More Related Content
Similar to Accurate and Precise Performance of the BD FACSVia™ System
Similar to Accurate and Precise Performance of the BD FACSVia™ System (20)
Accurate and Precise Performance of the BD FACSVia™ System
- 1. Accurate and Precise Performance of the BD FACSVia™ System
for Determination of CD4 Cell Count and %CD4 Cell concentration
Charlene Bush-Donovan, Julie Nguyen, Maya Kalyan, Anna Lin, Tom Frey
BD Life Sciences, 2350 Qume Drive, San Jose, CA 95131
Introduction
HIV/AIDS affects approximately 37 million people globally including 2.6 million children generating severe health and
development issues in the world, particularly in resource poor countries. A steady decrease of CD3+CD4+ lymphocyte
counts typically exhibits in HIV+ individuals as the infection progresses resulting in a dysfunctional immune system with
increased opportunistic infections and complications which often can lead to death. The full access to the highly effec-
tive ART therapy by the HIV+ community has dramatically reduced mortality and morbidity by allowing sustained control
of viral replication with improved life quality and expectancy. Determination of CD4 absolute count and percentages
plays a critical role in the diagnosis of HIV/AIDS, initiation of ART, treatment monitoring and patient risk management
rendering CD4 count as an important clinical laboratory test. Providing easy access to flow cytometric technology for
HIV/AIDS diagnosis and monitoring is part of the global effort to decrease the rate of HIV infections and to end the AIDS
epidemic by 2030.
To meet global health needs, BD has developed the new and affordable BD FACSVia™ System. It is a small and
easy-to-use flow cytometer that features a compact optical design with fixed alignment. The BD FACSVia System
contains two lasers and four fluorescence detectors for use with various biological assays. The BD FACSVia instru-
ment provides pre-optimized detector settings so that users do not have to adjust PMT voltages and compensation
during daily use and operation. Daily one-step BD™ Cytometer Setup and Tracking (CS&T) procedure for instru-
ment QC on the BD FACSVia System can be accomplished in less than five minutes, which provides quality control
for electronics, fluidics, and optical performance as well as automatic optimization of instrument compensation. QC
results are tracked by BD FACSVia™ clinical software for long-term monitoring of instrument performance. New
design features, coupled with an intuitive user interface (UI) on the BD FACSVia system, significantly reduce the
number of clicks users have to make when running clinical assays. Improved workflow on the BD FACSVia Sys-
tem, such as simultaneous data analysis during sample acquisition or system cleaning, saves time and labor for
routine laboratory operation. The BD FACSVia™ Loader option is available to increase sample throughput in clini-
cal settings.
The BD Tritest™ CD4/CD8/CD3, and BD Tritest CD3/CD4/CD45, and BD Multitest IMK assays available on the BD
FACSVia system in Europe is designed to automatically enumerate absolute count and percentages of T, B and NK
lymphocytes using the BD Testest™ , BD Multitest IMK reagents with BD Trucount™ Tubes. To validate the BD
FACSVia System using these assays, we evaluated multiple BD FACSVia systems to demonstrate robust perfor-
mance using HIV+ patients and normal donors.
Methods
Instrument setup and QC
The BD FACSVia systems were set up using BD™ CS&T Beads and BD FACSVia clinical software. The CS&T Beads
were prepared by adding two drops of beads into 500 µL of DI water, then run on the BD FACSVia instrument to gener-
ate a passing Instrument QC report.
On the predicate system, the BD FACSCalibur™, BD Calibrite™ beads were prepared per the BD instructions for use
and run on the BD FACSCalibur instrument using BD FACSComp™ software to set up the BD FACSCalibur instrument.
A Pass on the BD FACSComp QC report was obtained on each study day.
The BD FACSVia and BD FACSCalibur instrument systems were also qualified by running process controls. BD Mul-
tiCheck control cells were prepared using the BD Tritest and Multitest reagents and run on both BD FACSVia and BD
FACSCalibur systems. The absolute count of lymphocyte subsets of the BD Multicheck control cells must pass the
specification range provided by the manufacturer on both the BD FACSVia and FACSCalibur instruments.
