1. Background
Objectives
Methods
Results
Discussion and Implications
•The use of direct oral anticoagulants (DOACs) is increasing and there is a greater need
to understand how to manage DOACs in specific clinical scenarios (e.g. patients who
require interruption for procedures) in order to optimize safety.
• At Sunnybrook Health Sciences Centre (SHSC), there is a guideline for peri‐procedural
management of DOACs on the intranet, but we are unaware of how often this guideline
is used in practice and how clinicians make their decisions peri‐procedurally.
•This study was conducted to identify the gap between the guideline and practice and
to characterize patients’ adherence to instructions for peri‐procedural management of
anticoagulants.
1. Characterize the patient population receiving DOACs and undergoing elective
coronary angiography.
2. Examine current peri‐procedural practices at SHSC and the associated outcomes
a) Physician adherence to SHSC Guideline
b) Patient adherence to physicians’ instructions
3. Examine patients’ pre‐procedural coagulation levels (by obtaining a pre‐
procedural blood sample) and describe any relationships with the outcomes
4. Make recommendations to update and improve existing guidelines for peri‐
procedural management of DOACs
This is a prospective, observational study conducted in patients who were receiving
DOACs and undergoing elective coronary angiography (CA) with our without subsequent
percutaneous coronary intervention (PCI).
Eligible
Patient
1. Informed Consent Letter
2. Patient Information Collected
3. Physician Instructions to
Patients Collected
4. Blood sample collected
Pre‐procedure
Post‐procedure
•Informal interviews were conducted with cardiac triage coordinators who are responsible
for booking procedure appointments and relaying physicians’ instructions to patients to
identify current practice and practice use of the guideline.
•A brief informal questionnaire was distributed to physicians to understand how peri‐
procedural decisions regarding DOAC management were made.
•Anti‐Xa levels were measured for apixaban and rivaroxaban using the HemoSIL® and
Biophen® DiXal assays respectively. Dilute thrombin time (Hemoclot®) was used to measure
dabigatran levels. PT, INR, PTT and Thrombin Time were also run on all the samples.
•Descriptive statistics was used to analyze the data.
Peri‐procedural Info Collected
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1 3 5 7 9 11 13 15 17 19 21 23
# of Days
DOACs Held
Patient Number
Patient Adherence to Physician Instructions
Physician
Instruction
s
Number of
Days the
Patient
Held DOAC
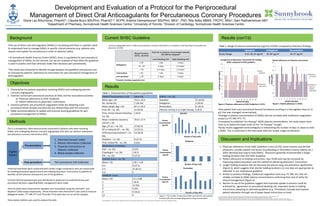
Figure 2. Physician adherence to SHSC Guideline is 12.5%. Figure 3. Patient adherence is 70.8%.
0
5
10
15
20
25
30
35
40
45
0 1.5 2 2 2 3 3 3 3 3 4
Plasma
Concentration
(ng/ml)
Number of Days Held
Apixaban
0
5
10
15
20
25
30
35
1 2 3 4 4
Plasma
Concentration
(ng/ml)
Number of Days Held
Dabigatran
0
5
10
15
20
25
30
35
40
0 1.5 2 2 2 3 3 3
Plasma
Concentration
(ng/ml)
Number of Days Held
Rivaroxaban
Apixaban Dabigatran Rivaroxaban
Study Range 0.41‐38.10 ng/ml 10‐30 ng/ml 16‐37 ng/ml
Figure 1. The number of days each DOAC was held for each patient
is shown with the corresponding plasma drug concentration.
Results (con’t’d)
Table 2. Range of plasma concentrations (ng/ml) of DOAC compared to literature findings.
1. Physician adherence to the SHSC Guideline is low (12.5%). Some reasons may be that
physicians consider patient risk factors (e.g bleeding or thrombotic history, elderly, etc.)
when deciding how long to hold DOACs. Physicians generally recommended a longer
holding duration than the SHSC Guideline.
2. Patient adherence to holding instructions was 70.8% and may be increased by
improving patient education and the method of delivering physicians’ instructions.
3. Longer holding durations did not decrease the plasma drug concentrations significantly
(Figure 3), which suggests that shorter holding durations (i.e one day) are appropriate as
reflected in our institutional guideline.
