In nursing practice, accurate identification and application of research is essential to achieving successful outcomes. The ability to articulate research data and summarize relevant content supports the student's ability to further develop and synthesize the assignments that constitute the components of the capstone project.
The assignment will be used to develop a written implementation plan.
For this assignment, provide a synopsis of the review of the research literature. Using the "Literature Evaluation Table," determine the level and strength of the evidence for each of the eight research articles you have selected. The articles should be current (within the last 5 years) and closely relate to the PICOT question developed earlier in this course. The articles may include quantitative research, descriptive analyses, longitudinal studies, or meta-analysis articles. A systematic review may be used to provide background information for the purpose or problem identified in the proposed capstone project.
While APA style is not required for the body of this assignment, solid academic writing is expected, and in-text citations and references should be presented using APA documentation guidelines, which can be found in the APA Style Guide, located in the Student Success Center.
This assignment uses a rubric. Please review the rubric prior to beginning the assignment to become familiar with the expectations for successful completion.
NOTE;
CAPSTONE TOPIC. PREVENTION OF FALLS IN THE ELDERLY IN HEALTHCARE FACILITY
the PIOCT statement (Remember to spell out your P-population of your focus; I- what is your intervention; C- compared to the current process/ old process; O- measurable outcome such as 10% at the minimum; T- it usually takes time for your Intervention to change the outcomes- data to be collected for 6 months to measure the outcomes of your project).
The project must be within the nursing scope of practice and focus on a single realistic project strategy. The supportive references must be (8) peer-reviewed articles and not from the following; .com, .org, CDC, or WHO, and product publications which can be used as supportive documents in addition to your peer-reviewed articles.
ORIGINAL RESEARCH
Objective: Analysis of risk factors for falls through a detailed geriatric evaluation is essential. The aim of the present study was to analyze prognostic
factors for falls in elderly patients in Spain.
Materials and Methods: a) Initial phase (n=247): transverse observational study. Inclusion criteria: patients >80 years old living alone and/or with a
relative of similar age; b) Final phase (n=90): prospective cohort study of the previously enrolled patients. Variables analyzed included demographics;
clinical characteristics and results of timed up and go (TUG) (mobility assessment) and Lobo (cognitive assessment) tests; Lawton-Brody Instrumental
Activities of Daily Living scale and Barthel index (basic activities).
Results: Falls ...
Basic Civil Engineering first year Notes- Chapter 4 Building.pptx
In nursing practice, accurate identification and application of re
1. In nursing practice, accurate identification and application of
research is essential to achieving successful outcomes. The
ability to articulate research data and summarize relevant
content supports the student's ability to further develop and
synthesize the assignments that constitute the components of the
capstone project.
The assignment will be used to develop a written
implementation plan.
For this assignment, provide a synopsis of the review of the
research literature. Using the "Literature Evaluation Table,"
determine the level and strength of the evidence for each of the
eight research articles you have selected. The articles should be
current (within the last 5 years) and closely relate to the PICOT
question developed earlier in this course. The articles may
include quantitative research, descriptive analyses, longitudinal
studies, or meta-analysis articles. A systematic review may be
used to provide background information for the purpose or
problem identified in the proposed capstone project.
While APA style is not required for the body of this assignment,
solid academic writing is expected, and in-text citations and
references should be presented using APA documentation
guidelines, which can be found in the APA Style Guide, located
in the Student Success Center.
This assignment uses a rubric. Please review the rubric prior to
beginning the assignment to become familiar with the
expectations for successful completion.
NOTE;
CAPSTONE TOPIC. PREVENTION OF FALLS IN THE
ELDERLY IN HEALTHCARE FACILITY
the PIOCT statement (Remember to spell out your P-population
of your focus; I- what is your intervention; C- compared to the
2. current process/ old process; O- measurable outcome such as
10% at the minimum; T- it usually takes time for your
Intervention to change the outcomes- data to be collected for 6
months to measure the outcomes of your project).
The project must be within the nursing scope of practice and
focus on a single realistic project strategy. The supportive
references must be (8) peer-reviewed articles and not from the
following; .com, .org, CDC, or WHO, and product publications
which can be used as supportive documents in addition to your
peer-reviewed articles.
ORIGINAL RESEARCH
Objective: Analysis of risk factors for falls through a detailed
geriatric evaluation is essential. The aim of the present study
was to analyze prognostic
factors for falls in elderly patients in Spain.
Materials and Methods: a) Initial phase (n=247): transverse
observational study. Inclusion criteria: patients >80 years old
living alone and/or with a
relative of similar age; b) Final phase (n=90): prospective
cohort study of the previously enrolled patients. Variables
analyzed included demographics;
clinical characteristics and results of timed up and go (TUG)
(mobility assessment) and Lobo (cognitive assessment) tests;
Lawton-Brody Instrumental
Activities of Daily Living scale and Barthel index (basic
activities).
3. Results: Falls were significantly associated with changes in
Lobo and Barthel test results during both phases. No association
was found between falls
and comorbidities, number or type of treatment received and
analytical variables studied. No statistical difference was
observed in TUG test between
fallers and non-fallers in the initial phase. A significant
deterioration was observed in Lobo, Lawton-Brody, Barthel and
TUG evaluation tests during
the 4-year in between-period; male gender and a lower score in
Lobo test were independent variables related to mortality. In the
final phase, a TUG
cut-off value of 25 seconds (sensitivity=0.52; specificity=0.75),
that differentiated fallers from non-fallers, was established.
Conclusion: Tests that evaluate cognitive ability and functional
activities are predictors of falls in the elderly. The use of Lobo
test to define the
cognitive state of elderly patients may contribute to predict
their vital prognoses.
Keywords: Elderly, fall, risk of fall, time get up and go test,
Lobo test, Lawton-Brody test, Barthel test
Functional Evaluation Tests as Prognostic Factors of Falls in
Elderly Patients
DOI: 10.4274/ejgg.galenos.2019.114
Eur J Geriatr Gerontol 2019;1(3):78-86
Javier Benítez1, Juan Manuel Ignacio1, Sofía Perea3, José
Antonio Girón2
1La Laguna Health Center, Department of Internal Medicine,
Cádiz, Spain
4. 2Puerta del Mar University Hospital, Clinic of Internal
Medicine, Cádiz, Spain
3Beth Israel Deaconess Medical Center, Department of
Medicine, Boston/MA, USA
Abstract
Introduction
Falls in elderly patients are a daily concern that occurs in
almost half of them, with a wide range of consequences and
whose importance is not recognized neither by themselves, nor
their relatives, nor health professionals (1,2). They are seldom
accidental, but rather the result of an inadequacy betw een the
senior and his/her surroundings; hence the unawareness of the
risk factors associated with the falls contributes to an increase
in their incidence (3).
Extrinsic (environmental) as well as intrinsic (clinical factors)
risk factors associated with falls have been previously described
(4,5). The incidence of falls increases progressively with age,
reaching 50% in individuals >80 years (6,7). A study conducted
by our group established that the incidence of falls in
individuals
>80 years per number of patients/year ranged between 11.9%
and 17.8%, with a mean value of 14.0% (6,8,9).
The analysis of the risk factors associated with falls
through a geriatric assessment is a key element for their
adequate management. Such assessment should include a
multidimensional analysis (10,11): a) circumstances of the fall;
b) comprehensive geriatric valuation: b1. biological evaluation
(acute or chronic processes, as well as drug consumption,
nutritional status, presence of other geriatric syndromes); b2.
functional evaluation (Barthel and Lawton-Brody tests) (11,12);
b3. Mental and psycho-affective evaluations (minimental state
6. assessment; g) specific complementary examinations: blood
count, glycemia, ions, thyroid hormones, vitamin D, EKG,
among
others.
With regards to the assessment of balance and gait, although
the Tinetti test was initially validated to predict the risk of
falls,
however, in daily clinical practice the test timed up and go
(TUG)
is currently used (14). This test presents a high correlation with
the speed of the march, it is much easier to carry out, requires
less time and has a strong correlation with Tinetti test (15,16).
In 2009 the “Comprehensive Plan for elderly individuals ≥80
years of age who live alone and/or with a relative with a similar
age” was implemented in our center. The results of a
preliminary
study showed that: a) the most common locations of falls are
corridor, bathroom, living room, bedroom and elevators; b) the
risk of falls increases with the degree of dependence; c) The
degree of dependence correlates with the results of the TUG
test.
Based on those results, the present study was designed to
analyze the frequency and factors involved (including the TUG,
Lobo, Lawton-Brody and Barthel tests) in the risk of falls in
elderly patients living alone and/or with a relative of similar
age
in the province of Cádiz, Spain.
Materials and Methods
Study Design
The study was conducted in Unidad de Gestión Clínica “La
7. Laguna”, Cadiz, Spain and was approved by the relevant health
authorities and ethic committees. The study consisted of an
initial phase (2013) and a final phase (2017): a) Initial phase:
transverse observational study. Inclusion criteria: Patients >80
years living alone and/or with a relative of similar age. Those in
whom the TUG test could not be carried out due to neurological
alterations, trauma or rheumatic diseases were excluded from
the final phase of the study; b) Final phase: prospective cohort
study of the patients enrolled in 2013, followed until 2017. The
electronic medical records were reviewed and once the cases
were selected, patients were visited in their homes, and after
obtaining the informed consent, collection of variables and
performance of tests described below were performed.
Study Outcomes
1. Primary outcome: To analyze factors (Lobo, Lawton-Brody,
Barthel and TUG tests) involved in the development of falls in
patients >80 years old years living alone and/or with a relative
of similar age. Tests were conducted by primary care
physicians.
