The clinical management of patients with polycystic ovarian syndrome PCOS in ...
JOP Perio OSA article
1. Investigating the Association Between
Obstructive Sleep Apnea and Periodontitis
Weiqiang Loke,* Thomas Girvan,† Paul Ingmundson,‡ Ronald Verrett,§ John Schoolfield,*
and Brian L. Mealey*
Background: Obstructive sleep apnea (OSA) is a sleep dis-
order characterized by disruptions of normal sleep archit-
ecture. Chronic periodontitis is a chronic disease of the
periodontium that elicits a general inflammatory response to
local dental plaque. It has been suggested that periodontal dis-
ease may increase in severity with increasingly severe OSA
because both disease entities share common inflammatory
pathways, acting synergistically to alter the host response.
The aim of this study is to analyze the association between se-
verity of OSA and the prevalence/severity of periodontitis.
Methods: One hundred patients from a large veterans ad-
ministration sleep study center (n = 26 normal, n = 21 mild,
n = 19 moderate, n = 34 severe) diagnosed with an overnight
polysomnogram underwent a comprehensive periodontal ex-
amination. Periodontal parameters measured included the fol-
lowing: 1) mean periodontal probing depth (PD); 2) clinical
attachment level (CAL); 3) gingival recession; and 4) percent-
age of sites with bleeding on probing, plaque, PD ‡5 mm, and
CAL ‡3 mm.
Results: Seventy-three percent of the sampled population
had moderate/severe periodontal disease. x2 analyses
revealed no significant differences in the prevalence of peri-
odontal disease between the apnea–hypopnea index (AHI)
groups, with a negligible Spearman correlation coefficient of
0.246 between AHI severity and periodontal disease severity
categories. Analysis of covariance indicated a significant asso-
ciation between AHI severity categories and percentage of
sites with plaque, after adjusting for age. Multivariable logis-
tic regression analysis predicting moderate/severe peri-
odontitis with AHI score, age, and smoking status indicated
a significant association with age (P = 0.028) but no signifi-
cant association with the other two predictors.
Conclusion: OSA was not significantly associated with the
prevalence of moderate/severe periodontitis and the peri-
odontal parameters examined, except percentage plaque.
J Periodontol 2015;86:232-243.
KEY WORDS
Chronic periodontitis; sleep apnea, obstructive.
O
bstructive sleep apnea (OSA) is
a sleep disorder characterized
by periodic and repetitive par-
tial or complete collapse of the upper
airway during sleep, resulting in reduced
ventilation (hypopnea) or absent venti-
lation (apnea) and, consequently, disrup-
tions of normal sleep architecture and
associated arterial desaturations.1,2 OSA
is currently diagnosed with an overnight
sleep diagnostic test known as a poly-
somnogram (PSG), which remains the
gold standard of diagnosis.3 The stan-
dard definition of an apneic event in-
cludes a minimum 10-second interval
between breaths, with a neurologic arousal,
a blood oxygen desaturation of 3% to
4% or greater, or both arousal and de-
saturation.4-6 Hypopnea is defined as
an episode of shallow breathing (air-
flow reduced by ‡50%) during sleep,
lasting for ‡10 seconds and usually
associated with a fall in blood oxygen
saturation attributable to partial ob-
struction of the upper airway.1
The apnea–hypopnea index (AHI)4 is
a commonly used index to categorize
the severity of OSA, and it represents
the average number of apneas and/or
hypopneas per hour of recorded sleep.
In adults, an AHI of less than five events
per hour is considered normal. Mild
OSA is defined as an AHI of at least five
to 15 events per hour, moderate OSA
as >15 to 30 events per hour, and se-
vere OSA as >30 events per hour.
The underlying mechanisms of OSA
are primarily associated with upper airway
* Department of Periodontics, University of Texas Health Science Center at San Antonio
Dental School, San Antonio, TX.
† Sleep Clinic, South Texas Veterans Health Care System, Veterans Administration
Facility, San Antonio, TX.
‡ Dental Clinic, South Texas Veterans Health Care System, Veterans Administration
Facility.
§ Department of Comprehensive Dentistry, University of Texas Health Science Center at
San Antonio Dental School.
