
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pleurisy
Similar to Pleurisy (20)
Recently uploaded
Recently uploaded (20)
Pleurisy
- 1. Pleurisy Koumail Yassine Group 8 4th dozen
- 2. Physiology of the Normal Lungs • The lungs are soft, spongy, cone-shaped organs located in the chest cavity. • They are Separated by the mediastinum and the heart. There are 3 lobes on the right lung and 2 lobes on the left lung.
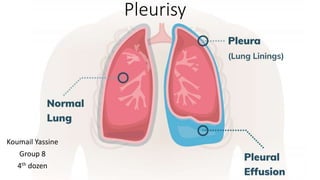
- 3. Layers of the lung pleura • Parietal Pleura -Lines the thoracic cavity, including the thoracic cage, mediastinum, and diaphragm. • Pleural Space- thin, transparent, serous membrane which lines the thoracic cavity a potential space between the parietal pleura and • Visceral pleura- Lines the entire surface of the lung.
- 4. Normal vs impaired physiology • The body produces pleural fluid in small amounts to lubricate the surfaces of the pleura, it lines the chest cavity and surrounds the lungs. The pleural cavity contains a relatively small amount of fluid, approximately 10 ml on each side • A pleural effusion is an abnormal, excessive collection of this fluid . • Excessive amounts of such fluid can impair breathing by limiting the expansion of the lungs during inspiration causing a stabbing pain in the chest. • This is pleurisy!
- 6. The syndrome of accumulation of fluid in the pleural cavity • severity of symptoms depends on the amount of exudate! • bulging of intercostal spaces behind the affected side during dynamic examination • reduced of the mobility of the lower pulmonary region on the affected side • changed borders of the relative cardiac dullness • the lack of voice tremor above the accumulation of fluid; • dullness over the place of accumulation of fluid • vesicular breathing does not auscultate • bronchophony is weakened
- 7. Radiological findings blunting of the costophrenic angle blunting of the cardiophrenic angle fluid within the horizontal or oblique fissures
- 8. Other scans Ultrasound: is useful both as a diagnostic tool and as an aid in performing thoracentesis. It assists in identifying pleural fluid locations. CT-scan: t helps distinguish anatomic compartment more clearly. This modality is useful as well in distinguishing empyema
- 9. Pain syndrome • complaints of pain in the chest • knife-stabbing pain- forced position of the body • tenderness (painful palpation of thorax).
- 10. Other syndromes Syndrome of local inflammation: cough with phlegm (mucus or muco purulent); Syndrome of general inflammation: - fever (and the associated with it complaints of a general nature); - changes in the blood count ( leukocytosis, accelerated erythrocyte sedimentation rate). Respiratory failure syndrome: - shortness of breath; - cyanosis; - tachypnea; - decrease in the partial pressure of oxygen; - decrease in oxygen saturation.
- 12. Dry vs Wet pleurisy • Wet: increased pleural fluid which compresses the lung • Dry: decreased pleural fluid to the point where the layers rub together
- 13. Transudative vs Exudative pleural effusion
- 16. On Type of Exudate • Serous and serofibrinous pleurisy (tuberculosis in 70 to 90 percent of cases, pneumonia, certain infections, and also rheumatism in 10 to 30 percent of cases) • Purulent process (pneumococci, streptococci, staphylococci, and other microbes) • Hemorrhagic pleurisy (tuberculosis of the pleura, bronchogenic cancer of the lung with involvement of the pleura, and also in injuries to the chest
- 18. Treatment
- 19. • treatment aims to: 1) Remove the fluid and prevent fluid from building up again, and 2) Treating the cause of the fluid buildup • Therapeutic thoracentesis: may be done if the fluid collection is large and causing chest pressure, shortness of breath, or other breathing problems, such as low oxygen level. Removing the fluid allows the lung to expand, making breathing easier • pleural effusions caused by congestive heart failure are treated with diuretics and other medication that treat heart failure • Pleural effusions caused by infection are treated with appropriate antibiotics after Gram stain and culture to identify possible bacterial infections • Cytopathology to identify cancer cell, and Treat accordingly.
- 20. Possible complications More often pleurisy is itself the complication of another pathologic process Pleural fluid that becomes infected may turn into an abscess, called an empyema, which will need to be drained with a chest tube Pneumothorax (air in the chest cavity) can be a complication of the thoracentesis procedure
- 21. References • a Putnam 8. Malignant pleural effusions. Surg Clin NAm.2OO2;38375- 383. • B. Víllena v, López Encuentra E, García-Luján R, Clinical implications of appearance of pleural fluid at thoracentesis.Chest.2OO4;I25:I56-9. • D. villena garrido v et al. diagnosis and treatment of pleural effusion(2oo5}
- 22. Thank You