In particular, the following specific outcomes were studied:
a) Analysis of the frequency of falls
b) Establishment of the intrinsic risk factors associated with a
higher frequency of falls.
c) Establishment of the predictive value of TUG test in the
appearance of falls.
d) Association between cognitive level (Lobo test) and risk of
falls.
e) Association between falls and the outcome regarding
8. cognitive assessment (Lobo test), instrumental (Lawton-Brody
tests) and basic (Barthel test) daily activities.
2. Secondary outcomes: Correlation between the levels of
vitamin D and frequency of falls among elderly patients and
predictive value of death of Lobo, Lawton-Brody, Barthel and
TUG tests.
Variables Analyzed
1. Dependent variables: Number of falls; number of deaths.
2. Independent variables: a) demographic (gender, age);
b) Clinical characteristics: b.1) comorbidities: cardiological;
neurological; respiratory; musculoskeletal system); metabolic/
endocrine diseases; b.2) biochemistry values: hemoglobin;
glycemia; glycated hemoglobin (HbA1c)(%); iron; ferritin;
transferrin; vitamin B12; folic acid; total proteins; albumin;
thyroid stimulating hormone (TSH); cholesterol; triglycerides;
uric acid; creatinine; vitamin D (this latter only during final
phase); c) functional evaluation tests: Lobo, TUG, Barthel and
Lawton-Brody tests; d) drug treatments associated with a
greater risk of falls (only during final phase).
Instruments
1. TUG Test: Validated test in which the patient is time while
they rise from a chair, walk 3 m, turn around, return to the
chair,
and sit down again. A faster time indicates a better functional
performance. Reported threshold values vary from 10 to 33
seconds (17).
2. Lobo Test (Mini Examen Cognoscitivo): It is the Spanish
validation/adaptation of the Folstein minimental state
examination (MMSE), and consists of 35 items, and each
9. correct answer is scored as 1 point. It evaluates six cognitive
abilities (orientation, registration, attention and concentration,
short-term memory and language), and takes 5-10 minutes to
administer. The cutting point of advanced cognitive impairment
stands at 24/35 points. The test has a sensitivity for diagnosis of
90.7% and a specificity of 69% (18).
3. Lawton-Brody Test: It is a validated instrument to assess
independent living skills. There are eight domains of function
measured with the Lawton IADL scale. A summary score
80
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly Patients Eur J Geriatr Gerontol 2019;1(3):78-
86
ranges from 0 (low function, dependent) to 8 (high function,
independent) for women, and 0 through 5 for men (19).
4. Barthel Index: The Barthel index is a validated test that
encompasses 10 items on motor tasks rated on a weighted
ordinal
scale with lower scores indicating more need for assistance to
complete each activity. The maximum score is 100 points (90 if
the patient is travelling in a wheelchair). The cutoff points are:
a) 81-100, self-employed; b) 61-80, mild dependence; c) 46-69,
moderate dependence, and d) <45, severe dependence (20,21).
Statistics
For quantitative variables that follow a normal distribution
(analyzed by Kolmogorov-Smirnov test), mean and the
standard deviation were used; otherwise, median and
10. interquartile range. Qualitative variables were expressed
by number and percentage. Student’s t-test was used for
comparison of two means in case of parametric quantitative
variables and with homogeneous variances, otherwise, Mann-
Whitney U test was used. Qualitative variables were compared
using the chi-square test, with Fisher correction whenever
needed. The ROC curve of the TUG test, its positive and
negative
predictive values, as well as the establishment of a cut-off to
determine the risk of falls was determined during the final
phase. For the evaluation of the independent association of
risk factors for falls and mortality, a logistic regression test
was carried out, introducing in the model those factors that
had reached statistical significance in the bivariate analysis.
For data analysis, SPSS statistical package, version 20.0 (SPSS
Inc. Chicago, IL, USA) was used. A level of significance of
95%
(p<0.05) was considered.
Results
Initial Phase
During the years 2013-2017, a total of 342 that patients
fulfilled all the inclusion criteria, from a pool population
of 984 patients, were selected. Of those, 247 signed the
informed consent and were enrolled in the initial phase
of the study. The demographic and clinical characteristics
as well as the frequency of falls are summarized in Table
1. The most common comorbidities were hypertension
and rheumatic diseases, followed by diabetes mellitus and
were not significantly associated with a higher risk of falls
(p>0.005). With regards to functional evaluation tests, the
profile of the elderly patient in this initial phase showed
an acceptable cognitive level, with autonomy for the basic
and instrumental daily life activities. Statistical significant
11. differences were observed between those who have reported
falls vs those who have not, with regards to cognitive level
(Lobo test) and daily basic activities (Barthel test). As of
TUG score, no significant difference was observed between
Table 1. Initial and final phases: demographic and clinical
characteristics
Demographics Baseline phase
(n=247)
Final phase
(n=90)
Gender (n, %M/F) 247 (30.8%/69.2%) 90 (17.7%/82.3%)
Age, mean (range),
in years
89.2±3.6 (80-101) 88.9±2.6 (83-96)
Age ranges: n (%)
80-84 152 (61.5%) 4 (4.4%)
85-89 75 (30.4%) 57 (63.3%)
≥90 20 (8.1%) 29 (32.2%)
Falls (n, %)
No 65 (26.3%) 67 (74.4%)
Yes 182 (73.7%) 23 (25.5%)
Comorbidities (n, %)
13. Iron (μg/dL) 69.1±26.5 75.6±28.3
Ferritin (ng/dL) 81.3±65.7 79.4±63.6
Transferrin (mg/dL) 274.1±55.5 276.9±49.4
Vitamin B12 (pg/dL) 427.2±277.9 435.7±282.2
Folic acid (ng/mL) 12.1±12.4 12.1±12.3
Total proteins (g/dL) 6.9±0.6 7.1±0.6
Albumin (g/dL) 4.5±3.9 5.3±3.1
TSH (ng/dL) 3.1±2.1 3.1±2.2
Cholesterol (mg/dL) 202.2±40.8 208.9±47.5
Triglycerides (mg/dL) 124.2±71.3 122.7±57.3
Uric acid (mg/dL) 5.2±1.6 5.1±1.2
Creatinine (mg/dL) 1.1±0.6 0.9±0.4
SD: Standard deviation; TSH: Thyroid stimulating hormone,
HbA1c : Hemoglobin A1c,
M: Male, F: Female, n: Number of the patients
*Others: Other diseases with a prevalence <0.4%
8181
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly PatientsEur J Geriatr Gerontol 2019;1(3):78-
14. 86
Table 2. Functional evaluation tests (falls vs no falls) and
bivariate analysis
Baseline phase: functional evaluation tests
Tests Total (n=247) Falls (n=182) No falls (n=65) p value
Lobo test, mean ± SD, points 27.2±9.3 27.7±8.6 25.1±11.5
0.012
Barthel test, mean ± SD, points 80.8±29.3 83.7±26.8 72.3±34.3
0.008
Lawton-Brody, mean ± SD, points 5.8±2.6 5.9±2.6 5.4±2.6
0.279
TUG test, mean ± SD, seconds 15.2±8.6 15.4±9.1 14.0±5.2
0.457
Bivariate analyses
Variables Falls (n=182) No falls (n=65) p value
Age, mean ± SD, years 88.9±3.4 89.9±4.3 0.069
Gender, Male (n, %) 54 (29.7%) 22 (33.8%) 0.535
Comorbidities
Hypertension (n, %) 95 (52.2%) 33 (50.8%) 0.886
Diabetes mellitus (n, %) 36 (19.8%) 15 (23.1%) 0.594
Rheumatological diseases (n, %) 50 (27.5%) 11 (16.9%) 0.097
Cognitive impairment (n, %) 18 (9.9%) 5 (7.7%) 0.804
Functional evaluation tests
Lobo test (points) 27.7±8.6 25.1±11.5 0.012
Lawton-Brody tests (points) 5.9±2.6 5.4±2.6 0.279
Barthel test (points) 83.7±26.8 72.3±34.3 0.008
TUG (seconds) 15.4±9.1 14.0±9.2 0.457
15. Hemoglobin (g/dL) 13.2±1.6 12.7±1.5 0.029
Final phase: functional evaluation tests
Tests Total (n=90) Falls (n=23) No falls (n=67) p value
Lobo test, mean ± SD, points
Initial
Final
30.8±4.3
24.9±7.4
30.8±4.0
21.6±8.7
30.7±4.5
25.9±6.6
0.243
0.016
Barthel test, mean ± SD, points
Initial
Final
92.8±13.8
77.7±27.9
92.0±14.5
63.9±33.1
93.1±13.6
81.4±22.6
0.967
0.006
16. Lawton-Brody test, mean ± SD, points
Initial
Final
6.7±1.9
5.0±2.8
7.1±1.5
4.5±3.1
6.6±2.0
5.1±2.5
0.184
0.318
TUG test, mean ± SD, seconds
Initial
Final
14.4±6.9
24.3±10.2
14.9±7.8
27.0±12.0
14.3±6.8
23.5±9.3
0.912
0.154
Bivariate analyses
Variables Falls (n=23) No falls (n=67) p value
Age, mean ± SD, years 88.7±2.6 88.1±2.7 0.320
17. Gender, Male (n, %) 6 (26.1%) 10 (14.9%) 0.342
Comorbidities
Hypertension (n, %) 10 (23.8%) 32 (76.2%) 0.811
Diabetes mellitus (n, %) 6 (33.3%) 12 (66.7%) 0.384
Rheumatological diseases (n, %) 7 (28.0%) 18 (72%) 0.790
Functional evaluation tests Falls (n=23) No falls (n=67) p value
Lobo test 21.6±8.7 25.9±6.6 0.016
Barthel test 63.9±33.1 81.4±22.6 0.006
Lawton-Brody test 4.5±3.1 5.1±2.5 0.318
TUG test 27.0±12.0 23.5±9.3 0.154
Hemoglobin (g/dL) 13.5±1.4 13.1±1.6 0.387
*SD: Standard deviation, TUG: Timed up and go test
82
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly Patients Eur J Geriatr Gerontol 2019;1(3):78-
86
the mean value of the fallers vs non-fallers (Table 2). A
significant positive correlation between age and TUG was
detected, whereas a negative correlation was found between
age and Lobo, Lawton-Brody and Barthel tests, respectively
(Table 3). Lobo, Lawton-Brody and Barthel tests correlated
significantly with each other and negatively with TUG.