Method comparison
Method comparison was performed at BD Life Sciences with a total of 208 HIV+ and normal donor samples in EDTA
tubes. Each whole blood specimen was stained with the BD Tritest CD4/CD8/CD3, and BD Tritest CD3/CD4/CD45, and
BD Multitest IMK (CD3/CD8/CD45/CD4 and CD3/CD16+56/CD45/CD19) reagents in BD Trucount tubes and
analyzed on the BD FACSVia System (Test) and BD FACSCalibur cytometer (Predicate). Acquisition was carried out on
a sample loader or using manual tube loading method. Lymphocyte subset absolute count and percentages were gen-
erated and compared between the predicate (reference) and test systems. Deming regression and Bland-Altman analy-
sis and Concordance Analysis were performed for lymphocyte subsets for the cell absolute count and percentages.
Precision
A 21-day study was conducted at BD Life Sciences, to assess within-site precision. Estimates of precision for the enu-
meration of lymphocyte subset percentages and absolute counts were determined across three BD FACSVia flow cy-
tometers and three operators by acquiring two concentrations of analyte, BD Multi-Check CD4 Low control and BD Mul-
ti-Check control, stained in duplicate with three lots of the BD Multitest IMK (CD3/CD8/CD45/CD4 and CD3/ CD16+56/
CD45/CD19) reagents. Two separate runs were analyzed separately during each of the 21 tested days.
Linearity
Eleven concentration levels of CD4 cells were prepared from normal donor whole blood. Triplicate stained samples us-
ing each of the reagents were measured on one BD FACSVia system to determine lymphocyte subset absolute counts
in the 11 linearity samples. Statistical analysis based on the CLSI guidance document EP6-A was performed to deter-
mine system linearity.
PRESENTED AT THE 21ST
INTERNATIONAL AIDS CONFERENCE - DURBAN,
SOUTH AFRICA
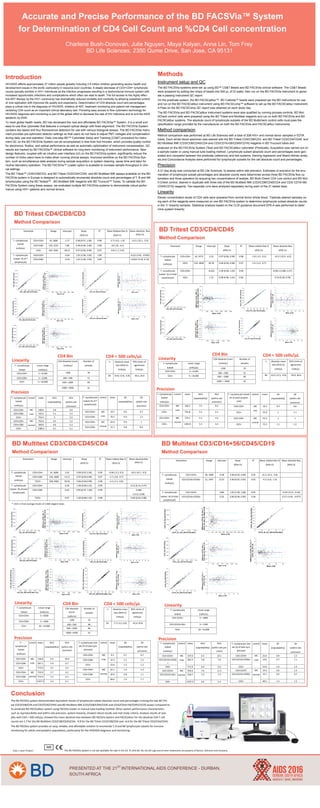
BD Tritest CD4/CD8/CD3
Method Comparison
BD Tritest CD3/CD4/CD45
Method Comparison
BD Multitest CD3/CD8/CD45/CD4
Method Comparison
BD Multitest CD3/CD16+56/CD45/CD19
Method Comparison
T –Lymphocyte
Subset
Linear range
(cells/µL)
CD3+CD4+ 5—6,500
CD3+CD8+ 5—3,500
CD3+ 5—10,000
T –Lymphocyte
Subset
(cells/µL)
control mean %CV
(repeatability)
%CV
(within-site
precision)
CD3+CD4+ MC
Low
148.9 5.8 6.6
CD3+CD8+ 533.5 5.1 5.5
CD3+ 754.4 5 5.5
CD3+CD4+ 754.6 4.5 5.2MC
normalCD3+CD8+ 369.0 4.6 5.3
CD3+ 1180.2 4.1 5.1
T –Lymphocyte
Subset (% of T
Lymphocyte)
control mean SD
(repeatability)
SD
(within-site
precision)
CD3+CD4+ MC
Low
19.7 0.6 0.7
CD3+CD8+ 70.7 0.9 1.1
CD3+CD4+ 63.9 0.9 1MC
normalCD3+CD8+ 31.1 0.8 0.9
Linearity
Precision
T –Lymphocyte
Subset
Linear range
(cells/µL)
CD3+CD4+ 5—6,500
CD3+ 5—10,000
Linearity
Precision
T –Lymphocyte
Subset
(cells/µL)
control mean %CV
(repeatability)
%CV
(within-site
