This document discusses heart failure, including:
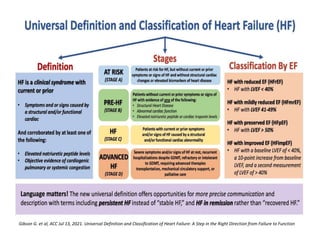
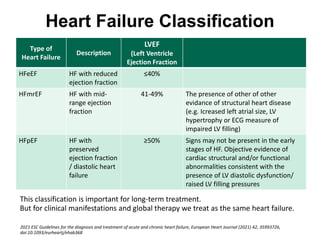
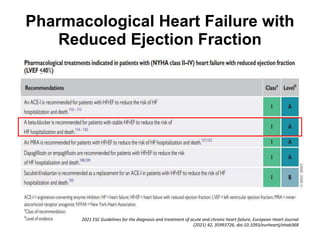
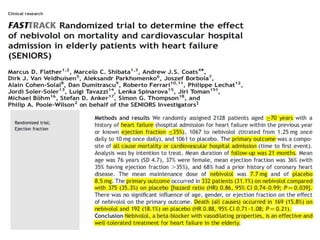
- Heart failure can be classified as HFrEF (ejection fraction ≤40%), HFmrEF (ejection fraction 41-49%), or HFpEF (ejection fraction ≥50%).
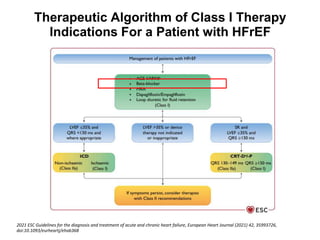
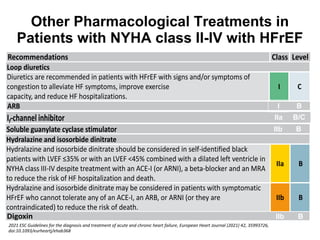
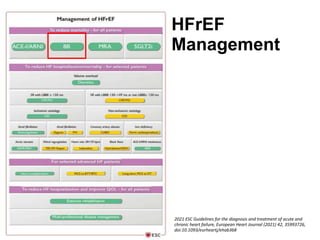
- Treatment for HFrEF focuses on ACE inhibitors, ARBs, beta-blockers, MRAs, and other drugs depending on symptoms.
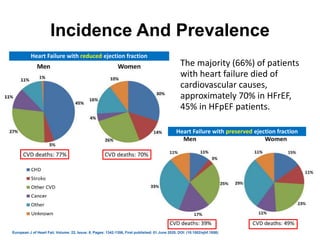
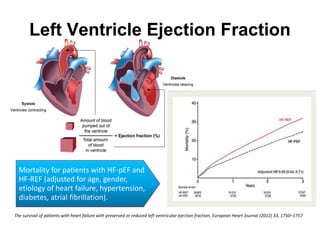
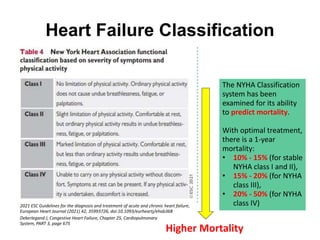
- Prognosis is generally worse for HFrEF than HFpEF, with higher mortality rates. The NYHA classification also correlates with mortality risk.
- Optimal treatment can reduce 1-year mortality to 10-15% for NYHA I-II, 15-20% for NYHA III, and 20








































![Heart failure – an update [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/heartfailureanupdateautosaved-110321012825-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





























