1. Case Study: Fetus Papyraceus
Kristen Kirsch; Walt Bugielski, PA (ASCP); Pradeep Sethi, MD; Michelle Costas, PA (ASCP); Justin Falcon, PA (ASCP)
Allegheny General Hospital – Pittsburgh, PA
CLINICAL BACKGROUND:
GROSS FINDINGS:
CONCLUSIONS:
References:
1. Kalousek, D.K, Fitch, N, Paradice, B.A. Pathology of the Human Embryo and Previable Fetus – An Atlas. New York, NY: Springer-Verlag; 1990.
2. Saul, R.A, Stevenson, R.E, Rogers, R.C, Skinner, S.A, Prouty, L.A, Flannery, D.B. Growth References From Conception To Adulthood. Supplement
Number 1. Greenwood, SC: Greenwood Genetic Center; 1988.
3. Benirschke, K, Burton, G.J, Baergen, R.N. Pathology of the Human Placenta. Berlin, Germany: Springer-Verlag; 2012.
4. Baldwin, V.J. Pathology of Multiple Pregnancy. New ork, NY: Springer-Verlag; 1994.
5. Kumar, V, Abbas, A, Aster, J. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Philadelphia, PA: Elsevier Saunders; 2015.
DISCUSSION:
Fetus papyraceus (also recently known as vanishing twin phenomenon) is a
condition in which there is a compressed, flattened, involuted twin fetus and the
surviving twin develops normally. This usually occurs in the second trimester with the
co-twin being delivered in the third trimester. The fetus must die in the twelve to
twenty week period but must be delivered after twenty weeks. It becomes
compressed to fetal papyraceus by the growing sac of the living twin as the fluid of its
own amniotic sac is resorbed. Monochorionic and fused dichorionic twins can present
with this condition; the fetus can be found within the placental membranes.
The twin that survives can have anomalies as well. These consist of ileal atresia,
congenital skin defects, limb amputations and gastroschisis. The mechanism of these
complications is unknown. The umbilical cord around the leg of the monoamniotic twin
can result in in amputation of the leg. Transamniotic vascular complications can result
in disseminated intravascular coagulopathy following the death of the co-twin4.
Studies have shown that the surviving twin can develop normally.
The deceased twin can have various amounts of compression. Normally they are
tan-gray with extensive tissue autolysis. Cause of death is difficult to determine in
these cases; this may be due to to anomalous cord insertion (i.e. velamentous),
severe twin-twin transfusion syndrome (vascular anastomoses) or cord
entanglements. The thorax is flattened and the entire surface is gray-yellow, slightly
dry. The epidermis shrinks to a single layer which may represent remnants of the
basement membrane. No bloating or swelling is grossly identified. The liver appears
as a mass of yellow material inferior to the diaphragm. Male fetuses are more affected
than female fetuses. The placental features are due to cessation of fetal circulation in
that portion of the placenta associated with the deceased twin. Thus, this leads to
gradual reduction of maternal circulation to that villous area which leads to ischemic
damage and eventual collapse of villi. The compaction is associated with increased
fibrin deposition around the villi.
When the fetus dies, the mother may experience amniotic fluid leaks, sudden
lower abdominal pain and vaginal bleeding. There may be a period of rapid uterine
growth then followed by a slowed or normal growth pattern.
In this case, composite gestational age was determined using tables and graphs
provided using both long bone measurements and presence of ossification centers.
During the process of embryogenesis, bones develop from cartilage molds which are
created from mesenchymal precursor cells. Primary ossification centers located in the
diaphysis, which provide radial bone growth, appear during gestational weeks 7 to 12
in the long bones. These are the areas of bone that ossify first; the clavicle and
mandible are first to ossify. Secondary ossification centers occur when endochondral
ossification progresses away from the center of the bone. The cartilage that becomes
trapped between these two centers is known as the growth plate. In this case,
ossification centers were found at the terminal fifth phalange of the foot and the fifth
middle phalanx of the hand; this corresponds to a approximate gestational age of at
least 12 weeks.
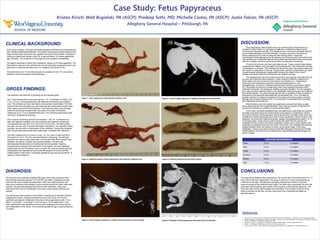
Figure 1. Fetus papyraceus with attached umbilical cord.
Figure 2. Opposing aspect of fetus papyraceus with attached umbilical cord.
Figure 4. X-ray of longer exposure to display phalanges of hands and feet.