doi: 10.1902/jop.2014.140229
Volume 86 • Number 2
232
2. anatomy, dilator muscle dysfunction, lung volume,
or ventilatory control stability.7 Ongoing studies
also suggest other possible pathophysiology path-
ways that include local and systemic inflammation8
and clock gene dysfunction.9 Neuropsychiatric com-
plications associated with OSA include daytime
somnolence, cognitive dysfunction, depression, and
Alzheimer’s disease.10-12 OSA has been associated
with an increased risk for development of vascular
disorders, such as coronary heart disease, hyperten-
sion, stroke, congestive cardiac failure, and ath-
erosclerosis, as well as metabolic disorders, such as
impaired glucose tolerance and insulin resistance.11
Although the exact pathogenesis pathway of OSA
leading to such complications is uncertain, studies
have suggested the role of OSA in activation of
various inflammatory processes through hypoxia
and oxidative stress-induced reperfusion injury
from intermittent hypoxia during apneic events in
OSA.12,13 Currently, treatment for OSA is confined
to relief of the mechanical obstruction rather than
focusing on the functional aspect of the disease.14
Better understanding of the underlying pathophys-
iology may bring about new and novel treatment
strategies in the future.15
The biofilm derived from dental plaque in peri-
odontitis is capable of adding to pre-existing sys-
temic inflammatory burden through elevation of
serum levels of C-reactive protein16 and a host of
other important inflammatory cytokines and medi-
ators.17-19 The resultant inflammatory response from
periodontitis coupled with genetic and environ-
mental risk factors could potentiate any existing
inflammatory disease. A pilot study performed by
Gunaratnam et al.20 found a higher prevalence of
periodontitis among patients with OSA, suggesting
a possible association between OSA and periodontitis.
Because treatment of periodontitis has been shown
to improve systemic inflammation, metabolic control
of glycemia, and parameters of vascular health,21,22
treatment of periodontitis may prove to be one of
the future, novel ways to improve OSA.
Epidemiologically, data from several OSA stud-
ies accomplished with PSG suggest that the prev-
alence of OSA is between 5% and 28%,23-27 with
higher prevalence in males. Periodontitis is also
a common chronic disease with a high prevalence.
According to the most recent National Health and
Nutrition Examination Survey 2009 to 2010, 47% of
adults aged >30 years have chronic periodontitis
(CP), distributed as a prevalence of 8.7%, 30%, and
8.5% with mild, moderate, and severe forms of peri-
odontitis, respectively.28
The aim of this study is to determine whether
OSA has any association with periodontitis. In par-
ticular, the association between OSA severity and
the prevalence of periodontitis was investigated. In
addition, the relations between OSA severity and
various clinical parameters of periodontal disease
status were examined.
MATERIALS AND METHODS
This cross-sectional study was conducted from
June 2012 to August 2013 after approval by the
Institutional Review Board of the University of Texas
Health Science Center and the South Texas Veterans
Health Care System, Veterans Administration (VA)
facility, San Antonio, Texas (protocol no. HSC12-123H).
All patients provided written informed consent be-
fore participation. Patients (n = 100) were recruited
by purposive consecutive sampling from the pool of
patients who were scheduled for PSGi evaluation6 at
the South Texas Veterans Health Care System facility,
San Antonio, Texas. The participants included 91
males and 9 females, aged 28 to 79 years; mean
age: 52.6 years), with a final total of 26 individuals
in the normal, 21 in the mild, 19 in the moderate,
and 34 in the severe AHI groups examined. Addi-
tional patient demographics are presented in Table
1. The population sampled at the VA hospital has
a bias toward males, with males accounting for 91%
of the data represented (Table 1). In terms of eth-
nicity, the distribution surveyed is representative of
the U.S. population, with a majority of the pop-
ulation sampled being white.
A comprehensive periodontal evaluation was per-
formed for each patient by a single examiner (WL)
immediately before the PSG; thus, the examiner
was masked to the patient’s OSA category. After
PSG, the patients diagnosed with varying degrees of
OSA (test group) were stratified into the following
categories: mild, moderate, and severe according to
the AHI. At the same time, those patients whose
PSG determined that they did not have OSA acted
as the control group. All patients had to have a
minimum of 16 remaining natural teeth to be in-
cluded in the study.
Before the periodontal examination, patient-level
variables that are putative confounders, such as body
mass index (BMI), diabetes, and smoking history,
were recorded during the patient examination in
detail as follows. The BMI was calculated for each
patient from data available in the chart. If the pa-
tient had diabetes, the chart was reviewed to de-
termine the most recent hemoglobin A1c (HbA1c)
(laboratory results had to be taken within the 6
months before the periodontal examination). Smok-
ing history was determined by questioning patients
and categorized as follows: 1) non-smoker (never
smoked); 2) former smoker (smoked but quit before
i Easy III PSG System, Cadwell Laboratories, Kennewick, WA.
J Periodontol • February 2015 Loke, Girvan, Ingmundson, Verrett, Schoolfield, Mealey
233
3. the study; time since quitting was determined in
months); and 3) current smoker. Current smokers
and former smokers who quit within the past 6
months were excluded from the study.
The inclusion criteria for the OSA patients were
as follows: 1) mild (AHI of at least five to 15 per
hour), moderate (AHI >15 to 30 per hour), and
severe (AHI >30 per hour) OSA; 2) aged ‡30 years;
3) non-smokers or former smokers who quit at least
6 months before the examination; 4) no history of
acute coronary syndrome; 5) American Society of
Anesthesiologists (ASA) Class I or II; and 6) pa-
tients with diabetes only included if glycemic con-
trol was good to moderate (documented HbA1c
within the past 6 months £8%).