Previous falls was significantly associated with a higher
score in Lobo and Barthel tests as well as with a signi ficantly
18. higher concentration of hemoglobin (Table 2).
In Between Phase
Between the two phases, 108 individuals (43.7% of the 247
subjects who participated in the initial phase) died; 24 (9.7%)
changed residence, 17 (6.8%) were admitted in nursing homes
and eight (3.2%) withdrew informed consent. Among the
deceased, no primary or secondary-related disease associated
with falls was detected. The causes of the deaths included:
cardiovascular disease (n=32, 30.2%); cancer (n=25, 23.3%);
cognitive disorder (n=17 individuals, 15.1%); cerebrovascular
disease (n=13, 11.8%); respiratory disease (n=9, 7.7%);
gastrointestinal disease (n=8, 7.3%); diabetes mellitus (n=3,
7.3%) and renal disease (n=1, 2.1%). The deceased were
slightly
older than the survivors; the proportion of males was higher;
Lobo, Lawton-Brody and Barthel tests’ scores were lower and
had lower cholesterol concentrations. No significant differences
were observed regarding the presence of previous falls or the
Table 3. Correlation between age (initial phase), vitamin D
concentration (final phase) and functional evaluation tests
Initial phase Age Lobo test Barthel test Lawton test TUG test
Age R value
p value
1
-
-0.190
0.008
-0.207
20. -
0.768
0.000
-0.576
0.000
Lawton test R value
p value
-0.282
0.000
0.662
0.000
0.768
0.000
1
-
-0.560
0.000
TUG test R value
p value
0.306
0.000
-0.453
0.000
-0.576
21. 0.000
-0.560
0.000
1
-
Final phase TUG test Lobo test Barthel test Lawton test Vitamin
D
TUG test R value
p value
1
-
-0.474
0.000
-0.758
0.000
-0.758
0.000
-0.259
0.014
Lobo test R value
p value
-0.474
0.000
1
23. 0.000
0.768
0.000
1
-
0.245
0.020
Vitamin D R value
p value
-0.259
0.014
0.262
0.013
0.281
0.007
0.245
0.020
1
-
TUG: Timed up and go test
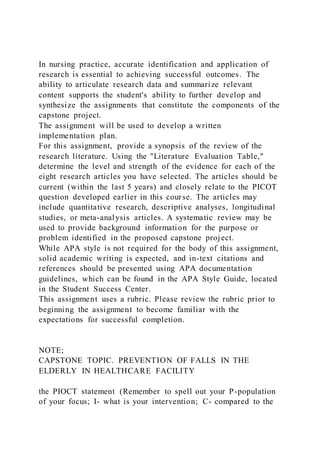
Figure 1. TUG test: ROC curve
TUG: Timed and go test, ROC: Receiver operating
characteristic
24. 8383
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly PatientsEur J Geriatr Gerontol 2019;1(3):78-
86
time in seconds spent in completing the TUG test between the
two groups. In the multivariate analysis, the factors that were
independently associated with mortality were male gender
(p=0.016) and Lobo test score (p=0.002), respectively (data not
shown).
Final Phase
A total of 90 patients were enrolled in the final phase (Table 1).
When compared to the initial phase, no statistically significant
differences were observed with regards to demographic and
biochemistry values. In addition, no significant differences
were observed with regards to biochemistry values between
fallers and non-fallers during the final phase. With regards to
comorbidities, hypertension, diabetes and rheumatological
diseases were the most prevalent. The presence of falls was
not significantly higher in individuals who presented some of
the most frequent comorbidities (data not shown).
With regards to functional evaluation tests, there was a
significantly lower score on Lobo and Barthel tests among
fallers vs non-fallers (Table 2). As for TUG test, when
individuals
were grouped according to the time required to conduct the
test, and using the cut-off point of 25 seconds, it was observed
that the frequency of falls was significantly higher in those that
required longer time to conduct the test (p=0.039). The TUG
cut-off value of 25 seconds had a sensitivity of 0.522 and a
25. specificity of 0.746, respectively (Figure 1).
With regards to drug treatments, the mean number of drugs
used was 6±4 (range=0-19). No statistically significant
differences were observed between fallers and non-fallers as to
type or number of treatments received (falls: mean treatments:
7.2±3.6 vs no falls: 5.8±3.4, p=0.109).
Functional Evaluation Tests and Vitamin D
Forty-seven (52.2%) individuals had low level vitamin D
concentrations (˂20 ng/dL) during the final phase. A positive
significant correlation between the serum concentration of
vitamin D and the scores obtained in the Lobo, Lawton-Brody
and Barthel tests and a negative correlation with the time
in seconds required to complete the TUG test was observed
(Table 3).
Initial Vs Final Phase
Falls
Only 14 individuals (15.5%) did not refer any fall during any of
the two phases of the study. A total of 53 (79.1%) individuals
that experienced falls during the baseline phase of the study did
not experience any fall during the final phase of the study. Only
five individuals (21.1%) reported falls during both study
phases.
The factors associated with the absence of recurrence of falls in
those who had previously presented them compared to those
who had a fall recurrence were analyzed. For that, the following
variables were compared: age, gender, comorbidities, functional
evaluation tests’ scores and biochemistry determinations. No
statistically significant differences were observed between the
two groups with regards to any of the above parameters (data
not shown).
26. Functional Evaluation Tests
The mean values for the initial phase and final phase tests are
shown in Table 4, detailing the data globally as well as in the
two groups (individuals with and without falls in this final
phase). The differences observed in each of the groups (with
or without falls), except for TUG, were statistical significant.
Both in the global group and in the two subgroups of
individuals, during the four years between assessments,
a significant deterioration occurred in each of the tests
analyzed (Table 2).
Multivariate Analysis of Risk Factors for Falls
The only variable significantly associated with a risk of falls
was
Barthel test score (p=0.006).
Discussion
The present study analyzed the prognostic factors of falls in
seniors. The population studied was older and included more
women compared to previous studies (22,23). The frequency
of falls was higher during the initial phase compared to the
final phase. In addition, the frequency of falls observed during
the final phase was significantly inferior to that reported by
Rodriguez Molinero et al. (6) in a previous study conducted in
Spain (50%). It could be assumed that the subjects participating
Table 4. Initial vs final phase: differences in the scores of Lobo,
Lawton-Brody, Barthel and TUG tests related to the presence or
absence of falls
Differences between initial and
final scores
Global (n=90) No falls (n=67) Falls (n=23) p value
27. (no falls vs falls)Mean ± SD Mean ± SD Mean ± SD
Lobo test -6.0±6.7 -4.9±5.7 -9.2±8.2 0.007
Barthel test -15.8±23.4 -11.6±18.5 -28.0±31.2 0.003
Lawton test -1.8±2.2 -1.4±2.1 -2.7±2.5 0.018
TUG test 9.9±8.8 9.2±8.4 12.1±9.6 0.208
TUG: Timed up and go test, SD: Standard deviation
84
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly Patients Eur J Geriatr Gerontol 2019;1(3):78-
86
in the final phase represent a subgroup of individuals with
better functional status or they protected themselves better
after having experienced prior falls.
Baseline comorbidities included hypertensio n, diabetes mellitus
and rheumatic diseases. However, unlike in other studies, their
presence was not associated with an increased risk of falls in
any
of the two phases studied, nor there was a significant increase
in the risk of falls associated with the use of drug treatments
that favor their appearance (4,24,25). The analytical profile of
the participants was within normal range. Different alterations
may have been associated with falls; however, no meaningful
association was found. In addition, low vitamin D concentration
was not associated with a higher risk of falls, although more
than 50% of the participants showed a vitamin D deficit. The
efficacy of vitamin D supplements to reduce risk of falls in
28. individuals with low vitamin D levels has been previously
shown
(26). It is possible, as Bromfield et al. (27) argues, that it is not
the underlying diseases or the treatment itself but the existence
of a fragility criterion.
In the initial phase of the study, the parameters that were
significantly associated with the presence of falls were a
higher concentration of hemoglobin and a higher score in Lobo
and Barthel tests. These findings are seemingly paradoxical.
It could be justified given that those patients who have a
cognitive deterioration or less capacity for the basic activities
of the daily life or a certain degree of anemia move less, and
therefore require greater care, thus reducing therefore the risk
of fall. One aspect to emphasize is the analysis of the evolution
during the in between phases period. While no significant
analytical modifications were observed, however, a significant
deterioration of the cognitive, functional and TUG tests was
detected. This scenario has been previously described by
several authors, who explain the worsening of the functional
evaluation tests with the ‘‘limited time mechanism’’ theory, that
is, the decrease in the speed with which cognitive processing
operations can be executed influences the functionality or
autonomy for the basic and instrumental activities of daily life
(28-30).
Finally, the different parameters, including the presence of
falls, present in the initial phase on the mortality occurring
between the two periods were analyzed. Mortality during
the four years between the two phases was 43.7%, being the
causes of the death expected in this age group (cardio-or
brain-vascular disease, neoplasms and dementias). The factors
associated with greater mortality were male gender and a
lower score in the Lobo test, confirming the results of previous
studies (31-34). In the present study the causes of death were
mainly vascular diseases and neoplasms, and therefore, there is
29. no clear explanation that justifies the relationship previously
mentioned.
