conditions would reduce
the cost burden to patients and increase the number of DALYs
averted
• As such it can provide a possible bridge to the adoption of full
laparoscopic services in resource limited settings
Conclusions
1. Chao TE, Mandigo M, Opoku-Anane J, Maine R. Systematic review of laparoscopic surgery in low-and middle-income countries: benefits, challenges, and
strategies. Surgical endoscopy. 2016;30(1):1-10.
2. Rosenbaum AJ, Maine RG. Improving access to laparoscopy in low-resource settings. Annals of global health. 2019;85(1).
3. Wilkinson E, Aruparayil N, Gnanaraj J, Mishra A, Bains L, Bolton W, et al. Barriers and facilitators of laparoscopic surgical training in rural north-east India: a
qualitative study. IJS Global Health. 2020;3(6):e29
4. Mishra A, Bains L, Jesudin G, Aruparayil N, Singh R. Evaluation of Gasless Laparoscopy as a Tool for Minimal Access Surgery in Low-to Middle-Income Countries: A
Phase II Noninferiority Randomized Controlled Study. Journal of the American College of Surgeons. 2020;231(5):511-9.
5. Icons made by Freepik and mavadee from www.flaticon.com
References
Methods
Evaluated cost-effectiveness of gasless laparoscopy to
increase access to minimally invasive surgery for abdominal
conditions in rural North-East India using decision tree model
Costs evaluated from patient perspective including direct &
indirect costs
Outcomes in terms of disability-adjusted life years (DALYs)
averted modelled based on patient severity and duration of
symptoms obtained by expert elicitation
Scale up analysis modelled impact on costs and outcomes as
provision of gasless laparoscopy increases based on data
from 12 facilities in rural North-East India
Following a training programme in gasless laparoscopic surgery and
using data from a subsequent registry of abdominal operations in
rural India, a facility survey and the wider literature, we:
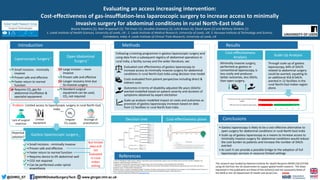
Cost-effectiveness plane
-2500
-2000
-1500
-1000
-500
0
500
1000
1500
2000
2500
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35
Incremental
Cost
(USD)
DALYs Averted
ICER
Point estimate
Cost-effectiveness threshold=342USD/DALY averted (17% GDP per capita)
Cost-effectiveness threshold=462USD/DALY averted (23% GDP per capita)
Cost-effectiveness threshold=2010USD/DALY averted (GDP per capita)
Cost-effectiveness threshold=6030USD/DALY averted (3x GDP per capita)
Decision tree
Laparoscopic Surgery
• Small incisions - minimally
invasive
• Proven safe and effective
• Faster return to normal
function
• Requires CO2 gas for
abdominal insufflation &
specialist equipment
Open Abdominal
Surgery
• Large incision – more
invasive
• Proven safe and effective
• Longer recovery time due
to invasive surgery
• Standard surgical
equipment can be used,
CO2 not required
Gasless laparoscopic surgery
• Small incisions - minimally invasive
• Proven safe and effective
• Faster return to normal function
• Requires device to lift abdominal wall
• CO2 not required
• Can be performed under spinal
anaesthesia
Potential
solution?
Limited
equipment
Problem: Limited access to laparoscopic surgery in rural North-East
India
Lack of surgical
expertise
CO2
Irregular
CO2 supply
Shortage of
anaesthetists
Introduction
But limited
data and
not
evaluated
in rural
Indian
setting
3,4,5
1,2
3,4
1,2
@GHRG_ST @NIHRGlobalSurgeryTech www.ghrgst.nhir.ac.uk
This research was funded by National Institute for Health Research (NIHR) (16/137/44)
using UK Aid from the UK Government to support global health research. The views
expressed in this publication are those of the author(s) and not necessarily those of
the NIHR or the UK Department of Health and Social Care.
Results
Cost-effectiveness
Analysis
Minimally invasive surgery,
performed as gasless or
conventional laparoscopy, is
less costly and produces
better outcomes, less DALYs,
than open surgery.
Scale Up Analysis
Through scale up of gasless
laparoscopy, 64% of DALYS
related to abdominal surgery
could be averted, equating to
an additional 454.8 DALYs
averted in 12 facilities in the
rural North-East Indian region
alone.
Died
Post-operative complications
Discharged
Convert to open
Died
No post-operative complications Discharged
Gasless
Died
Post-operative complications
Discharged
No conversion Died
Minimally
Invasive Surgery No post-operative complications Discharged
Died
Post-operative complications
Discharged
Convert to open
Died
No post-operative complications Discharged
Laparoscopy Died
Patient needing Post-operative complications
abdominal surgery Discharged
No conversion Died
No post-operative complications Discharged
Died
Post-operative complications
Discharged
Open
Died
No post-operative complications Discharged