The periodontal examination included a full peri-
odontal charting at six points per tooth (mesio-facial,
mid-facial, disto-facial, disto-lingual, mid-lingual,
and medio-lingual), excluding third molars, recording
probing depth (PD), recession (REC), and clinical
attachment level (CAL). Bleeding on probing (BOP)
was assessed at six points per tooth and recorded
as either present or absent within 15 seconds of
probing. The presence of visible plaque was eval-
uated at four sites per tooth (mid-mesial, mid-facial,
mid-distal, and mid-lingual) and recorded as present
or absent. Periodontal variables were examined for
differences across all four categories of OSA (none,
mild OSA, moderate OSA, and severe OSA). After
comprehensive clinical periodontal examination,
the periodontal variables were assessed for both the
test and control groups to determine relations with
sleep apnea and were recorded as follows for each
patient: 1) mean periodontal PD; 2) mean CAL; 3)
mean REC; 4) percentage of sites with BOP as
a measure of gingival inflammation; 5) percentage
of sites with plaque; 6) percentage of sites with PD
‡5 mm; and 7) percentage of sites with CAL ‡3 mm.
The definitions of periodontitis used in this study
are the American Academy of Periodontology (AAP)/
Centers for Disease Control and Prevention (CDC)
definitions of periodontal disease as described by
Eke et al:29 1) mild periodontitis, defined as two or
more interproximal sites with attachment loss (AL)
‡3 mm and at least two interproximal sites with PD
‡4 mm (not on the same tooth) or one site with ‡5
mm; 2) moderate periodontitis, defined as two or
more interproximal sites with AL ‡4 mm (not on the
same tooth) or two or more interproximal sites with
PD ‡5 mm, also not on the same tooth; and 3) severe
periodontitis, defined as two or more interproximal
sites with AL ‡6 mm (not on the same tooth) and one
or more interproximal site(s) with PD ‡5 mm.
Statistical Analysis
The association between OSA and periodontal
disease was analyzed using statistical methods that
treated OSA as an exposure factor and periodontal
diagnosis as outcome. Because OSA was represented
by both ordinal (AHI classification) and continuous
(observed AHI count) measures and periodontal
diagnosis was represented by dichotomous, ordinal,
and continuous measures, several statistical methods
were used.
For the purposes of a priori power analysis, a
one-way analysis of variance (ANOVA) comparing
means for a continuous value periodontal index
across the four classifications of OSA severity was
considered. Based on equal sample sizes of 25
patients per group, the proposed total sample of
100 patients achieves 91% power to reject the null
hypothesis of equal means using an F test with
a 0.05 significance level if the population effect size
is ‡0.39. To achieve this effect size, the standard
deviation of the four group means needs to be ‡39%
of the common standard deviation within groups.
This effect size requires a clinically significant mean
difference of one common standard deviation to be
present for the sample population between the control
group and at least one of the OSA severity groups.
Statistical analyses to assess associations between
OSA severity represented as an ordinal grouping
variable (normal, mild, moderate, severe) and de-
mographic and periodontal variables were performed
using x2 tests for categoric measures, Spearman rank
correlations for ordinal and continuous measures,
and analysis of covariances (ANCOVAs) for peri-
odontal indices with age as a covariate. When small
Table 1.
Frequency of Patient Characteristics (by
AHI classification)
Characteristic Normal Mild Moderate Severe Total
Ethnicity
African American 4 2 1 8 15
White 16 13 13 16 58
Hispanic 6 3 5 10 24
Other 0 3 0 0 3
Sex
Females 4 3 2 0 9
Males 22 18 17 34 91
Smoking history
Former smoker 6 2 6 11 25
Non-smoker 20 19 13 23 75
Diabetes
Absent 24 17 13 22 76
Present 2 4 6 12 24
Total 26 21 19 34 100
Obstructive Sleep Apnea and Periodontitis Volume 86 • Number 2
234
4. expected frequencies were observed, Fisher exact
tests were substituted for x2 tests. If the F test for
the main effect for OSA severity was significant for
ANCOVA, then age-adjusted mean comparisons
were performed for the severe group versus the
normal, mild, and moderate OSA groups.
Additional analyses were performed to assess as-
sociations between continuous AHI scores and de-
mographic and periodontal variables using Spearman
rank correlations for ordinal and continuous mea-
sures and multivariable logistic regressions pre-
dicting moderate/severe periodontitis using 10-unit
increments for AHI. Hosmer-Lemeshow goodness-
of-fit tests were performed to verify the validity of
multivariable logistic regression models. The num-
ber of predictors for logistic regression was limited
to the smaller number of patients between negatives
and positives for moderate/severe periodontitis di-
vided by 10. For statistical tests, P <0.05 was con-
sidered significant. The 95% confidence intervals
(CIs) were calculated for correlation coefficients.