precision)
CD3+CD4+ MC
Low
146.2 7.5 8.3
CD3+ 791.8 5.2 6.1
CD3+CD4+ 779.1 5.3 6.4MC
normal
CD3+ 1304.0 5.3 6.3
T –Lymphocyte Subset
(% of total Lympho-
cyte)
control mean SD
(repeatability)
SD
(within-site
precision)
CD3+CD4+ MC
Low
10.2 0.5 0.6
CD3+ 55.0 1 1.1
CD3+CD4+ 43.2 1 1MC
normal
CD3+ 72.3 1.1 1.2
T –Lymphocyte
Subset
Linear range
(cells/uL)
CD3+CD4+ 5—6500
CD3+CD8+ 5—3500
CD3+ 10—14,000
T –Lymphocyte
Subset
Linear range
(cells/uL)
CD3-CD19+ 5—1800
CD3-(CD16+56)+ 5—1300
CD3+ 10—14,000
T –
Lymphocyte
Subset
(cells/µL)
control mean %CV
(repeatability)
%CV
(within-site
precision)
CD3+CD4+ MC
Low
136.8 9.3 10.0
CD3+CD8+ 587.1 5.0 6.7
CD3+ 773.0 4.5 6.5
CD3+CD4+ 752.9 5.7 6.2MC
normalCD3+CD8+ 374.4 5.3 6.3
CD3+ 1227.3 5.4 6.1
T –Lymphocyte Sub-
set (% of total Lym-
phocyte)
control mean SD
(repeatability)
SD
(within-site
precision)
CD3+CD4+ MC
Low
9.5 0.7 0.7
CD3+CD8+ 37.3 1.2 1.5
CD3+ 53.6 1.2 1.2
CD3+CD4+ 42.1 1.0 1.2MC
normalCD3+CD8+ 20.9 0.8 1.1
CD3+ 68.6 1.4 1.7
T –Lymphocyte
Subset
(cells/µL)
control mean %CV
(repeatability)
%CV
(within-site pre-
cision)
CD3-CD19+ MC
Low
337.0 6.5 10.1
CD3-(CD16+CD56)
+
282.2 5.8 7.0
CD3+ 771.9 4.0 5.6
CD3-CD19+ 259.6 7.6 11.5MC
normalCD3-(CD16+56)+ 218.7 7.5 7.5
CD3+ 1237.2 4.6 5.4
T –Lymphocyte Sub-
set (% of total Lym-
phocyte)
control mean SD
(repeatability)
SD
(within-site
precision)
CD3-CD19+ MC
Low
23.4 0.9 1.5
CD3-(CD16+CD56)+ 19.6 0.7 1.1
CD3+ 53.6 1.0 1.3
CD3-CD19+ 14.3 0.9 1.3MC
normalCD3-(CD16+CD56)+ 12.1 0.6 0.7
CD3+ 68.5 1.5 1.5
Conclusion
The BD FACSVia system demonstrated equivalent results of lymphocyte subset absolute count and percentages running the two BD Trit-
est (CD3/CD8/CD4 and CD3/CD4/CD45) and BD Multitest IMK (CD3/CD8/CD45/CD4) and (CD3/CD16+56/CD45/CD19) assays compared to
its predicate BD FACSCalibur system using FACSVia loader or manual tube loading method. Other system performance characteristics
such as reproducibility and within-site precision, system linearity, showed robust results and met study criteria. Analysis results of sam-
ples with CD4 < 500 cells/µL showed the mean absolute bias between BD FACSVia System and FACSCalibur for the absolute CD4 T cell
counts are 1.7 for the BD Multitest CD3/CD8/CD45/CD4, -9.8 for the BD Tritest CD3/CD8/CD4 and –6.6 for the BD Tritest CD3/CD4/CD45.
The BD FACSVia system provides an easy, reliable, and affordable solution to enumerate T, B and NK lymphocyte subsets for immune
monitoring for adults and pediatric populations, particularly for the HIV/AIDS diagnosis and monitoring.
LinearityLinearity
PrecisionPrecision
Class 1 Laser Product. The BD FACSVia System is not yet available for sale in the US. © 2016 BD. BD, the BD Logo and all other trademarks are property of Becton, Dickinson and Company.
