
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Perforator flaps
Similar to Perforator flaps (20)
More from Dr.Avinash Rao Gundavarapu
More from Dr.Avinash Rao Gundavarapu (20)
Recently uploaded
Recently uploaded (20)
Perforator flaps
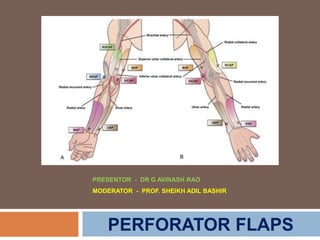
- 1. PRESENTOR - DR G AVINASH RAO MODERATOR - PROF. SHEIKH ADIL BASHIR PERFORATOR FLAPS
- 2. An overview of flap history
- 3. A brief history of perforator flaps
- 4. This concept was firstly put forward by Koshima and Soeda (1989). They described an inferior epigastric artery skin flap without rectus abdominis muscle for reconstruction of floor-of-the-mouth and groin defects Described that a large flap without muscle could survive on a single muscle perforator.
- 5. The perforator flap is - island pattern flap with the blood supply from thin skin perforator vessels (diameter ≥0.5 mm after perforating deep fascia). At the beginning, perforator flap developed slowly and failed to attract much attention. Then two milestone meetings in Ghent, Belgium (2001) and Yinchuan, China (2005) promoted the research and development of perforator flap.
- 8. Perforator flap is an axial pattern flap, with thin subcutaneous tissue without deep fascia and gets nourished by Septo / Myocutaneous artery perforator. Originally, the concept of perforator flaps is attributed to musculo-cutaneous perforators only. But later extensive clinical practice had broadened the concept and included all kinds of cutaneous perforators. Currently, the concept has been expanded to a broader sense and includes all island pattern flaps nourished by blood vessels perforating deep fascia.
- 12. There are two types of perforating vessels to the skin. Musculocutaneous perforators: this type of perforator is the cutaneous vessel - penetrating underlying muscle., Longer vascular pedicle can be obtained by intramuscular dissection Septocutaneous perforators: this type of perforator is the cutaneous vessel - piercing the fascial septum between muscles. Through intraseptal dissection, the perforator can be traced to its deep source artery
- 13. Vascular Plexus of the Integument There are 5 layers of vascular plexus in the integument, from deep to surface; it is subfascial, suprafascial, adiposal, subdermal, and dermal. Three vascular plexus of integument are rich and abundant – suprafascial plexus, perineural and perivenous plexus, and subdermal plexus
- 14. Angiosome Area Angiosome is a three-dimensional complex with the same blood supply and consists of skin and deep tissues (muscles, tendons, bones). Def – Area supplied by a big deep vessel and runs along connective tissue, and radiates to movable parts from the fixed parts.
- 15. The concept of angiosome area 1. Modified the transplantation mode of flaps, 2. Exploited more flap donor sites and derived special modes of perforator flap. Eg - propeller perforator flap, flow-through perforator flap, superthin perforator flap, conjointed perforator flap, and chimeric perforator flap.
- 16. Perforasome Vascular arterial territory of a perforator
- 17. Tang Maolin et al. in 2002 successfully modified the angiography and combined it with the modern computer imaging technology and described origins, runnings and distribution of perforators (diameter ≥0.5 mm) in the skin and subcutaneous tissues and the distribution map of human skin perforators was plotted. The map revealed that a total of 61 skin-originated vessels in our body gave out 442 perforators (diameter ≥0.5 mm) to nourish the skin
- 18. In Their Study - The ratio of intramuscular perforator to intermuscular space perforator was 3:2, The average diameter of perforator vessels was 0.7 mm. The average running distance in superficial fascia was measured as 3.3 cm. They have also studied the number of perforators from each of the source arteries and their distribution area were calculated
- 20. Perforator Vessel It is a nutrient vessels that supply blood for subcutaneous tissues and skin after originating from the source artery passing through the deep fascia and exiting from the superficial layer of the fascia. (not including the source artery), It can be an indirect perforator or a direct perforator.
- 22. Indirect perforator Indirect perforator runs through deep muscle and deep fascia to subcutaneous tissues and skin. Longer and thicker vessel pedicles can be obtained by tracing the anatomical structure of the deep muscles after cutting open the deep fascia.
- 23. Direct perforator Direct perforator usually runs through lacuna musculorum / intermuscular space / intermuscular septum, and then through deep fascia to subcutaneous tissues and skin. It is present in thin intermuscular space / lacuna musculorum, or between the muscles with same functions or in intermuscular septum (between muscle groups). By separating the intermuscular septum (intermuscular space), we can see that the perforator vessel orginates from the deep main artery.