Assuming all correlations to be positive, then cor-
relation coefficients with a lower 95% CI bound >0.20
were considered to be meaningful, between 0.10
and 0.20 were considered to be small, and <0.10
were considered to be negligible, similar to the rule
of thumb for interpreting the size of a correlation
coefficient proposed by Hinkle et al.30 Statistical
analyses were performed using statistical software.¶
In addition to age, demographic variables included
continuous measures of BMI and categoric pa-
rameters of ethnicity (classes), sex (males/females),
diabetes (presence/absence), and smoking history
(non-smoker/former smoker).
RESULTS
Patient Enrollment
The mean – SD for age in the normal, mild, mod-
erate, and severe AHI categories were 44.0 – 12.9,
55.4 – 13.4, 58.6 – 12.6, and
54.2 – 11.8, respectively. BMI in
the normal, mild, moderate, and
severe AHI categories were 31.9 –
7.1, 32.0 – 5.3, 32.5 – 4.3, and
36.6 – 6.9, respectively. Fisher
exact tests indicated no significant
relation among AHI classification
and ethnic categories (P = 0.174)
or sex (P = 0.065). x2 analysis also
revealed no significant relation
among AHI classification and his-
tory of past smoking or no
smoking (P = 0.245) or the pres-
ence or absence of diabetes (P =
0.070).
Association Between AHI Classification and
Periodontal Disease
The main objective of this study is to examine the
association between AHI severity and periodontal
disease prevalence and severity (Table 2). The
prevalence of moderate/severe periodontitis in the
sampled population, defined according to the AAP/
CDC classification, was 73%. This is almost twice as
high as the 38.5% prevalence of moderate and se-
vere periodontitis found in the most recent study of
the United States population.28
When comparing the percentage of patients with
moderate/severe periodontitis across the four AHI
groups (Table 2), the x2 test did not indicate any
statistically significant differences among AHI
groups (P = 0.111). The largest percentage differ-
ence between groups was for normal AHI (57.7%)
versus severe AHI (85.3%).
Because of the high prevalence of moderate/
severe periodontitis in the study population, a post
hoc power analysis was performed to determine the
sample size needed to detect significant AHI group
differences in prevalence of moderate/severe peri-
odontitis. If the sample size was doubled to 200
patients, then the sample size would be sufficient to
detect AHI group differences by x2 test at the 0.05
level with a power of 84%.
When analyzing the Spearman correlations be-
tween the two main variables in this study— AHI
classification (normal, mild, moderate, severe) and
periodontal disease classification (none, mild, mod-
erate, severe)—the correlation coefficient is negli-
gible (r = 0.246, 95% CI = 0.052 to 0.422). Small or
negligible correlations were also found between peri-
odontal disease classification and both age (r = 0.317,
95% CI = 0.128 to 0.483) and BMI (r = 0.179, 95%
CI = -0.018 to 0.363). Similarly, the correlation
Table 2.
Pearson x2 Test for AHI Classification and Presence or
Absence of Moderate/Severe Periodontitis
Periodontal Disease (moderate/severe)
AHI Classification No Yes Total
Normal 11 (42.3%) 15 (57.7%) 26 (100.0%)
Mild 5 (23.8%) 16 (76.2%) 21 (100.0%)
Moderate 6 (31.6%) 13 (68.4%) 19 (100.0%)
Severe 5 (14.7%) 29 (85.3%) 34 (100.0%)
Total 27 (27.0%) 73 (73.0%) 100 (100.0%)
P = 0.111.
¶ SPSS v.20.0, IBM, Chicago, IL.
J Periodontol • February 2015 Loke, Girvan, Ingmundson, Verrett, Schoolfield, Mealey
235
5. between AHI classification and age was negligible
(r = 0.276, 95% CI = 0.084 to 0.448), and the AHI
classification with BMI correlation was small (r =
0.300, 95% CI = 0.110 to 0.468).
Association Between AHI (Absolute) and
Periodontal Disease
The relation between AHI and periodontal disease
was also examined using absolute AHI values as a
continuous variable. When AHI was expressed as a
continuous variable, there were negligible correla-
tions between AHI and periodontal disease severity
classification (r = 0.191, 95% CI = -0.006 to 0.373)
and between AHI and age (r = 0.273, 95% CI =
0.081 to 0.446), whereas a small correlation was
observed between AHI and BMI (r = 0.342, 95%
CI = 0.156 to 0.505).
Association Between AHI and Periodontal
Disease (Box Plot Analysis and ANCOVA)
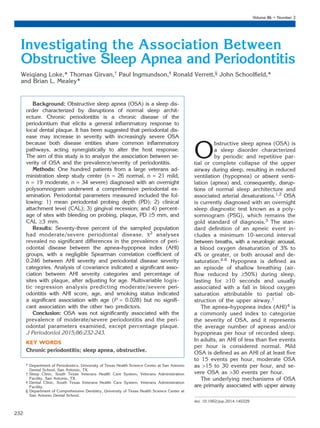
Box plot analysis was performed to evaluate the
relation between AHI classification and periodontal
parameters (Fig. 1). The box plot analysis provided
a visual assessment of the medians, 25th to 75th
interquartile range, minimum and maximum values,
and the outliers. Percentage plaque proved to
be the only clinical periodontal parameter that
had a statistically significant relation with AHI
classification.