Parameters Range Intercept Slope
(95% CI)
R2
Mean relative Bias %
(95% CI)
Mean absolute Bias
(95% CI)
T –Lymphocyte
Subset
(cells/µL)
CD3+CD4+ 14, 2608 2.63 0.99 (0.97,1.00) 0.99 -0.90 (-2.2, 0.5) -8.6 (-16.7, -0.5)
CD3+CD8+ 150, 2848 14.11 0.97 (0.95,0.98) 0.97 -1.7 (-2.8, -0.7)
*CD3+ 306, 4683 39.63 0.96 (0.94,0.98) 0.98 -1.4 (-2.1, -0.6)
T –Lymphocyte
Subset (% of total
Lymphocyte)
CD3+CD4+ 0.29 1.00 (0.99,1.01) 0.99 0.31 (0.14, 0.47)
CD3+CD8+ 0.62 0.99 (0.97, 1.00) 0.99 0.068
(-0.15, 0.28)
*CD3+ 0.97 1.00 (0.98,1.02) 0.98 0.69 (0.50, 0.88)
Parameters Range Intercept Slope
(95% CI)
R2
Mean relative Bias %
(95% CI)
Mean absolute Bias
(95% CI)
T –Lymphocyte
Subset
(cells/µL)
CD3-CD19+ 28, 1088 -4.98 0.96 (0.93, 0.99) 0.95 -8.2 (-10.5, -5.8)
CD3-(CD16+CD56)+ 22, 1497 12.01 0.90 (0.87, 0.93) 0.95 -4.3 (-6.6, -1.9)
T –Lymphocyte
Subset (% of total
Lymphocyte)
CD3-CD19+ -0.80 1.03 (1.00, 1.06) 0.95 -0.39 (-0.57, -0.20)
CD3-(CD16+CD56)+ 0.20 0.96 (0.94, 0.99) 0.96 -0.27 (-0.45, -0.077)
*: CD3+ is from average results of 2 IMK reagent tubes.
Range Intercept Slope
(95% CI)
R2
Mean Relative Bias %
(95% CI)
Mean Absolute Bias
(95% CI)
Parameter
T –Lymphocyte
Subset
(cells/µL)
CD3+CD4+ 19, 2686 -1.57 0.98 (0.97, 1.00) 0.98 -2.7 (-4.0, -1.4) -13.5 (-22.1, -5.0)
CD3+CD8+ 149, 3252 7.88 0.98 (0.96, 1.00) 0.98 -10 (-20, -0.1)
CD3+ 303. 5061 28.52 0.97 (0.96, 0.99) 0.97 -0.8 (-1.7, 0.0)
T –Lymphocyte
Subset (% of T
Lymphocyte)
CD3+CD4+ -0.56 1.01 (1.00, 1.02) 1.00 -0.23 (-0.41, -0.052)
CD3+CD8+ -0.34 1.01 (1.00, 1.02) 0.99 -0.052 (-0.25, 0.15)
Range Intercept Slope
(95% CI)
R2
Mean relative Bias %
(95% CI)
Mean absolute Bias
(95% CI)
Parameter
T –Lymphocyte
Subset
(cells/µL)
CD3+CD4+ 10, 2575 3.32 0.97 (0.96, 0.99) 0.98 -1.8 (-3.2, -0.5) -14.5 (-22.9, -6.0)
CD3+ 314, 4858 36.78 0.96 (0.94, 0.98) 0.97 -1.5 (-2.4, -0.7)
T –Lymphocyte
Subset (% of total
Lymphocyte)
CD3+CD4+ -0.022 1.00 (0.99, 1.02) 0.99 0.091 (-0.085, 0.27)
CD3+ 1.72 0.98 (0.96, 1.01) 0.96 0.53 (0.28, 0.78)
CD4 Bin
CD4 Absolute Count
(cells/µL)
Number of
samples
<200 34
200—500 51
500—1000 83
1000—4500 41
CD4 Bin
CD4 Absolute
Count
(cells/uL)
Number of
samples
<200 35
200—500 48
500—1000 84
1000—4500 41
CD4 Bin
CD4 Absolute Count
(cells/µL)
Number of
samples
<200 33
200 —500 51
500 —1000 83
1000 — 4500 42
Absolute mean
bias (95% CI)
Cells/µL
95% Limits of
agreement
Cells/µL
n
-9.8 (-13.8, -5.8) -46.3, 26.685
CD4 < 500 cells/µL CD4 < 500 cells/µL
Absolute mean
bias (95% CI)
Cells/µL
95% Limits of
agreement
Cells/µL
n
-6.6 (-12.5, -0.6) -59.9, 46.884
Absolute mean
bias (95% CI)
Cells/µL
95% Limits of
agreement
Cells/µL
n
1.7 (-3.2, 6.6) -42.4, 45.883
CD4 < 500 cells/µL