The results in the final phase of the study showed a
significantly
higher incidence of falls associated with a lower score of the
Lobo and Barthel tests, as well as with the differences in
the scores in Lobo, Barthel and Lawton-Brody tests reported
between the initial and final phases. It can therefore be
concluded that in real life the cognitive and functional tests are
the ones associated with the risk of falls in senior population
and not so much the comorbidities, treatments received or
analytical alterations. Several studies confirm that cognitive
impairment, associated with an altered result in the Lobo
test, and functional dependency, measured by the Barthel
and Lawton-Brody tests, are key predisposing factors for the
emergence of falls (35,36).
One of the specific aims of the present study was to establish
a cut off value of TUG that would identify the population with
a greater risk of fall. In the initial phase of the study, the time
to perform the TUG test did not differentiate those individuals
who fell from those who did not. Only in the final phase a
TUG cut off value of 25 seconds, that differentiated those
who fell from those who did not, was established. The cut off
value ranged from 12 to 16 seconds in prior studies (37,38).
The results of the TUG test showed a negative correlation with
Lobo, Barthel and Lawton-Brody tests. While the correlation
with the latter two was as expected (lower speed in exercise,
less capacity for instrumental and even basic activities of
daily life), the relationship with Lobo test was less obvious.
However, there are studies in the literature that analyzed the
relationship between these parameters and have shown that,
at least partially, alterations in cognitive tests are correlated
with alterations in the speed or variability of gait (39,40).
30. Study Limitations
There are some limitations that should be mentioned. First,
the number of patients that participated in the final phase is
small (90 patients), that is, 36% of the initial sample, but it is
also important to highlight that, none of the deaths during
the in-between period (108 patients, 48%), were due to
complications related to a fall. Second, the results might have
been affected by recall bias (fall history was obtained using
a questionnaire) as well as selection bias (participants may
have had a stronger interest in learning about their risk of fall
compared to their peers who did not choose to participate). In
addition, all subjects were recruited from a single independent
living community in the Southern region of Spain, so it may be
difficult to generalize our results to older adults with different
characteristics or from other countries.
Conclusion
It can be concluded that the predictive factors of falls in
individuals >80 years of age are mainly those that evaluate
cognitive ability and functional activities. Moreover, the
8585
Benítez et al. Functional Evaluation Tests as Prognostic Factors
of Falls in Elderly PatientsEur J Geriatr Gerontol 2019;1(3):78-
86
evaluation of the cognitive status by a simple test like the Lobo
test contributes to evaluate their vital prognoses.
Ethics
Ethics Committee Approval: The study was conducted in
32. 3. Lázaro del Nogal, M. Inestabilidad y Caídas en “Geriatría en
Atención
Primaria” Ribera Casado JM, et al eds. Ed. Biblioteca Aula
Médica, 4ª edición,
Madrid 2008; pp. 243-254.
4. Mesa Lampré MP. Factores de riesgo de caídas en Evaluación
del anciano
con caídas, Documento del Grupo de Trabajo de Caídas de la
Sociedad
Española de Geriatría y Gerontología. Madrid 2011;pp. 17-36.
5. Marañón Fernández E, Mesas Sotos R, en Guillen Llera, F.
Síndromes y
cuidados en el paciente geriátrico. Elsevier, 2ª edición, Madrid
2008;
pp.497-512.
6. Rodriguez Molinero A, Narvaiza L, Gálvez-Barrón C, de la
Cruz JJ, Ruiz J,
Gonzalo N, Valldosera E, Yuste A. Caídas en la población
anciana española:
incidencia, consecuencias y factores de riesgo. Rev. Esp Geriatr
Gerontol
2015;50:274-280.
7. Ribera Casado JM. Caídas y edad avanzada, ¿un problema
médico? Med Clin
2004; 122:180-181.
8. Benitez J, Bellanco P. Avances en el estudio de las caídas en
mayores.
Análisis del punto de corte de Timed get Up and Go. Eur J
Health Research
2015;1:15-25.
33. 9. Duaso E, Casas A, Formiga F, Lázaro Del Nogal M, Salvà A,
Marcellán T,
Navarro C. Unidades de prevención de caídas y fracturas
osteoporóticas.
Propuesta del Grupo de Osteoporosis, Caídas y Fracturas de la
Sociedad
Española de Geriatría y Gerontología. Rev Esp Geriatr Gerontol
2011;46:268-
274.
10. AGS/BGS clinical practice guideline: prevention of falls in
older persons.
In:
www.alabmed.com/uploadfile/2014/0504/20140504033204923.p
df,
accessed Feb 20,2019
11. Flores Ruano T, Cruz Jentoft A, González Montalvo JI,
López Soto A, Abizanda
Soler. Herramientas de valoración geriátrica en servicios de
Geriatría. Rev
Esp Geriatr Gerontol 2014;49:235-242.
12. Cid-Ruzafa J, Damián-Moreno J. Valoración de la
discapacidad física: el
índice de Barthel. Rev Esp Salud Pública 1997;71:127-137.
13. Díaz Pelegrina A, Cabrera-Martos I, López-Torres I,
Rodríguez-Torres
J, Valenza MC. Efectos del estado cognitivo sobre las
alteraciones del
equilibrio y la marcha en ancianos institucionalizados. Rev Esp
Geriatr
Gerontol 2016;51:88-91.
14. Podsiadlo D, Richardson S. The “Up & Go” timed: a basic
34. functional mobility
test for frail elderly people. J Am Geriatr Soc 1991;39:142-148.
15. Tinetti ME, Speechley M, Ginter SF. Risk factors for fall
among elderly
persons living in the community. N Eng J Med 1988;319:1701-
1717.
16. Roqueta C, De Jaime E, Miralles R, Cervera AM.
Experiencia en la evaluación
del riesgo de caídas. Comparación entre el test Tinetti y el
Timed get Up &
Go. Rev Esp Geriatr Gerontol 2007;42:319-327.
17. Lázaro del Nogal M, González-Ramírez A, Palomo-Iloro A.
Evaluación del
riesgo de caídas. Protocolos de valoración clínica. Rev Esp
Geriatr Gerontol
2005;40:54-63.
18. Vinyoles Bargalló E, Vila Domènech J, Argimon Pallàs JM,
Espinàs Boquet
J, Abos Pueyo T, Limón Ramírez E; Los investigadores del
proyecto Cuído.
Concordance among Mini-Examen Cognoscitivo and Mini-
Mental State
Examination in cognitive impairment screening. Aten Primaria
2002;30:5-
13.
19. Lawton MP, Brody EM. Assessment of older people: Self-
maintaining and
instrumental activities of daily living. The Gerontologist
1969;9:179-186.
20. Mahoney FI. Functional evaluation: the Barthel index.
35. Maryland State Med
J 1965;14:61-65.
21. Bernaola-Sagardui I. Validation of the Barthel Index in the
Spanish
population. Aging Clin Exp Res. 2018;30:489-497.
22. Formiga F, Ruiz D, López Soto A, Duaso E, Chivite D,
Perez-Castejon JM.
Circunstancias asociadas a las caídas responsables de fractura
de fémur en
pacientes ancianos. Diferencias por grupo de edad y género.
Rev Clin Esp
2006;206:314-318.
23. Rubenstein L Z, Josephson KR. Falls and their prevention in
elderly people:
what does the evidence show? Med Clin N Am 2006;90:807-
824.
24. Espaulella, M. Tratamiento para la HTA y riesgo de caídas.
Sociedad Catalana
de Geriatría y Gerontología. http://scgig.cat/tratamiento-para-
la-hta-y-
riesgo-de-caidas-por-mariona-espaulella, accesses Feb 14, 2019
25. Yang Y, Hu X, Zhang Q, Zou R. Diabetes mellitus and risk
of falls in older
adults: a systematic review and meta-analysis. Age Aging
2016;45:761-767.
26. Costa Gameiro D. Efecto de la Vitamina D sobre el
rendimiento físico
en ancianos frágiles institucionalizados. Tesis Doctoral
Universidad de
Salamanca 2015.
36. 27. Bromfield SG, Ngameni CA, Colantonio LD, Bowling CB,
Shimbo D,
Reynolds K, Safford MM, Banach M, Toth PP, Muntner P.
Blood pressure,
antihypertensive polypharmacy, frailty and risk of serious
injury from falls
in adults treated with hypertension. Hypertension 2017;70:259-
266.
28. Martos Martín A. Variables medidoras en la relación entre
deterioro
cognitivo y la capacidad funcional en personas mayores, Tesis
doctoral
Universidad de Granada, 2005.
29. Salthaouse TA. The processing-speed theory of adult age
differences in
cognition. Psychol Rev 1996;103:403-428.
30. Salthaouse TA. Aging and measures of processing speed.
Biol Psychol
2000;54:35-54.
31. Palmer K, Wang HX, Backman L, Winblad B, Fratiglioni L.
Differential
evolution of cognitive impairment in nondemented older
persons: results
from the Kungsholmen Project. Am J Psychiatry 2002;159:436-
442.
86
Benítez et al. Functional Evaluation Tests as Prognostic Factors
37. of Falls in Elderly Patients Eur J Geriatr Gerontol 2019;1(3):78-
86
32. Ingles JL, Fisk JD, Merry HR, Rockwood K. Five-year
outcomes for dementia
defined solely by neuropsychological test performance.
Neuroepidemiology
2003;22:172-178.
33. Wilson RS, Aggarwal NT, Barnes LL, Bienias JL, Mendes
de Leon CF, Evans
DA. Biracial population study of mortality in mild cognitive
impairment and
Alzheimer disease. Arch Neurol 2009;66:767-772.
34. Guehne U, Luck T, Busse A, Angermeyer MC, Riedel-Heller
SG. Mortality
in individuals with mild cognitive impairment. Results of the
Leipzig
Longitudinal Study of the Aged (LEILA75+).