Because box plot analyses demonstrated a sig-
nificant relation with percentage plaque and sug-
gested a possible relation with percentage BOP and
percentage CAL ‡3 mm with AHI classification, these
relations were further evaluated by ANCOVA (Table 3).
The significant relation between AHI class and per-
centage plaque was confirmed by ANCOVA (P = 0.037),
with the age-adjusted severe group mean significantly
greater than the age-adjusted mild group mean
(mean difference of 21.7%, 95% CI = 7.0% to 36.3%,
P = 0.004). The age covariate was also significantly
associated with percentage plaque (P = 0.001).
However, ANCOVA revealed no significant relation
between AHI class and percentage BOP (P = 0.126)
or percentage sites with CAL ‡3 mm (P = 0.842).
The age covariate was significantly associated with
Figure 1.
Box plot analysis of AHI category and periodontal variables. A) Mean PD. B) Mean REC. C) Mean
CAL. D) Percentage of sites with BOP. E) Percentage of sites with plaque. F) Percentage of sites with
PD ‡5 mm. G) Percentage of sites with CAL ‡3 mm. Open circles indicate mild outliers; asterisks
indicate extreme outliers.
Obstructive Sleep Apnea and Periodontitis Volume 86 • Number 2
236
6. percentage BOP (P = 0.025) but not significantly
associated with percentage CAL ‡3 mm (P = 0.266).
Analyzing Periodontal Disease as a Categorical
Variable
The relation between periodontitis classification as
a categorical variable (ADA/CDC mild, moderate,
or severe) and other patient-level variables was
analyzed separately using Fisher exact tests. The
analysis showed no statistically significant relation
between periodontitis classification and ethnicity
(P = 0.086) or sex (P = 0.902). However, periodontal
classification was significantly related to diabetes
(P <0.001) and smoking history (P = 0.042). As dis-
cussed above, Spearman correlation analysis also
revealed a small correlation between periodontal
disease classification and age (r = 0.317, 95% CI =
0.128 to 0.483), whereas the correlation with BMI
(r = 0.179, 95% CI = -0.018 to 0.363) was negligible.
Multivariable Logistic Regression
Multivariable logistic regression analysis was used to
explore the relation between the prevalence of
moderate/severe periodontitis and AHI. For logistic
regression, AHI absolute values were
divided into 10-unit increments, and
age was divided into 10-year in-
crements. Given the fact that there
were only 27 patients who did not
have moderate/severe periodontitis,
the sample had sufficient power to
include up to three predictors in the
model. Other demographic variables
considered for inclusion were di-
abetes and smoking history. How-
ever, because the average age for
patients with diabetes was 12.7
years older than the average age for
those without diabetes, these mea-
sures were significantly associated,
whereas no such association was
found between age and smoking
history. Thus, the three-predictor
model included the continuous
measures of AHI and age and the categorical co-
variate of smoking history, with non-smoker as the
reference group (Table 4). The Hosmer-Lemeshow
goodness-of-fit test had P = 0.749, so the model
was valid. The resulting periodontal disease severity
odds ratio (OR) for 10-unit AHI was not statistically
significant (OR = 1.04, 95% CI = 0.88 to 1.23, P =
0.615), nor was the OR of former smokers to non-
smokers (OR = 3.49, 95% CI = 0.92 to 13.3, P =
0.067). Conversely, the 10-year increment age OR
was significant (OR = 1.52, 95% CI = 1.05 to 2.22,
P = 0.028), indicating a significant relation between
age and diagnosis of moderate/ severe peri-
odontitis.
DISCUSSION
The main objective of this study is to analyze the
relation between OSA and periodontal disease prev-
alence and severity using a variety of clinical param-
eters. The association between OSA and periodontal
disease has been suggested by previous cross-
sectional studies20,31-33 to have an OR of between
1.75 and 1.84.31 Furthermore, a dose–response
relation has been proposed32 (i.e., higher AHI may
be associated with increased odds for periodontitis).
The current study set out to examine dose–response
relations by stratifying the OSA population into three
categories of severity (AHI: mild, moderate, and
severe) along with a control group without OSA. All
the patients, who were consecutively recruited at a
VA hospital sleep center, were newly diagnosed and
had no previous treatment for their sleep condition
of OSA.
Strict inclusion criteria excluded possible con-
founders such as current smokers, patients with
poorly controlled diabetes, other poorly controlled
Table 3.
