
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (19)
Similar to PT Interventions for Diabetic Neuropathy
Similar to PT Interventions for Diabetic Neuropathy (20)
PT Interventions for Diabetic Neuropathy
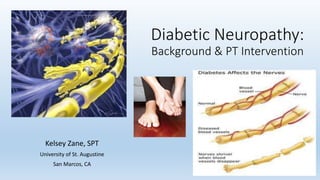
- 1. Diabetic Neuropathy: Background & PT Intervention Kelsey Zane, SPT University of St. Augustine San Marcos, CA
- 2. Overview of Diabetes Mellitus • Diabetes is a common co- morbidity among many Americans today. • Definition: chronic disease characterized by abnormal use of insulin and elevated blood glucose levels.8 • Associated complications: hyper/hypoglycemia, glycosuria, ketoacidosis, coma, ischemia, atherosclerosis, amputation, poor healing, HTN, MI, CVA, kidney disease, peripheral neuropathies and death. Common Types of Diabetes Mellitus Type I (Insulin Dependent) Type II (Non-insulin Dependent) o severe deficiency of insulin o usually present in youth o without insulin, patients develop ketoacidosis* *definition: when sugar is not able to utilized and instead the body breaks down muscle and fat for energy. o presents later in life & usually overweight o glucose enters cell in adequate amounts o extracellular glucose is elevated o do not usually become ketotic
- 3. A striking statistic: "Diabetic polyneuropathy is one of the most common long-term complications affecting around 50% of all people [with type II diabetes mellitus].”8 Tesfaye, S., Boulton, A., Dyck, P. et al. Diabetes Care 2010.
- 5. Overview of Diabetic Neuropathy: • Dependent Sensorimotor Polyneuropathy (DSPN): It is chronic, symmetrical and length dependent. • This most often develops with patients who has a background of long standing hyperglycemia, other metabolic abnormalities and cardiovascular risk factors.8 • Diabetic Autonomic Neuropathy (DAN): disorder of the autonomic nervous system in the setting of diabetes or pre-diabetic metabolic derangements (after the exclusion of other pathologies). • Effect on body systems is variable, including the cardiovascular, gastrointestinal, urogenital and sudomotor systems. • What this means to healthcare professionals:8 • Cardiovascular system: unexplained tachycardia, orthostatic hypotension, poor exercise tolerance Therapy: monitor vitals during treatment, setting realistic goals, breathing techniques • Gastrointestinal system: Impaired oral drug absorption, malnutrition, poor quality of life Therapy: timing of treatment to ensure participation • Urogenital: Severe incontinence Therapy: including pelvic floor exercises • Sudomotor: Foot dryness increasing risk of foot ulceration Therapy: foot hygiene instruction and proper footwear choice
- 7. Interdisciplinary communication In order to provide comprehensive care for our patients other healthcare providers on our team include: • Physician • Nursing • Neurologist* • Dietician/Nutritionist* • Podiatrist*
- 8. Screening tools for sensation loss • Semmes-Weinstein monofilament & tuning fork testing: • Study by Perkins et al: identified a baseline for monofilament score that predicts the probability of a patient developing diabetic neuropathy in the next 4 years. • Score: < 5/8 • Excellent inter- and intrarelater reproducibility using specific protocol
- 9. Semmes-Weinstein protocol4 • 10 g Monofilament procedure: • Apply a reference stimuli to the forehead or sternum. • With patients eyes closed apply a stimuli to a non callused area of the dorsum of the great toe just proximal to the nailbed in a smooth motion. • The skin was touched and the monofilament bent for a full second then lifted from the skin. • This was repeated 4 times per foot in a random manner. • Scoring: results are tallied and then applied to a 1-8 scale. • Normal = 1 point assigned • Decreased = 0.5 points assigned • Absent = 0 points assigned
- 10. 128 Hz Tuning fork protocol4: • Strike the tuning fork hard enough so it will vibrate for approximately 40 seconds. • Apply base of tuning fork to the patients forehead or sternum and ensure the vibration sensation is understood. • Ask the patient to close their eyes then apply the tuning fork to the bony prominence at the dorsum of the first toe just proximal to the nailbed. • Ask if the vibration sensation is perceived. Then ask when the vibration sensation has stopped. • One point is given for if the vibration if the sensation is correctly perceived as "on". Another point is assigned if the correct timing of dampening of the vibration is perceived or "off". • Repeat this procedure again on the same foot then twice on the other foot in a random manner.
- 11. Neuromuscular Re-education Therapeutic Exercise Gait Training Modalities Effective Interventions to Improve Functional Mobility in Diabetic Neuropathy Patients
- 12. Therapeutic Exercises: Sartor et al 2012: • Focused on stretching, strengthening and functional foot/ankle exercise to improve foot rollover. • Prescription: 2x/wk for 12 wks at 40-60 min a session • 4 areas that were included: increase in foot/ankle ROM, strengthen foot/ankle muscles, functional exercises, walking skills & foot rollover training • Outcome: Improvement was modest but plant pressure re-distribution did occur in experimental group. Overall the patients demonstrated an improved dynamic loading pattern.7 • Application: Essential principles of therapeutic exercise including techniques to improve weight bearing during mobility and exercises to increase strength can be beneficial for patients with diabetic neuropathy. See attached example of the specific protocol used in this study.