Neuroepidemiology
2007;29:226-234.
35. Ferrer A, Formiga F, Plana Ripoll O, Tobella MA, Gil A,
Pujol R; Octabaix
Study Group. Risk of falls in 85-year old is associated with
functional and
cognitive status: The Octabaix Study. Arch Gerontol Geriatr
2011;54:352-
356.
36. Bath PA, Morgan K. Differential risk factor profiles for
indoor and outdoor
falls in older people living at home in Nottingham, UK. Eur J
Epidemiol
1999;15:65-73.
39. in accordance with the terms of the License.
RESEARCH Open Access
‘Around the edges’: using behaviour
change techniques to characterise a
multilevel implementation strategy for a
fall prevention programme
S. McHugh1* , C. Sinnott2, E. Racine1, S. Timmons3, M.
Byrne4 and P. M. Kearney1
Abstract
Background: Implementation strategies are needed to ensure
that evidence-based healthcare interventions are
adopted successfully. However, strategies are generally poorly
described and those used in everyday practice are
seldom reported formally or fully understood. Characterising
the active ingredients of existing strategies is
necessary to test and refine implementation. We examined
whether an implementation strategy, delivered across
multiple settings targeting different stakeholders to support a
fall prevention programme, could be characterised
using the Behaviour Change Technique (BCT) Taxonomy.
Methods: Data sources included project plans, promotional
material, interviews with a purposive sample of
stakeholders involved in the strategy’s design and delivery and
observations of staff training and information
meetings. Data were analysed using TIDieR to describe the
strategy and determine the levels at which it operated
(organisational, professional, patient). The BCT Taxonomy
identified BCTs which were mapped to intervention
40. functions. Data were coded by three researchers and finalised
through consensus.
Results: We analysed 22 documents, 6 interviews and 4
observation sessions. Overall, 21 out a possible 93 BCTs
were identified across the three levels. At an organisational
level, identifiable techniques tended to be broadly
defined; the most common BCT was restructuring the social
environment. While some activities were intended to
encourage implementation, they did not have an immediate
behavioural target and could not be coded using
BCTs.
The largest number and variety of BCTs were used at the
professional level to target the multidisciplinary teams
delivering the programme and professionals referring to the
programme. The main BCTs targeting the
multidisciplinary team were instruction on how to perform the
(assessment) behaviour and demonstration of
(assessment) behaviour; the main BCT targeting referrers was
adding objects to the environment. At the patient level,
few BCTs were used to target attendance.
Conclusion: In this study, several behaviour change techniques
were evident at the individual professional level;
however, fewer techniques were identifiable at an
organisational level. The BCT Taxonomy was useful for
describing
components of a multilevel implementation strategy that
specifically target behaviour change. To fully and
completely describe an implementation strategy, including
components that involve organisational or systems level
change, other frameworks may be needed.
Keywords: Implementation, Intervention content, Behaviour
change, Fall prevention, Qualitative
42. An implementation strategy is typically a broad ‘package’
of techniques wrapped around, and often obscured by, the
intervention designed to produce health outcomes [5].
Distinguishing between an intervention and its implemen-
tation strategy is an important first step in testing the effi -
cacy of strategies and selecting appropriate outcomes to
assess implementation success [6].
Almost 10 years ago, Michie and colleagues highlighted
the poor and inconsistent description of complex behav-
iour change interventions [7]; terms were used inter-
changeably and the development and content of
interventions was rarely driven by an explicit theory of
change. The same weaknesses have been highlighted in
the design and reporting of implementation strategies: in-
consistent use of terminology, lack of conceptual clarity
and underutilisation of theory to select strategies [8]. Out-
side of research, the process for selecting the content of
an implementation strategy in the health system is also
likely to be unsystematic and atheoretical. For policy
makers, managers and healthcare professionals (HCPs)
tasked with introducing a clinical intervention, there is a
potentially confusing array of options [2]. Decisions are in-
fluenced by the type of intervention being implemented
and the context in which it is being introduced [9], and
health systems are increasingly constrained by competing
demands for attention and limited resources to make
change possible [10]. Also, strategies may be selected to
address expected barriers based on previous experience,
rather than targeting the most salient barriers that have
been identified systematically in advance. In an analysis of
quality improvement studies, Bosch and colleagues found
that the reasons for believing a particular strategy would
overcome a particular barrier to change were often not
explained [11].
Tools and checklists, such as the Template for Inter-
43. vention Description and Replication (TIDieR), have been
developed to guide the development and to standardise
reporting of complex interventions [5, 12–15]. The
TIDieR framework describes the main features of an
intervention and promotes the reporting of any activities
to enable or support an intervention [15]. Complemen-
tary tools have been developed in behavioural science,
which describe intervention and implementation activ-
ities in even greater detail using an agreed standardised
terminology [14, 16]. One of the most commonly applied
frameworks for defining activities in behaviour change
interventions is the Behaviour Change Technique (BCT)
Taxonomy [16]. The Taxonomy contains 93 discrete be-
haviour change techniques (BCTs) considered to be the
‘active ingredients’ of an intervention. A BCT is defined
as an ‘observable, replicable and irreducible component
of an intervention’ that has the potential to change be-
haviour [16]. BCTs serve different and often multiple
intervention functions.
The original development of BCT Taxonomy drew on six
classification systems of techniques used primarily to
change lifestyle behaviour, and the developers highlighted
the importance of examining the extent to which the tax-
onomy is generalizable across behaviours, disciplines and
countries [16]. It has been argued that successful imple-
mentation requires individuals at multiple levels to do
things differently [17]. Yet, the behaviours that support im-
plementation at the organisational level are often
overlooked or are poorly described. While individual organ-
isational theories focus on different organisatio nal factors
and how they influence the implementation processes [18],
the BCT Taxonomy potentially provides a way to systemat-
ically and comprehensively describe the behavioural aspects
44. of these processes at multiple levels, using an agreed ter -
minology. The extent to which the taxonomy can be used
to characterise the activities within a complex implementa-
tion strategy, operating at multiple levels of the health sys-
tem and targeting a range of stakeholders, is less well
understood. Few studies have applied the BCT Taxonomy
to retrospectively characterise implementation strategies.
Presseau et al. analysed implementation interventions for
diabetes prevention within the confines of randomised con-
trolled trials [17]; Steinmo et al. characterised an impl e-
mentation strategy used for a discrete clinical intervention
in an acute care setting [19]. In the latter example, health-
care professionals were the sole targets and the implemen-
tation strategy was delivered in a single setting.
We examined the utility of the BCT Taxonomy to
retrospectively characterise the content of an implemen-
tation strategy that was developed pragmatically (with-
out reference to theory), spans several settings and
targets multiple stakeholder groups. The strategy is be-
ing used to implement a fall risk assessment programme
for older people, an example of an evidence-based inter-
vention that has been the subject of over 100 interven-
tion trials [20] (see Additional file 1). However, there has
been suboptimal translation of this evidence into prac-
tice [20]. By describing the implementation strategy in
detail using a standardised framework and terminology,
we can move towards testing effectiveness and replica-
tion in other settings [5, 19, 21]. By retrospectively char -
acterising an existing implementation strategy, we will
also gain a better understanding of ‘implementation as
usual’ in the health system and identify targets for
improvement [22].
McHugh et al. Implementation Science (2018) 13:113 Page 2 of
13
45. Methods
We conducted a qualitative analysis, using multiple
sources of data, to build a comprehensive description
of the implementation strategy being used in the fall
prevention programme delivered in the Health Ser-
vice Executive (HSE) in Cork city and county (Re-
public of Ireland). Data were gathered concurrently
over a 6-month period (April–September 2016) (see
Additional file 2).
Document analysis
Documents describing the fall risk assessment clinics or
their implementation were provided by the implementa-
tion steering group. This multidisciplinary group of
health professionals and health service managers were
responsible for planning, managing and overseeing
implementation of clinics. We also collected documents
relating to the broader fall prevention pathway, promo-
tional material, referral forms and documents used by
staff during the fall risk assessment clinic (e.g. risk as-
sessment tool) (see Additional file 3 for an outline of the
documents included).
Interviews
Semi-structured face-to-face interviews were conducted
with a purposive sample from the 12-member imple-
mentation steering group. We followed the principles of
critical case sampling to select participants who would
yield the most information about day-to-day implemen-
tation [23]. As our aim was to examine whether the
content of an implementation strategy could be charac-
terised using the BCT Taxonomy as opposed to evaluat-
ing its acceptability among the target population or its
46. impact on behaviour change, we did not include inter-
views with staff and potential referrers in this analysis.
Potential participants were invited via email, telephone
or in person and were provided with an information
sheet outlining the study objectives. As the research lead
on the steering group, the lead researcher (SMH) was
known to participants.
During interviews, participants were asked to describe
what they did to support the set up and running of the fall
risk assessment clinics. The interview topic guide was in-
formed by TIDieR reporting tool for complex interven-
tions [15] and included probes on the implementation
processes, activities, their purpose and timing. Prompts
were added to the topic guide, informed by concurrent
observation and document analysis. Interviews were digit-
ally recorded and transcribed verbatim (ER).
Observation
One researcher (SMH) conducted unstructured observa-
tions of training sessions with multidisciplinary teams
(MDTs) delivering fall risk assessment clinics and
meetings with health professionals eligible to refer to the
clinics [24]. As the timing of sessions was determined by
those delivering and receiving the training a convenience
sample of interactions was selected. Observations took
place at two primary care sites where training and
the risk assessment clinics were being delivered (April–
June 2016). The researcher, who previously conducted
interviews with team members, adopted a ‘complete ob-
server’ role [25], attending with the explicit purpose of
collecting data and did not participate in the sessions.