ANCOVA of Percentage of Sites With BOP, Percentage
of Sites With Plaque, and Percentage of Sites With
CAL >3 mm (means unadjusted for the age covariate)
AHI Class n
Percentage
BOP – SD*
Percentage
Plaque – SD†
Percentage of Sites with
CAL ‡3 mm – SD‡
Normal 26 13.1 – 12.4 34.0 – 27.6 42.5 – 20.7
Mild 21 11.3 – 9.4 31.5 – 20.5 44.4 – 23.7
Moderate 19 14.9 – 9.0 47.2 – 28.7 44.0 – 27.8
Severe 34 19.8 – 19.0 52.3 – 31.5 48.4 – 22.6
Total 100 15.3 – 14.2 42.2 – 29.0 45.2 – 23.2
* Percentage BOP: F = 1.952; P = 0.126
† Percentage plaque: F = 2.938; P = 0.037
‡ Percentage of sites with CAL ‡3 mm: F = 0.276; P = 0.842
Table 4.
Logistic Regression Model for Periodontal
Disease Prevalence and AHI
Variable OR 95% CI P
AHI 10-unit increments 1.044 0.883 to 1.234 0.615
Age 10-year increments 1.523 1.047 to 2.216 0.028
Smoking history (yes/no) 3.492 0.918 to 13.279 0.067
J Periodontol • February 2015 Loke, Girvan, Ingmundson, Verrett, Schoolfield, Mealey
237
7. systemic diseases (ASA Class greater than II), and
pregnant or lactating females, thus providing a
study sample with the least amount of patient-
centered confounders. The examiner was masked
and performed the periodontal examination on patients
before their PSG sleep study, therefore limiting the
effect of examiner bias.
The sample size was calculated based on the
required number of patients per group to reject the
null hypothesis of equal group means using one-
way ANOVA at the 0.05 significance level with 90%
power with an effect size defined by a clinically sig-
nificant mean difference of one common standard
deviation being present for the sample population
between the control group and at least one of the
OSA severity groups. The final enrolled sample of
100 patients provided the required effect size, as-
suming a population prevalence of periodontitis similar
to that seen in studies of the United States pop-
ulation.28,29 Although this sample size was smaller
than some other studies,31-33 the study used AHI scores
and analyzed them as both categorical variables
(i.e., mild OSA [AHI of at least five to 15 per hour],
moderate OSA [AHI >15 to 30 per hour], and severe
OSA [AHI >30 per hour]) and as continuous vari-
ables based on the absolute AHI values. Because
the prevalence of moderate/severe periodontitis
was higher in this study population than originally
expected, a post hoc power analysis was performed
to determine the sample size needed to detect
significant AHI group differences in percentages for
moderate/severe periodontitis for a population with
a very high prevalence of moderate/severe disease.
The sample size would need to be doubled in such
a population (n = 200) to attain a sample size
sufficient to detect AHI group differences by x2 test
at the 0.05 level with power of 84%.
This study found no meaningful association be-
tween OSA and the prevalence of moderate/severe
periodontitis. Furthermore, there was a negligible
correlation between AHI severity and periodontal
disease severity categories. It is concluded that the
relation between the severity of OSA and periodontal
status, if any, was weak in this specific patient pop-
ulation. Caution should be exercised when extrap-
olating the results of this study to the general
population because the high prevalence of peri-
odontitis recorded in this study differs from the
prevalence found in the United States population as
a whole.28,29 The high percentage of patients with
moderate/severe periodontitis makes evaluation of
differences in AHI severity among groups with no,
mild, moderate and, severe periodontitis more dif-
ficult. However, this patient population was selected
from consecutively treated VA sleep center patients,
without regard to their periodontal status, and peri-
odontal examination was performed before the PSG
study. Future studies should evaluate larger sleep
study patient populations to provide a greater
number of patients with little or no periodontitis. A
summary of the various study designs, definitions,
and limitations of the previous studies are found in
Table 5.
The findings of this study are in disagreement
with previous studies that examined the relation
between OSA and periodontal disease.20,31-33 The
difference in study outcomes has several possible
explanations. First, this study used six-point com-
prehensive full-mouth periodontal examination on
all teeth. One of the other studies32 used partial-mouth
charting, which may lead to an underestimation of
the prevalence of periodontal disease. Second, the
definitions of periodontal disease used in the pre-
vious studies were different from the current study.