- 25. Advantages Reduced donor-site morbidity Replace like with like. Faster recovery and reduced postoperative pain. Tailored to accurately reconstruct the defect Resurfacing shallow defects Freedom of orientation of the pedicle Longer pedicle can be harvested than with the parent septo-musculo cutaneous perforators Smaller defects – primary closure.
- 27. Pedicled Perforator Flap Pedicled perforator flap - perforator flap with a pedicle designed and harvested peripheral to the wound of recipient site by local transposition.
- 28. Free Perforator Flap Free perforator flap - perforator flap that is designed and dissected from any site, Require Microvascular vessel anastomosis for transfer.
- 30. Perforator Vessel Anastomosis The adjacent perforator vessels are connected by three types of anastomosis: (1) True anastomosis (diameter not reduced) - vessels run on the fascia or in fatty layer; (2) Obstructive anastomosis (diameter gradually reduced) vessels run in dermis. Ramus communicans are formed between true anastomosis vessels and obstructive anastomosis vessels to maintain the perfusion; (3) Potential anastomosis usually does not work under normal conditions.
- 32. Flap Donor Site Anatomical donor site refers to - vessel branches in anatomical morphology, and is the most basic vessel donor site . Hemodynamics donor site refers to the enlarged range of one donor site due to the extra blood supply from vessels at the adjacent donor site – Because the vessels at one side of the two donor sites are obstructed because of pressure gradient
- 33. Potential donor site refers to the expanded donor site due to human intervention (operation delay, drugs delay). Based on the need for covering defect, surgeon extend the area for flap harvest beyond the boundary of the hemodynamics donor, even to the adjacent donor site, and all the flaps can still survive.
- 35. “Point”, “Line”, and “Arc” in Perforator Flap Design Point - Point refers to the body surface position of vessel pedicle that supplies blood for perforator flap. For flap transfer, “point” is the axis point by which the flap rotates. The flap, after being resected, rotates around the axis point to repair the defects of recipient site. Line - refers to the axial lead of perforator flap. It is the body surface projection line of the nutritious vessel of perforator flap, and the long axis of perforator flap. The flap shall be designed at both sides of this line.
- 36. Arc - specific in transposition flaps - refers to the rotation arc of perforator flap. When adjacent wounds are repaired by transposition of vascular pedicle flap, the flap rotates along the axis point, and the points which the distal end of flap can reach forms an arc. Any tissue defect or wound can be repaired by this flap within this Arc.
- 38. Propeller Perforator Flap The perforator vessel adjacent to the wounds is used as the pedicle to harvest an island perforator flap, and the perforator vessel is used as the axis for rotation, with the big end of the flap (propeller) employed to repair the wound defects, and the small end (propeller) to cover the wounds in donor site, followed by a direct suture of the remaining wounds. The concept of propeller perforator flap, firstly put forward by Hallock in 2006, is generally characterized by: (1) island flap; (2) the perforator vessel locating at the eccentric end of flap; (3) a flap rotating as much as 180°.
- 39. Design of the Flap
- 40. Good caliber perforator - Skeletonize and complete free the perforator. True perforator-pedicled flap
- 41. Perforator caliber is not ideal - keep the septum and a quadrant adipofascial to protect the vessel and provide more venous drainage route. Perforator-plus- pedicled flap
- 50. Keystone flap The keystone island perforator flap (KPIF) is a perforator based advancement flap. Described and classified in 2003 by Behan It has a curvilinear trapezoidal shape representing the architectural shape of the keystone in Roman arches. It is designed over dermatomal segments with a flap width at a 1:1 ratio to an elliptical defect.
- 54. Principles for Perforator Flap Selection Transplantation Principles – Simple safe and effective method. Transplantation Methods – Pedicled or Free. Condition of Donor Site – Trauma / Surgery / Radiotherapy. Nature of Wound Surface – Tissue Deficit – Components in flap Scope of Recipient Site – Area needed cover
- 55. Procedures for Perforator Flap Preparation of Recipient Site.
- 56. Flap Design Method First introduced by Wei and coauthors in 2004 - termed as FREE-STYLE CONCEPT. Based on this this concept, any skin paddle based on a substantially sized perforator, localized by an audible Doppler signal, can be potentially harvested. With a substantial number of available perforators in the body, this approach increased the surgeon’s degree of freedom in terms of reconstructive options.
- 57. Flap Design Method Step 1- The first step in performing a free-style perforator flap is locating sizable perforators in the selected region of the body. Handheld Doppler ultrasonography - locating and mapping these cutaneous vessels. Carefully note the quality of the Doppler sound detected with particular attention given to the location of loud, high-pitched, and pulsatile signals. The vessels with more prominent sounds are marked with a larger dot and selected as the vessel that is intended to dissect. The flap is then designed centered on these perforators
- 58. Flap Design Method Step 2- Dissection is performed under loupe magnification (2.5–3.5×). Only one border of the proposed design should be incised initially for exploration. This provide the flexibility to alter the flap design. Step 3 - The flaps were dissected in the suprafascial plane to minimize donor-site morbidity by preserving fascia and cutaneous nerve that run immediately above the fascia. It is important to maintain meticulous hemostasis as excessive bleeding and subsequent staining of the tissues interferes with clear visualization and accurate identification of small vessels.