Observation notes were taken to record the implemen-
ters’ actions and health professionals’ behaviours and re-
47. sponses in context. Notes were written up in full at the
end of each period of observation.
Analysis
All data sources (documents, interview transcripts and
observation notes) were imported into NVivo software
to support data management and analysis. Interviews
and observation notes were anonymised prior to analysis
and reporting.
Data analysis was guided by the principles of directed
content analysis, a deductive approach in which coding
can begin with predetermined codes [26]. Initially, data
were coded deductively (by SMH, trained in health ser-
vices research) using the TIDieR framework which
helped to clarify the underlying rationale for the imple-
mentation strategy [15]. Where possible, we also coded
the population and behaviour being targeted [21]. Data
were coded to identify what was carried out, at what
level (organisational, professional, patient), by whom,
how, where, when and how much and any planned tai-
loring or modification during the study period.
Data were then coded by one researcher (SMH) using
the BCT Taxonomy (version 1) of 93 techniques which
are organised into 16 categories. First, data were coded
to label potential BCTs and these segments of text were
checked carefully against BCT definitions to determine
whether a BCT was present or absent [16]. Once this
coding was complete, each BCT definition in the tax-
onomy was reviewed and the researcher (SMH) assessed
all three data sources for presence/absence of this BCT.
Implementation activities that did not fit with a BCT
taxonomy description were retained and coded using in
vivo codes (words and phrases used by participants in
the data).
48. A selection of the data was coded by two other re-
searchers, one familiar with the service through a wider
evaluation (ER—trained in public policy) and one who
was independent of the project (CS—primary care phys-
ician and clinical researcher). Each researcher coded a
document, field notes from one observation and an
interview transcript deemed (by SMH) to include the
richest description of the implementation strategy. All
McHugh et al. Implementation Science (2018) 13:113 Page 3 of
13
coders had participated in online BCT training and had
experience coding qualitative data. Coding discrepancies
were listed (by SMH) and reviewed by the coding team
(CS, ER). Researchers outlined their rationale for coding
a BCT, and the group reviewed the clarity and volume of
data available to support its presence. An accumulation
of segments of text led to greater certainty about the
presence or absence of a BCT rather than a single line
of text, so when an interview transcript was taken in its
entirety, researchers tended to code the same BCTs. In a
small number of cases where researchers identified dif-
ferent BCTs, this was typically due to different interpre-
tations of the target or purpose of the implementation
activity. These discrepancies were reviewed together and
resolved by discussing our individual coding rationale,
consulting other sources of data and drawing on the lead
researcher’s knowledge of the implementation context.
Outstanding discrepancies and uncertainties were
reviewed by a behavioural scientist with experience in
the use of BCTs (MB). Any resultant changes to coding
were applied across the data.
49. BCTs were mapped to intervention functions, guided
by data on the rationale and purpose of the implementa-
tion strategy and links between functions and BCTs out-
lined in the Behaviour Change Wheel Guide to Designing
Interventions [27].
Sampling, data collection and analysis were iterative.
As initial data were analysed, participants were recruited
using the same sampling and contact methods described
above and additional documents were sought to elabor-
ate on specific aspects of the implementation strategy.
We purposively chose a sample of critical cases, interac-
tions and documents that provided the best opportunity
to gather sufficient depth of information to fully describe
the implementation strategy being studied [28]. The
stages of analysis and codes were revisited multiple
times. We assessed construct saturation, whether the
conceptual categories of the BCT Taxonomy and inter-
vention functions were adequately populated, based on
the analysis of all data sources in consultation with the
definitions in the BCT Taxonomy.
Coding assumptions
We made a number of assumptions during analysis.
These assumptions were adapted from the approach
used by Presseau et al. to code multilevel implementa-
tion interventions [29]. First, we focused on techniques
used to support or enable the implementation of the fall
risk assessment clinics (implementation strategy), as dis-
tinct from techniques used during the risk assessment it-
self (clinical intervention).
Second, in line with the premise of the Behaviour
Change Wheel approach, we assumed that the imple-
mentation of an intervention depends on behaviour
50. change at some point [12]. We assumed that all BCTs
(included those at the system level) functioned by target-
ing the behaviour of health service managers, HCPs (re-
ferring to and/or running clinics) and patients, to
ultimately influence implementation outcomes.
Third, there were a range of target behaviours which
were broadly defined as ‘implementation behaviours’.
The specific behaviour varied depending on the actor
and level of the strategy being considered. In some cases,
the target behaviour was clear and thus BCTs were
coded at that level (e.g. referring clients to the clinic).
Where the specific target behaviour was not clear, BCTs
were coded at a more general level of ‘supporting the
implementation of the fall risk assessment clinics’.
Fourth, we considered a BCT to be present based on
an accumulation of text segments across a single source
of data or multiple sources (document, interview and/or
observation field notes). If it was unclear whether a BCT
was present or absent, following discussion and consid-
eration of multiple data sources, it was not coded. We
did not apply a minimum frequency of occurrence of
BCTs; techniques that occurred once were coded. Fifth,
planning and initial implementation occurred in tandem
with data collection. Therefore, some BCTs were
planned while others had taken place at the time of data
collection.
The Standards for Reporting Qualitative Research
(SRQR) was used to guide the reporting of findings (see
Additional file 4) [30].
Results
Twenty-two documents, six interviews and four observa-
51. tions were conducted across two implementation sites
(see Additional file 3).
Components of the implementation strategy and target
behaviours
Table 1 presents the main components of the implemen-
tation strategy, stratified by target level (i.e. organisa-
tional, professional or patient level) [15]. In summary, at
an organisational level, the implementation strategy in-
volved establishing a multidisciplinary steering group led
by a clinical project manager, appointing an implementa-
tion coordinator and administrator and assembling
multidisciplinary teams to deliver clinics. Multiple be-
haviours were targeted simultaneously at this level mak-
ing it difficult to identify a specific behavioural target;
thus, the target behaviour was defined broadly as ‘sup-
porting implementation of fall risk assessment clinics’.
Most of the implementation strategy targeted either (1)
the behaviour of professionals in the multi-disciplinary
team responsible for ‘delivering the fall risk assessment
clinic’ or (2) the behaviour of professionals ‘referring to
the clinic’ (including primary care physicians, public
McHugh et al. Implementation Science (2018) 13:113 Page 4 of
13
T
a
b
le
1
C
133. n
g
g
ro
u
p
McHugh et al. Implementation Science (2018) 13:113 Page 6 of
13
health nurses, physiotherapists, occupational therapists
and advanced nurse practitioners in emergency depart-
ments). At this level, the strategy focused on training and
ongoing ‘coaching’ for multidisciplinary teams, and stan-
dardised referral documentation and promotional meet-
ings with referrers. At the patient level, a standardised
invitation letter and information leaflet were developed to
encourage referred patients to ‘attend the clinic’.
The implementation strategy was tailored depending
on existing resources at each site, and communication
was ‘tailored to the requirements of different audiences’.
Other components were modified during initial imple-
mentation in response to the needs identified at each
site, for example the number of training sessions varied
according to the health professional and his/her
experience.
Behaviour Change Techniques (BCTs)
Overall, 21 out a possible 93 BCTs, from 14 of the 16
categories in the taxonomy, were identified (indicated in
italics). Table 2 illustrates the BCTs used at each level of
the implementation strategy (Additional file 5 describes
each BCT identified within each component, with sup-
134. porting data). The most commonly used BCTs were in-
struction on how to perform the behaviour and adding
objects to the environment.
BCTs and functions used at each level of the
implementation strategy
Organisational level
At the organisational level, the target behaviour was de-
fined as ‘supporting the implementation of fall risk as-
sessment clinics’. The steering group’s activities
concentrated ‘around the edges [of the programme],
problem solving and making sure that it’s presented well’
(interview). Overall, 11 BCTs were coded from six of the
16 categorises. The main BCT used was restructuring
the social environment.
Even within the organisational level, multiple layers of
BCTs were identifiable (see Additional file 5). For ex-
ample, we coded the establishment of the implementa-
tion steering group itself as restructuring the social
environment but there were also specific BCTs evident
within the work of the steering group such as ‘monitor-
ing and analysing pathway flows and activity, [to] adapt
and refine the [fall prevention] pathway’ (document).
This activity was coded as the steering group self-moni-
toring outcome(s) of behaviour to change their own im-
plementation activities. Similarly, members of the
steering group who were line managers ‘sold’ fall risk as-
sessment clinics to their staff using framing/reframing
and vicarious consequences (for older people):
‘I tell them it's an integrated service for an actual
screening tool to be used within the community, and
that they're the decision makers around it. They can
decide whether the client needs to be referred, they
can do the plan of care there and then [and] the client
135. can provide input for what they need.’ (interview)
Professional level
We classified target behaviours at the professional level
as behaviours relating to ‘delivering the fall risk assess-
ment clinic’ and those relating to ‘referring to the clinic’.
The largest number and variety of techniques were iden-
tifiable at the professional level. Overall, 16 techniques
were coded from 13 of 16 groups of BCTs.
The main BCTs used to target multidisciplinary pro-
fessionals tasked with ‘delivering the fall risk assessment
clinics’ were providing instruction on how to perform the
assessment and demonstration of assessment behaviour,
serving a training function. Training was delivered by a
credible source (implementation coordinator with clinical
expertise and experience in falls prevention) and in-
cluded verbal persuasion about capability. Previous ef-
forts to establish fall prevention services had failed
because of a lack of ‘practical support’ for health profes -
sionals, thus social support (unspecified and practical)
and problem solving were also used.
To support health professionals ‘referring to the clinic’,
a smaller number and range of BCTs were used. The
most common BCTs were adding objects to the environ-
ment (standardised referral form) which included
prompts and cues and using credible sources to meet
with referrers to persuade them to use the service.