Some of the definitions may have underestimated32
the prevalence of periodontal disease and others
may have overestimated31 the prevalence of peri-
odontal disease relative to the AAP/CDC definition
used in this study.28 Third, the clinical diagnosis of
OSA in one of the previous studies33 did not use the
PSG sleep test; instead, a questionnaire meant for
screening patients undergoing general anesthesia
was used. Fourth, most of the previous studies col-
lapsed all the OSA groups into a dichotomous
definition of presence or absence of sleep apnea,10
had a stratification of three OSA groups (less than
5, 5 to 10, and >10 events per hour),32 or obtained
the diagnosis from International Classification of
Diseases, Ninth Revision (ICD-9) databases.31 This
may mask the inherent differences in prevalence of
periodontal disease based on the AHI-defined se-
verity groups from detection. The current study pro-
vides the most rigorous OSA classification of any
study published to date, using the currently accepted
stratification of the AHI groups into non-OSA (AHI
of less than five per hour), mild OSA (AHI of at least
five to 15 per hour), moderate OSA (AHI >15 to 30
per hour), and severe OSA (AHI >30 per hour).4
Finally, some studies20,31 examined the periodontal
status of OSA patients only, comparing the prev-
alence of periodontitis in the OSA study population
with that found in populations outside the study
group, such as national demographic dental data-
bases20 or insurance databases.31 The current study
examined both OSA and non-OSA patients, newly
diagnosed with a PSG gold-standard test within the
VA-eligible population.
In other studies demonstrating an association be-
tween OSA and periodontal disease, the associa-
tion measured by OR was relatively weak (1.75
to 1.84).31,32 In the current study, the OR for AHI
and prevalence of periodontitis was not statistically
Obstructive Sleep Apnea and Periodontitis Volume 86 • Number 2
238
11. significant (OR = 1.057, 95% CI = 0.896 to 1.248;
P = 0.511) and, coupled with the negligible corre-
lation between AHI and periodontal disease severity
categories, suggests that there is no dose–response
relation between AHI severity and prevalence of
periodontitis. This was confirmed statistically when
AHI was expressed as an absolute value and treated
as a continuous variable (r = 0.191, 95% CI = -0.006
to 0.373). In addition, the clinical parameters providing
information on periodontitis severity and extent—mean
PD, mean CAL, percentage of sites with CAL ‡3 mm,
and percentage of sites with PD ‡5 mm—were not
significantly correlated with AHI severity.
CONCLUSIONS
In conclusion, this is the first cross-sectional study
showing that OSA, when defined in AHI severity
categories, is not significantly associated with the
prevalence of periodontitis in this specific VA pop-
ulation. Furthermore, none of the clinical periodontal
parameters except percentage plaque were signifi-
cantly related to severity of OSA. In addition, when
AHI was expressed in absolute values, there was no
correlation with any periodontal parameters measured.
ACKNOWLEDGMENTS
The authors thank sleep technicians Amy McHenry
and Larry Tho for their support in the recruitment of
patients at the Audie L. Murphy Memorial Sleep
Laboratory. The authors report no conflicts of interest
related to this study.
REFERENCES
1. Medicine AAoS. Obstructive sleep apnea syndrome.
In: The International Classification of Sleep Disorders
Revised Diagnostic and Coding Manual; 2001:52-58.
2. Duchna HW. Sleep-related breathing disorders — A
second edition of the International Classification of
Sleep Disorders (ICSD-2) of the American Academy
of Sleep Medicine (AASM) (in German). Pneumologie
2006;60:568-575.
3. Epstein LJ, Kristo D, Strollo PJ Jr., et al; Adult Obstruc-
tive Sleep Apnea Task Force of the American Academy
of Sleep Medicine. Clinical guideline for the evaluation,
management and long-term care of obstructive sleep
apnea in adults. J Clin Sleep Med 2009;5:263-276.
4. [no authors listed]. Sleep-related breathing disorders in
adults: Recommendations for syndrome definition and
measurement techniques in clinical research. The Re-
port of an American Academy of Sleep Medicine Task
Force. Sleep 1999;22:667-689.
5. Redline S, Budhiraja R, Kapur V, et al. The scoring of
respiratory events in sleep: Reliability and validity.
J Clin Sleep Med 2007;3:169-200.
6. Iber CA, Chesson AL, Quan SF. The AASM Manual for
the Scoring of Sleep and Associated Events: Rules,
Terminology, and Technical Specifications. Westches-
ter, IL: American Academy of Sleep Medicine; 2007.
7. Eckert DJ, Malhotra A, Jordan AS. Mechanisms of
apnea. Prog Cardiovasc Dis 2009;51:313-323.
8. Antonopoulou S, Loukides S, Papatheodorou G,
Roussos C, Alchanatis M. Airway inflammation in
obstructive sleep apnea: Is leptin the missing link?
Respir Med 2008;102:1399-1405.
9. Burioka N, Koyanagi S, Endo M, et al. Clock gene
dysfunction in patients with obstructive sleep apnoea
syndrome. Eur Respir J 2008;32:105-112.
10. [no authors listed]. Even mild sleep apnea increases
heart risk. Research shows that minimally symptom-
atic obstructive sleep apnea can increase arterial
stiffness. Heart Advis 2009;12:4.
11. Arter JL, Chi DS, Girish M, Fitzgerald SM, Guha B,
Krishnaswamy G. Obstructive sleep apnea, inflamma-
tion, and cardiopulmonary disease. Front Biosci 2004;
9:2892-2900.
12. Atkeson A, Jelic S. Mechanisms of endothelial dys-
function in obstructive sleep apnea. Vasc Health Risk
Manag 2008;4:1327-1335.