Figure 3. X-Ray image to display rib, vertebra and long bones of arms and legs.
Figure 5. Infarcted placenta post-formalin-fixation.
In the case reviewed, a 28-year-old female presented with severe pre-eclampsia and
diet maintained gestational diabetes. The patient had previous prenatal ultrasound to
diagnose diamniotic-dichorionic twin gestation during the first trimester. Subsequent
ultrasound determined demise of twin “B” at approximately 13.5 weeks gestational
age (clinically). The remainder of the pregnancy was reported unremarkable.
The patient presented to West Penn Hospital for delivery at 37 weeks gestation. The
fetus failed to descend and a primary low cervical transverse caesarean section was
performed. A viable female infant (twin “A”) weighed 2730 grams (6 lbs.).
The placenta for twin “A” and the products of conception for twin “B” were sent to
Allegheny General Hospital surgical pathology.
The specimen was received in pathology as two separate parts.
Part 1 was the placenta for the surviving twin – “A”. It consisted of a 592g , 19.0
x 15.3 x 3.2 cm, ovoid placental disc with attached membranes and umbilical
cord. The umbilical cord and membranes were grossly unremarkable. The fetal
surface of the disc was glistening, pale blue-gray with peripherally located areas
of tan-yellow subchorionic fibrin deposits. The maternal surface was complete,
intact and sectioning revealed three, tan-yellow, firm areas of induration
measuring up to 1.5 cm in greatest dimension. The remaining parenchyma was
red-brown, congested and spongy.
Part 2 was the remaining products of conception – twin “B”. It consisted of a
fetus with attached umbilical cord and a placenta with attached membranes.
The placental disc was 50g, 10.0 x 8.0 x 0.5 cm and ovoid. The fetal surface
was pale, tan-pink with no grossly identifiable vasculature. The maternal surface
was pale, tan-pink with no demarcation of the cotyledons. Sectioning revealsed
pale, tan-pink parenchyma with gray-white areas, consistent with infarctions.
The fetus measured 9.2 cm crown to rump, 12.7 cm crown to heel and had a
foot length of 1.2 cm. The skin was dessicated and sloughing. The attached
umbilical cord was severely dessicated, red-pink and three blood vessels were
identified. No cleft lip or palate were grossly identified. The fetus was
phenotypically female based on external and internal genitalia. Opening
revealed severe autolysis and desiccation of the organs; the heart appeared
anatomically normal; the kidneys were not cystic; the lungs had ribbed grooves.
Ossifications were identified at the terminal fifth phalanx of the foot and fifth
middle phalanx of the hands. Composite gestational age was appropriate for 14
weeks on growth patterns.
LONG BONE MEASUREMENTS
Femur 1.6 cm ~14 weeks
Tibia 1.4 cm ~14 weeks
Fibula 1.5 cm ~14 weeks
Humerus 1.8 cm ~14 weeks
Radius 1.6 cm ~15 weeks
Ulna 1.7 cm ~14 weeks
DIAGNOSIS:
The first part was a placenta weighing 592 grams which was consistent with a
third trimester placenta (between 10th and 50th percentile). It displayed mature
chorionic villi and increased syncytial knots. There was reactive amnion and
meconium-containing macrophages. Acute chorioamnionitis and focal villitis were
present. The placenta displayed subchorionic fibrin deposition, infarct and
intervillous fibrin thrombi. Additionally, there was a three-vessel umbilical cord
present.
The second part were products of conception consisting of an infarcted placenta
weighing 50.0 grams, autolyzed membranes and cords. Acute and chronic
deciduitis was present. Additionally, there was a fetus papyraceous with 1.6 cm
femur, 1.4 cm tibia, 1.5 cm fibula, 1.8 cm humerus, 1.6 cm radius and 1.7 cm
ulna. Ossifications were identified at the terminal phalangeal of the foot and the
first metaphalanx of the hands. The composite gestational age is approximated at
14 weeks.
Figure 6. Example of fetus papyraceus dissected from the placenta.3
This case demonstrated a fetus papyraceus. The overall rate of this phenomenon is 1 in
every 180 to 190 twin pregnancies. The cause is unknown in most circumstances as
confirmed in this case. The placenta was highly infarcted as it seems to not have
received enough of the maternal blood supply. The fetus was compressed; the skin was
desiccated and sloughing upon receipt of the specimen confirming this diagnosis. The
heart was intact and no abnormalities were identified. The condition of the surviving
infant is unknown at this time, but she could have a list of potential anomalies as
described above.