Table 3 shows differences in the BCTs used to target the
range of HCPs eligible to refer to the service: primary
care physicians were told about the vicarious conse-
quences (shorter waiting times) of referring to the single
point of access; social comparison was used to persuade
public health nurses whereby colleagues involved in the
delivery of clinics would ‘(anonymously) feedback out-
136. comes of clients…, how this [clinic] works, and how they
[the clients] proceeded to the clinic’ (interview); and ad-
vanced nurse practitioners would receive feedback on
their referral behaviour.
BCTs relating to seven of nine intervention functions
were apparent in the implementation strategy. Most
BCTs were used to increase the means or reduce bar-
riers to increase capability or opportunity to carry out
behaviour (enablement function) (Additional file 5). The
two intervention functions not represented by any BCTs
were incentivisation and restriction. Only one BCT, be-
haviour cost, served a coercive function, to encourage
public health nurses to use a fall risk screening tool to
identify eligible clients for referral; ‘any aids or
McHugh et al. Implementation Science (2018) 13:113 Page 7 of
13
Table 2 Map of BCTs identified across levels and components
of the implementation strategy
Org organisational level, Prof professional level, Pt
patient/client level, PHN public health nurse
McHugh et al. Implementation Science (2018) 13:113 Page 8 of
13
appliances that people are applying for, they won’t be is-
sued unless there’s a falls screen’ (interview).
Patient level
137. At the patient level, the target behaviour was ‘attend-
ing the fall risk assessment clinic’ and in total, three
techniques were coded from three categories of BCTs.
The invitation letter and information leaflet contained
instruction on how to perform the behaviour (attend-
ing the clinic). There was brief information about the
health consequences and social consequences of at-
tending; the information leaflet indicated that clients
‘may be offered the opportunity to attend a falls edu-
cation class’ and ‘will be shown how to cope in the
event of a fall’.
Participants’ activities to shape knowledge, attitudes and
intentions to act in future
At the organisational level, we found many implementa-
tion activities could not be coded using any of the BCTs
and that they appeared to target attitudes rather than
immediate behaviour change. First, there were activities,
described as ‘the hustle’, to generate buy-in and foster
goodwill among key stakeholders. These activities ap-
peared to implicitly target stakeholders’ intentions to
support clinics in the future for example by releasing
staff and space to run clinics (target: heads of discipline)
or referring clients (target: health professionals eligible
to refer). Selling the clinics served the function of edu-
cating health professionals about their ‘existence’ and
purpose, but also sought to persuade potential referrers
about the benefits and ease of adopting the service.
‘[we tell them] you can’t do without [these clinics] but
it’s no trouble [to refer]’ (interview)
Second, piloting activities, which were evaluative and
reactive and did not align with goals and planning BCTs
such as reviewing behaviour and outcome goals, were
used at the first implementation site.
138. ‘What changed was the onward referral form and the
process of who we were referring on to, and what
form they got and what level of information they got
or needed. That changed really on a weekly basis in
clinic 1.’ (interview)
Discussion
Summary
We examined the utility of the BCT Taxonomy to char-
acterise the content of a real-world implementation
strategy targeting a range of stakeholders across organ-
isational boundaries. Overall, 21 distinct BCTs were used
to restructure the environment for implementation and
to train, educate, enable and persuade health profes-
sionals and patients. Of the nine possible intervention
functions, none of the techniques sought to restrict be-
haviour or incentivise behaviour change. While we iden-
tified several techniques at the individual professional
level, fewer techniques were identifiable at an organisa-
tional level. Furthermore, some implementation activ-
ities at this level did not target immediate behaviour
change. The utility and application of implementation
strategies could be improved by adopting a systematic
Table 3 Map of BCTs identified according to target group of
referrers
McHugh et al. Implementation Science (2018) 13:113 Page 9 of
13
approach using a theory-based framework which identi-
fies active ingredients and offers the potential to under -
stand mechanisms of change [13, 29, 31]. However, to
139. accurately describe and fully understand a multilevel im-
plementation strategy, the behavioural approach may
need to be integrated with organisational theories of
change.
Utility of the BCT Taxonomy
Like Steinmo et al., we found that this systematic ap-
proach could be applied ‘post hoc’ to an existing imple-
mentation strategy that was developed pragmatically
based on organisational knowledge and experience.
Building on their analysis of an implementation strategy
targeting professional behaviour in the hospital setting,
our results show that the BCT Taxonomy is also applic-
able to wider implementation strategies which target
multiple groups across different healthcare settings.
Similar to Presseau et al., who examined randomised
controlled trials of diabetes implementation interven-
tions, we found that a small number of the possible
BCTs (21/93) were used to support the introduction of a
fall prevention programme. The main techniques used
to target professional behaviour, including instruction on
how to perform behaviour, adding objects to the envir-
onment, prompts and cues and social support, were
similar across all three studies. The popularity of certain
BCTs and the narrow range being used in implementa-
tion strategies highlights the potential for practitioners
and researchers to think creatively about implementa-
tion by drawing on other techniques listed in the BCT
Taxonomy [29].
Characterising organisational-level implementation
activities and their targets
In this study, fewer BCTs were identifiable at the organ-
isational level compared to the professional level. Tech-
niques at the organisational level tended to be broadly
defined BCTs, such as restructuring the social environ-
140. ment, which were not necessarily specific to the clinical
context of fall prevention. Our findings highlight some
of the more specific techniques, such as action planning
and problem solving, used to operationalise this broad
BCT at an organisational level. Rather than simply listing
the BCT ‘ingredients’ in an implementation strategy, we
believe that techniques should be linked to specific
components and levels of delivery in the strategy’s
description.
Some activities did not have an immediate behavioural
target, highlighting the importance of measuring prox-
imal outcomes (such as attitudes and beliefs) as well as
distal outcomes (like changes in behaviour) when evalu-
ating implementation strategies. Although the ultimate
goal of implementation may be behaviour change,
immediate goals include changing organisational deter-
minants of behaviour such as policy and procedures,
staffing and resource allocation [32–34]. It could be ar-
gued that the recruitment of dedicated staff to coordin-
ate implementation, an example of restructuring the
social environment and a resource which enabled most
components of the implementation strategy in this
study, is targeting organisational as well as individual de-
terminants of change. Research on implementation cli-
mate suggests that when organisations align their
policies, practices and resources to support implementa-
tion, staff have a clearer understanding of the priorities
and value placed on an intervention, and thus are more
likely to change their behaviour accordingly [35].
Practical implications
The systematic process of characterising and reporting
an implementation strategy may prompt those designing
and delivering strategies to think about the intended tar-
141. get(s) and expected outcomes of their activities. Outside
of research studies, the process of specifying existing im-
plementation strategies using approaches such as the
BCT Taxonomy may be difficult to navigate in practice
without support, given the number and granularity of
techniques, and the specific terminology. An overarching
framework, such as the AIMD (Aims, Ingredients,
Mechanism, Delivery), may be a useful and efficient
starting point for health care professionals, funders,
managers and policy makers seeking to formally describe
interventions. This simplified framework is deliberately
‘terminology agnostic’ to promote collaboration across
related fields including quality improvement, policy,
public health, patient safety and behaviour change [32].
As a meta-framework, it accommodates the use of spe-
cific frameworks such as BCT Taxonomy for particular
purposes.
Characterising an existing strategy using a well-established
framework provides an in-depth understanding of
‘implementation as usual’ in the health system and
highlights gaps that can be addressed to refine imple-
mentation and maximise effectiveness. For example,
in this study, few behaviour change techniques were
used to target older peoples’ attendance at the fall
prevention programme. Client engagement is a
well-established problem for fall prevention pro-
grammes; a systematic review of uptake rates in clin-
ical trials of fall prevention interventions reported
non-attendance rates as high as 42% [36]. The imple-
mentation strategy in this study did not include any
monitoring and feedback techniques to target health
professionals referring to the service or those health
professionals delivering the service. Yet data on refer -
rals and assessment outcomes were collected and ana-
lysed to facilitate self-monitoring and action planning
142. McHugh et al. Implementation Science (2018) 13:113 Page 10
of 13
among the implementation steering group. Given the
availability of valid routine data with mechanisms for audit
and feedback from trusted sources within the health ser-
vice and the substantial evidence of effectiveness for chan-
ging professional behaviour [37], there is potential to trial
different approaches to and components of audit and
feedback within this ongoing organisational initiative [38].
This study identified the behaviour change techniques
planned or used during the initial implementation of fall
risk assessment clinics in the health service. This is likely
only a sample of the techniques that will be used over
the course of implementation. Indeed, from the outset,
the number and type of behaviour change techniques
varied depending on the target group and context; differ-
ent techniques were used to target referral behaviour
among primary care physicians, advanced nurse practi-
tioners in hospitals and public health nurses working in
the community. It is widely acknowledged that imple-
mentation strategies should be tailored to the local con-
text [39]. Further research is being conducted with the
health professionals and clients to explore their experi -
ences of implementation and perceptions of the accept-
ability and appropriateness of the implementation
strategy. We will combine these results with our current
understanding of the content and function of the imple-
mentation strategy to address gaps or barriers to its
success.
Strengths and limitations
143. The TIDieR framework helped us to clarify the under-
lying rationale for the implementation strategy and thus
the intended target population for some activities [15].
We supplemented the TIDieR framework with a descrip-
tion of the ‘action targets’ [21], that is population and
behaviour being targeted by activities, which was neces-
sary before coding behaviour change techniques.