13. Alam I, Lewis K, Stephens JW, Baxter JN. Obesity,
metabolic syndrome and sleep apnoea: All pro-
inflammatory states. Obes Rev 2007;8:119-127.
14. Abad VC,Guilleminault C.Treatment optionsforobstructive
sleep apnea. Curr Treat Options Neurol 2009;11:358-367.
15. Owens RL, Eckert DJ, Yeh SY, Malhotra A. Upper
airway function in the pathogenesis of obstructive sleep
apnea: A review of the current literature. Curr Opin
Pulm Med 2008;14:519-524.
16. Schenkein HA, Loos BG. Inflammatory mechanisms
linking periodontal diseases to cardiovascular diseases.
J Periodontol 2013;84(Suppl. 4):S51-S69.
17. Buhlin K, Hultin M, Norderyd O, et al. Risk factors for
atherosclerosis in cases with severe periodontitis. J Clin
Periodontol 2009;36:541-549.
18. Ebersole JL, Machen RL, Steffen MJ, Willmann DE.
Systemic acute-phase reactants, C-reactive protein
and haptoglobin, in adult periodontitis. Clin Exp Im-
munol 1997;107:347-352.
19. Ebersole JL, Cappelli D, Mathys EC, et al. Periodontitis
in humans and non-human primates: Oral-systemic
linkage inducing acute phase proteins. Ann Periodon-
tol 2002;7:102-111.
20. Gunaratnam K, Taylor B, Curtis B, Cistulli P. Obstruc-
tive sleep apnoea and periodontitis: A novel associa-
tion? Sleep Breath 2009;13:233-239.
21. Blum A, Front E, Peleg A. Periodontal care may improve
systemic inflammation. Clin Invest Med 2007;30:
E114-E117.
22. Vidal F, Figueredo CM, Cordovil I, Fischer RG. Peri-
odontal therapy reduces plasma levels of interleukin-
6, C-reactive protein, and fibrinogen in patients with
severe periodontitis and refractory arterial hyperten-
sion. J Periodontol 2009;80:786-791.
23. Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemi-
ology of obstructive sleep apnea: A population-based
perspective. Expert Rev Respir Med 2008;2:349-364.
24. Young T, Peppard PE, Gottlieb DJ. Epidemiology of
obstructive sleep apnea: A population health perspec-
tive. Am J Respir Crit Care Med 2002;165:1217-1239.
25. Young T, Palta M, Dempsey J, Skatrud J, Weber S,
Badr S. The occurrence of sleep-disordered breathing
among middle-aged adults. N Engl J Med 1993;328:
1230-1235.
26. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of
sleep-disordered breathing in women: Effects of gen-
der. Am J Respir Crit Care Med 2001;163:608-613.
27. Dura´n J, Esnaola S, Rubio R, Iztueta A. Obstructive
sleep apnea-hypopnea and related clinical features in
Obstructive Sleep Apnea and Periodontitis Volume 86 • Number 2
242
12. a population-based sample of subjects aged 30 to 70
yr. Am J Respir Crit Care Med 2001;163:685-689.
28. Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ;
CDC Periodontal Disease Surveillance workgroup:
James Beck (University of North Carolina, Chapel Hill,
USA), Gordon Douglass (Past President, American
Academy of Periodontology), Roy Page (University
of Washin. Prevalence of periodontitis in adults in the United
States: 2009 and 2010. J Dent Res 2012;91:914-920.
29. Eke PI, Thornton-Evans G, Dye B, Genco R. Advances
in surveillance of periodontitis: The Centers for Disease
Control and Prevention periodontal disease surveil-
lance project. J Periodontol 2012;83:1337-1342.
30. Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for
the Behavioral Sciences. Boston: Houghton Mifflin; 2003:
95-120.
31. Keller JJ, Wu CS, Chen YH, Lin HC. Association
between obstructive sleep apnoea and chronic peri-
odontitis: A population-based study. J Clin Periodontol
2013;40:111-117.
32. Seo WH, Cho ER, Thomas RJ, et al. The association
between periodontitis and obstructive sleep apnea: a
preliminary study. J Periodontal Res 2013;48:500-506.
33. Ahmad NE, Sanders AE, Sheats R, Brame JL, Essick
GK. Obstructive sleep apnea in association with peri-
odontitis: A case-control study. J Dent Hyg 2013;87:
188-199.
Correspondence: Dr. Brian L. Mealey, University of Texas
Health Science Center at San Antonio, Department of
Periodontics, MSC 7894, 7703 Floyd Curl Dr., San
Antonio, TX 78229-3900. Fax: 210/567-3761; e-mail:
mealey@uthscsa.edu.
Submitted April 16, 2014; accepted for publication
September 3, 2014.
J Periodontol • February 2015 Loke, Girvan, Ingmundson, Verrett, Schoolfield, Mealey
243