4. Similar to previous findings, traditional coagulation tests (e.g. PT, INR, etc.) did not
reliably correlate to DOAC plasma concentrations confirming their lack of utility for
clinical management (Figure 4).
5. Barriers to use of the guideline suggest that improved uptake in practice could be
achieved by: agreement on procedural bleeding risk, improved clarity in holding
instructions, adopting an alternate guideline (e.g. Thrombosis Canada) and improve
patient education through use of paper‐based instructions or tools.
Coronary angiography with or without percutaneous coronary intervention is considered a low bleeding risk procedure by
physicians at SHSC.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1 3 5 7 9 11 13 15 17 19 21 23
# of Days to Hold DOAC
Patient Number
Comparison of physicians' instructions for holding
DOAC compared to SHSC guideline
SHSC
Guideline
Physicians'
Instructions
Patient Characteristics n=24 Value (%)
Mean age ± SD 75.8 ± 10.4
No. female (%) 7 (29.2%)
Mean weight (kg) ± SD 87.4 ± 26.4
Prior MI – no. (%) 11 (45.8)
Prior clinical relevant bleeding –
no. (%)
2 (8.3)
Mean creatinine clearance
ml/min ± SD
70.8 ± 27.9
Age >75 yrs – no. (%) 15 (62.5)
HF or reduced LEF – no. (%) 13 (54.2)
HTN requiring treatment – no.
(%)
23 (95.8)
Diabetes – no. (%) 9 (37.5)
Prior stroke/TIA – no. (%) 6 (25)
Medications at Baseline
ASA – no. (%) 6 (25)
Clopidogrel – no. (%) 2 (8.3)
PPI – no. (%) 9 (37.5)
CHADS2 Score – no. (%)
Mean ± SD 2.96 ± 1.04
0‐2 9 (37.5)
3‐4 15 (62.5)
5‐6 0
HASBLED Score
Mean ± SD 2.5 ± 0.88
1 2 (8.3)
2 12 (50)
3 6 (25)
4 4 (16.6)
>5 0
DOACs – no. (%)
Apixaban 11 (45.8)
Dabigatran 5 (20.8)
Rivaroxaban 8 (33.3)
Patients coming in on triple therapy 2 (8.3) •One patient had a peri‐procedural femoral hematoma resulting in a hemoglobin drop of 12
g/L that was managed conservatively .
•Changes in plasma concentrations of DOACs did not correlate with traditional coagulation
assays (i.e PT, INR, PTT, TT)
•Compared to published “on‐therapy” DOAC plasma concentrations, the study values were
close to or below the lower limits of the “on‐therapy” troughs
•Study results suggested some ambiguity in interpreting the number of days vs. doses to hold
a DOAC. This is confirmed in the interviews with the cardiac triage coordinators.
1. Atul et al. 2014 focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation. Can J Cardiol. 2014;30:1114‐30.
2. Thrombosis Canada. Peri‐operative management of patients who are receiving new oral anticoagulant (dabigatran, rivaroxaban, apixaban).
3. Heidbuchel H et al. European Heart Rhythm Association practical guide on the use of new oral anticoagulants in patients with non‐valvular atrial fibrillation. Eurospace. 2013;15:626‐51.
4. Sunnybrook Health Sciences Center Thromboembolism Service. Peri‐Procedure management of patients receiving an oral direct inhibitor of coagulation (apixaban, rivaroxaban, dabigatran). 2014.
Table 1. Characteristics of the patient population.
Development and Evaluation of a Protocol for the Periprocedural
Management of Direct Oral Anticoagulants for Percutaneous Coronary Procedures
Gloria Lau BSc(Hons), PharmD1; Claudia Bucci BScPhm, PharmD1,2, ACPR; Artemis Diamantouros2 BScPhm, MEd1,, PhD; Rita Selby MBBS, FRCPC, MSc2; Sam Radhakrishnan MD3
1Department of Pharmacy, Sunnybrook Health Sciences Centre; 2University of Toronto; 3Division of Cardiology, Sunnybrook Health Sciences Centre
Current SHSC Guideline
Acknowledgements: Thank you to the coagulation laboratory at Sunnybrook Health Sciences Centre and St. Michael’s Hospital for performing the coagulation testing.