- 13. Neuromuscular Re-education • Various studies have focused on the importance of balance training in this population: • Progressive balance training in the anterior-posterior direction and decreasing reliance on visual feedback increased dynamic stability.1,6 • Furthermore other research supports training in ankle strategies during standing dynamic balance to improve functional mobility and reduce exploratory postural sway.5,6
- 14. Pre gait & Gait Training: • Amemiya et al identified a link between an increase in plantar foot pressure and increased incidence in diabetic foot ulcers. • Outcome: Diabetic patients demonstrated decreased motion during the mid-stance phase which could be improved with increasing ankle ROM and sensory feedback. • Application: Joint mobilization and pre-gait training with emphasis on ankle rollover are appropriate interventions.
- 15. Modalities to Improve Sensation: • Low level TENS can be used in conjunction with other interventions to increase sensory feedback3. The protocol consisted of: • 6 weeks of treatment at 5 times a week. • patients sat for 30 min. in a foot bath w/electrodes • TENS delivered 120-Hz pulsed current waveforms up to max of 50 mA at a 1:1 ratio.
- 16. Take Home Message: Diabetic neuropathy is common among Type II DM patients and can lead to serious consequences including amputation. As therapists we need to improve their somatosensory processing in order to increase their functional mobility. Interventions to improve ROM, sensation and dynamic balance are examples of techniques to achieve that goal.
- 17. References: 1. Akbari, M., Jafari, H., Moshashaee, A., Forugh, B. "Do diabetic neuropathy patients benefit from balance training?". JRRD. 2012; 49: 333-338. 2. Amemiya, A., Noguchi, H., Oe, M, et al. "Elevated plantar pressure in diabetic patients and its relationship with their gait features". Gait & Posture. 2014; 40: 408-414. 3. Najafi, B., Crews, R., Wrobel, J. "A novel plantar stimulation technology for improving protective sensation and postural control in patients with diabetic peripheral neuropathy: a double-blinded, randomized study". Gerontology. 2013; 59: 473-480. 4. Perkins, B., Orszag, A., Ngo, M., Ng., E., New, P., Bril, V. "Prediction of incident diabetic neuropathy using the monofilament examination." Diabetes Care. 2010; 33: 1549-1554. 5. Salsabili, H., Bahrpeyma, F., Forogh, B., Rajabali, S. "Dynamic stability training improves standing balance control in neuropathic patients with type 2 diabetes". JRRD. 2011; 48: 775-786. 6. Salsabili, H., Bahrpeyma, F., Esteki, A., Karimzadeh, M., and Ghomashchi, H. "Spectral characteristics of postural sway in diabetic neuropathy patients participating in balance training." Jour. Of Diabetes & Metabolic Disorders. 2013; 12: 29-37. 7. Sartor, C., Hasue, R., Cacciari, L. et al. "Effects of strengthening, stretching and functional training on foot function in patients with diabetic neuropathy: results of a randomized controlled trial." BMC Musculoskeletal Disorders. 2014; 15: 137-150. 8. Tesfaye, S., Boulton, A., Dyck, P. et al. "Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments." Diabetes Care. 2010; 33: 2285-2293.
Editor's Notes
- (chronic, symmetrical, length) Dependent Sensorimotor Polyneuropathy: most common kind that occurs.
- *These members aren't common to every condition but are beneficial for a patient with diabetic neuropathy.
- While it's not in our scope to diagnose a patient with diabetic neuropathy during our initial evaluation assessment of sensation is relevant. A study by Perkins et al identified a baseline regarding the monofilament score that predicts the probability of a patient developing diabetic neuropathy in the next 4 years. Monofilaments are cost and time efficient. Use of this tool is helpful in assessment of a patient's sensory loss or when tracking progress. The score of sensate stimuli that was determined by < 5/8. In addition inter- and intrarelater reproducibility was excellent for the following protocol:
- Please refer to attached handout for the specific protocol: The improvement was modest but would be useful if applied consistently as a complementary intervention. In addition plantar pressure re-distribution did occur which can positively influence participation. A decrease in COP displacement velocity was also noted. All of these together provide an improved dynamic loading pattern in diabetic neuropathy patients.6
- Akbari (1) used the Biodex Balance System (BBS), wobble board and rocker board for training.
- Plantar pressure in the stance phase was divided into four areas of the foot. Gait characteristics were measured via sensors at the sacrum and the feet. Results: may be possible to prevent diabetic foot ulcers by increasing foot motion during the mid-stance phase. Passive exercise aimed at increasing ankle ROM in patients with sensory neuropathy or long standing diabetes may assist in achieving this. Normally: the foot performs a rolling motion, in which the ankle is used as a rocker, during mid-stance. The benefits of this is to distribute plantar pressure primarily through inversion at the ankle. When this motion is small then a small area of the plantar surfaces receives a highly concentrated plantar pressure. In addition this lack of motion at the ankle affects the loading pattern at the knee and hip. It can also be related to an overall decrease in proximal stability. Other recommendations include: increasing awareness of gait and using larger rolling motions during walking (rolling motions are around the anteroposterior axis). Kind of like think big??