- 59. Flap Design Method Step 4 - After sizable cutaneous vessels are found, the deep fascia is cut to start mobilizing the vessels. Proceed with intramuscular dissection for musculocutaneous perforators or relatively straightforward in case of septocutaneous perforators. Retrograde mobilization of the vascular pedicle is continued until a sufficient length and size is achieved. Depending on the size of the perforators and the size of the flap that need to be harvested, the flap can be based on a single perforator or multiple perforators.
- 60. Flap Design Method Step 5 - Once all these crucial surgical decisions have been made and flap dimensions and design confirmed, the flap is completely islanded. (Pedicle is divided in free tissue transfer) In general, the average size of a single perforator-based flap is 100–200 cm 2 .
- 61. Flap Design Method Step 6 - Because of the inherent unpredictability of pedicle size and length, the surgeon should always have a “backup” plan when attempting a free- style perforator flap. The first exploratory incision should allow the opportunity of using the “backup” flap. In the thigh, for example, if the mapped vessel is located in the medial thigh, the first incision should be along the lateral margin. The dissection should be from lateral to medial. If no suitable skin vessels are encountered, the dissection direction will be shifted toward the lateral side for the harvest of the “backup” ALT flap.
- 62. Flap Design Method Step 7 - Critical to the success of harvesting a freestyle perforator flap is the intramuscular perforator dissection. Gentle handling is important to prevent vasospasm and to protect this thin flap from harvest to inset. Its pedicle consists of a small perforator that has been completely skeletonized during harvest and lacks a protective cuff of soft tissue around the site where the perforator enters the flap - making it susceptible to kinking, compression, and even rupture during the inset.
- 64. Pedicled Perforator Flap Transfer 1. Flap transposition is mainly used for repairing the wound surface exactly adjoining the perforator flap. It is the simplest procedure for flap transfer with a great convenience due to the absence of normal tissues between the flap and the wound surface. During the operation, it is not necessary to expose the flap nutritious vessel and cut off the skin at the pedicle.
- 65. 2. Flap advancement is mainly used for repairing the soft tissue defects at distal or proximal end of the flap. Generally, V–Y advancement is adopted to close the wound, and a posture of joint flexion can help to avoid pulling of vascular pedicle when advancing the perforator flap.
- 67. Factors Influencing Flap Advancement 1. Position of the skin island to the skin tension line. 2. Anatomical features of the perforator vessel. If possible, centering the flap on the main audible perforator is advisable, because eccentric pedicles may restrict flap advancement. 3. Types of perforator. Septocutaneous perforators, are found to be shorter and usually offer a lesser degree of advancement when compared with myocutaneous perforator. 4. The direction of advancement in extremities. In case of distal flap movement, a lesser degree of advancement is expected.
- 68. 3. Flap rotation is the most commonly used procedure for flap transfer. For instance, the propeller perforator flap is mainly used for repairing defects with in a distance or in an opposite direction. The maximum rotation angle of perforator flap pedicle can be as large as 180°. Most flaps are transferred through an open path, and the vascular pedicle cannot be turned around or curved in an acute angle, pressed or excessively pulled to - avoid blocking the blood supply to the vascular pedicle.
- 69. 4. Cross transplantation is considered in the healthy limb when serious wound cannot be repaired using an adjacent flap and there is no acceptable vessel in the recipient site for vascular anastomosis for flap free transplantation.
- 70. Most common complications Blood Supply to flap Hematoma Infection
- 71. There is a learning curve for every new procedure. Reading books and articles to get sufficient knowledge and follow standard steps can shorten the learning time, avoid mistakes, and prevent complications. The philosophy is forward step-by- step and leaves the opportunity of salvage with alternative flaps.
- 72. Perforator Flap from Upper Limbs Medial Arm Perforator Flap Lateral Arm Perforating Flap Proximal Radial Artery Perforator Flap Postero-Lateral Mid-Forearm Perforator Flap Distal Radial Artery Perforator Flap Snuffbox Radial Perforator Flap Proximal and Middle Ulnar Perforator Flap Distal Ulnar Perforator Flap Posterior Interosseous Perforator Flap Anterior Interosseous Dorsal Perforator Flap Dorsal Metacarpal Artery Perforator Flap Little Finger Perforator Flap Pedicled with Ulnar Palmar Artery Digital Dorsal Perforator Flap