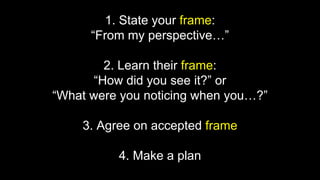
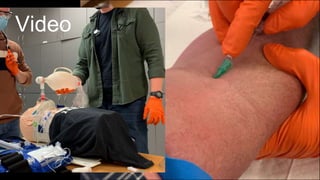
Nearly half of medical professionals surveyed did not receive feedback on their work in the previous 30 days. Providing effective feedback requires establishing a culture where feedback is expected and using the right approach depending on what is being evaluated, such as clinical decisions versus psychomotor skills. There are also guidelines for how feedback should be delivered, such as being specific, discussing different perspectives, and creating an action plan to improve. The future of feedback may involve greater use of peer-to-peer and video feedback as well as coaching.