It was not feasible to observe every interaction, par-
ticularly at an organisational level, given the dynamic
and often unpredictable nature of implementation and
the number of actors and settings involved. Therefore,
some BCTs at the organisational level may have been
missed. While the number of interviews and observa-
tions in this study is small, the underlying sampling ra-
tionale was to generate a rich and thick description of
the content of an implementation strategy. Thus, our
sampling was not driven solely by numbers of interviews
but also the appropriateness of the data. A purposively
chose sample of participants, interactions and docu-
ments provided the best opportunity to gather sufficient
depth of information to fully describe the implementa-
tion strategy being studied [28, 40]. Given our use of
deductive content analysis with a pre-determined frame-
work, we focused on construct saturation over the con-
cept of theoretical saturation from grounded theory.
Data collection and sampling was iterative; however, the
process of judging saturation may have been facilitated
and enhanced by the use of explicit a prior stopping cri -
teria which have been used in theory-based interview
studies [41]. The identification of BCTs was influenced
by the richness of description and the specificity of BCT
definitions. As mentioned previously, the definitions of
some BCTs are relatively broad which could increase the
ease and frequency with which they are coded. Interview
144. participants did not naturally describe their work activ-
ities in the language of BCTs. Data from interviews were
triangulated with data from documents and observations
which provided reassurance about the presence or ab-
sence of a BCT [42]. BCTs were typically coded from an
accumulation of evidence across data sources rather
than relying on a single source.
In line with the Medical Research Council guidance
for process evaluations of complex interventions, which
warns against forcing an established framework to fit in-
terventions which were not originally designed based on
theory [43], we used participants’ own language to code
and preserve aspects of the implementation strategy that
were not adequately or accurately described using BCT
definitions.
In this study, we did not evaluate the performance of
behaviour change techniques and therefore cannot com-
ment on the degree to which they were consistently de-
livered as intended or their impact on behaviour change.
Capturing what is delivered in practice is essential for
evaluators to identify adaptations that may undermine
or enhance effectiveness [43]. Variability in the way pro-
fessionals deliver an implementation strategy is to be ex-
pected as they try to respond appropriately to the needs
of the target group and changing context. Hence, sys-
temisation may not always be feasible [44].
Conclusions
We examined the utility of the BCT Taxonomy for charac-
terising the content of a multilevel implementation strategy
used in the ‘real world’ to support an evidence-based fall
prevention intervention for older people. Using the BCT
Taxonomy, we identified several techniques at the profes-
sional level but fewer techniques that constitute implemen-
145. tation behaviour at an organisational level. Some activities
did not have an immediate behavioural target thus to fully
and accurately describe a multilevel implementation strat-
egy, other organisational frameworks may be needed. Im-
proving the ability of health service managers, clinicians
and researchers to firstly consider and, if possible,
formalise the content of implementation strategies
would facilitate the testing, replication and refinement
of implementation strategies, ultimately maximising
the value of existing and future clinical-focussed re-
search for healthcare providers and patients.
McHugh et al. Implementation Science (2018) 13:113 Page 11
of 13
Additional files
Additional file 1: Outline of Fall Risk Assessment Clinics.
Figure
depicting the organisation and main features of fall risk
assessment
clinics being supported by the implementations strategy. (PDF
172 kb)
Additional file 2: Timeline of initial implementation at two
primary care
sites and data collection for study. Figure depicting the timeline
of initial
implementation including the timing of clinics being set up and
the
implementation strategy being delivered and the overlap with
data
collection for the current study. (PDF 177 kb)
146. Additional file 3: Documents collated and analysed. Table of
the
documents collated and analysed in the study. (PDF 189 kb)
Additional file 4: Standards for Reporting Qualitative Research
(SRQR)
Checklist. (PDF 328 kb)
Additional file 5: List of BCTs and functions used at the
organisational
level targeting behaviours ‘supporting the implementation of
fall risk
assessment clinics’. Table outlining the activities undertaken
within each
component of the implementation strategy, the BCT coded to
that
activity and the intervention function(s) it served. (PDF 358 kb)
Abbreviations
ANP: Advanced nurse practitioner; BCT: Behaviour Change
Technique;
GP: General practitioner; HCP: Healthcare professional; MDT:
Multidisciplinary
team; PHN: Public health nurse; TIDieR: Template for
Intervention Description
and Replication
Acknowledgements
We thank the members of the Integrated Fall and Fracture
Prevention
Pathway Steering Group in Community Health Organisation 4
within the
Health Service Executive (HSE). We wish to acknowledge
Finola Cronin, Orla
Hosford, Eileen Moriarty, Olivia Wall, Liz O’Sullivan, Dr.
Patrick Barry and
147. Dr. Kieran O’Connor for designing and delivering the
implementation
strategy and for facilitating access to documents for this study.
We also
thank the multidisciplinary teams of health professionals
involved in the
delivery of the fall risk assessment clinics for allowing us to
visit their
clinics. We thank the health professionals involved in
information
sessions for allowing us access to their meetings.
Funding
Dr. S McHugh would like to acknowledge the funding of the
Fellowship by
the Centre for Ageing Research and Development in Ireland
(CARDI) which
became the Ageing Research and Development Division within
the Institute
of Public Health in Ireland (IPH) in September 2015. Professor
Patricia
Kearney and Professor Molly Byrne are funded by the Health
Research Board
Research Leader Awards in diabetes (RL/2013/7) and health
behaviour
change (RL/2013/8) respectively.
Availability of data and materials
The datasets used and/or analysed during the current study are
available
from the corresponding author on reasonable request.
Authors’ contributions
SMH was the principal investigator on this study and was
responsible for its
conception. All authors contribute to the development of the
148. research
objectives and methods. SMH conducted the data collection. ER
transcribed
and collated the data. SMH, ER and CS were involved in
analysing and
interpreting the data. MB reviewed the analysis and
interpretation of data.
SMH wrote the first draft of the paper. All other authors
contributed to
successive drafts. All authors read and approved the final
manuscript.
Ethics approval and consent to participate
This study received ethical approval from the Clinical Research
Ethics
Committee for Cork Teaching Hospitals (CREC), and
participants provided
consent prior to taking part.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional
claims in
published maps and institutional affiliations.
Author details
1School of Public, University College Cork, Cork, Ireland.
2THIS Institute (The
Healthcare Improvement Studies Institute), University of
Cambridge,
Cambridge, UK. 3Center for Gerontology and Rehabilitation,
149. University
College Cork, Cork, Ireland. 4Health Behaviour Change
Research Group
(HBCRG), School of Psychology, National University of Ireland
Galway,
Galway, Ireland.
Received: 12 April 2018 Accepted: 23 July 2018
References
1. Plsek P. Redesigning Health Care with Insights from the
Science of Complex
Adaptive Systems. In: Institute of Medicine (US), editor.
Crossing the Quality
Chasm: A New Health System for the 21st Century. Washington
(DC):
National Academies Press (US); 2001. p. 309–22.
2. Grol R, Grimshaw J. From best evidence to best practice:
effective
implementation of change in patients’ care. Lancet.
2003;362(9391):1225–30.
3. Flodgren G, Parmelli E, Doumit G, et al. Local opinion
leaders: effects on
professional practice and health care outcomes. Cochrane
Database Syst
Rev. 2011;(8):CD000125.
https://doi.org/10.1002/14651858.CD000125.pub4
4. Pinnock H, Barwick M, Carpenter CR, Eldridge S, Grandes
G, Griffiths CJ, et al.
Standards for reporting implementation studies (StaRI)
statement. BMJ.
2017;356 https://doi.org/10.1136/bmj.i6795.
150. 5. Proctor EK, Landsverk J, Baumann AA, Mittman BS, Aarons
GA, Brownson
RC. The implementation research institute: training mental
health
implementation researchers in the United States. Implement Sci.
2013;8
https://doi.org/10.1186/1748-5908-8-1.
6. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne
AM. An introduction
to implementation science for the non-specialist. BMC
psychology. 2015;3(1):32.
7. Michie S, Fixsen D, Grimshaw JM, Eccles MP. Specifying
and reporting
complex behaviour change interventions: the need for a
scientific method.
Implementation Sci. 2009;4:40. https://doi.org/10.1186/1748-
5908-4-40.
8. Waltz TJ, Powell BJ, Chinman MJ, Smith JL, Matthieu MM,
Proctor EK, et al.
Expert recommendations for implementing change (ERIC):
protocol for a
mixed methods study. Implement Sci. 2014;9(1):39.
9. Powell BJ, Beidas RS, Lewis CC, Aarons GA, McMillen JC,
Proctor EK, et al.
Methods to improve the selection and tailoring of
implementation
strategies. J Behav Health Serv Res. 2017;44(2):177–94.
https://doi.org/10.
1007/s11414-015-9475-6.
10. Coiera E. Why system inertia makes health reform so
151. difficult. BMJ. 2011;342
https://doi.org/10.1136/bmj.d3693.
11. Bosch M, van der Weijden T, Wensing M, Grol R. Tailoring
quality improvement
interventions to identified barriers: a multiple case analysis. J
Eval Clin Pract.
2007;13(2):161–8. https://doi.org/10.1111/j.1365-
2753.2006.00660.x.
12. Michie S, van Stralen MM, West R. The behaviour change
wheel: a new
method for characterising and designing behaviour change
interventions.
Implement Sci. 2011;6(1):42.
13. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith
JL, Matthieu MM,
et al. A refined compilation of implementation strategies:
results from the
expert recommendations for implementing change (ERIC)
project.
Implement Sci. 2015;10(1):21. https://doi.org/10.1186/s13012-
015-0209-1.
14. Kok G, Gottlieb NH, Peters G-JY, Mullen PD, Parcel GS,
Ruiter RAC, et al. A
taxonomy of behaviour change methods: an intervention
mapping
approach. Health Psychol Rev. 2016;10(3):297–312.
https://doi.org/10.1080/
17437199.2015.1077155.
15. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R,
Moher D, et al.
Better reporting of interventions: template for intervention