Oral Medicine Phone Slides (4th BDS)
•
11 likes•935 views

Oral Medicine Test Slides for 4th Year BDS - Yangon Copyright by OM Department Teachers 🤫🤫🤫

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Oral Medicine Phone Slides (4th BDS)
Similar to Oral Medicine Phone Slides (4th BDS) (20)
More from Cing Sian Dal
More from Cing Sian Dal (20)
Recently uploaded
Recently uploaded (20)
Oral Medicine Phone Slides (4th BDS)
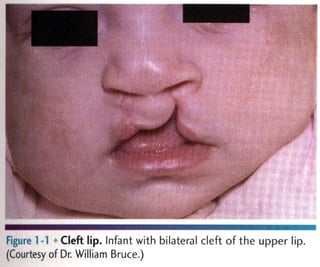
- 1. Figure 1 >1 Cleft Infant with bilateral Cleft of the upper lip. (Courtesy of Dr, William Bruce‘)
- 2. FlSlllc I 7 Paramedian lip pits. Bilateral piis (arrows) on lhe lower lip in a patient with van der Woude syndrome.
- 3. m Double lip. Redundant fold of (issue on the upper lip in a patient with Ascher syndrome. (Courtesy of RC. Zeig‘er.)
- 4. Figure I’ll Fordyce granules. Lesions at the commissure
- 5. Fxgmv l H,» Microglossia. Abnormally small tongue associated with constricted mandibular arch.
- 6. m.‘ .mmm‘ Fl‘h’ull‘ I I Microglossia. Associated constriction of the maxi Iary arch in he same patient shown in Figure 1716.
- 7. Figure 1-19 ' Ankyloglossia. Abnormal attachment of the lingual frenum, limitlng tongue mobility.
- 8. w Fugum I ~22 Fissured tongue. Moderate fissuring of the dorsal tongue. (From Allen CM, Camisa C: Diseases of the mouth and lips‘ In Sams WM, Lynch P, editors: Principles ofdermatology, New York, 1990, Churchill Livingstone.)
- 9. Figure 1724 H tongue. Eiongated. black-flaming fihform papillae on the posterior dorsai tongue.
- 10. figure l»27 >Van'cosities. Multiple purple dilated veins on the ventval and lateral surfam of the tongue.
- 11. Figure 1735 Exostoses. Multiple buccal exostoses of thc maxilr law and mandlbular alveolar ridges.
- 12. Figure l»38 Torus palatinus. Midline bony nodule of the palatal vault.
- 13. Figure 1-39 Torus palatinus. Large, lobulated palatal mass.
- 14. Figure 1-40 Torus palatinus. Asymmetric. lobulated bony mass.
- 15. Figure 1741 Torus mandibularis. Bllulmdl Iobulatod bony protuberames of the mandibular lingual alveolav ridge.
- 16. Figure 1742 Torus mandibularis. Masswe "kissmg" (on meet in the midline.
- 17. Figure 1 -48 ~ Stafne defect. Anterior radiolucent lesion ofthe body of the mandible associated with the sublingual gland.
- 18. Figurel-67 ‘ Dermoid cyst. Fluctuant midline swelling in the floor ofthe mouth (From Budnick SD: Handbook afpediatrir oral pathology. Chicago, 1981, Year Book Medical.)
- 19. Figure 1-69 Thyroglossal duct cyst. Swelling (arrow) of the anterior midline ofthe neck‘ (Courtesy of Drl Philip Sprinkle.)
- 20. Figure L77 Hemihyperplasia. Enlargement of the right sbde of the face. (Courtesy of Dr George Blazis)
- 21. Figure 1-78 Hemihyperplasia. Same patient as depicted in Figure 1777, with associated enlargement of the right half of the tongue. (Courtesy of Dr. George Blozis.)
- 22. Figure 2-1 > Environmental enamel hypoplas . Bilaterally symmetric pattern of horizontal enamel hypoplasia of the anterior dentition. Maxillary central incisors have been restored previously (From Neville BW, Damm DD, White DK: Color atlas ofclinicul oral pathology. ed 2, Baltimore, 1999. Williams & Wi ins.)
- 23. Figure 2-2 Environmental enamel hypoplasia. Same patient as depicted in Figure 271‘ Note the lack of enamel damage on bicuspids, (From Neville BW, Damm DD, White DK: Color atlas of clinical oral pathology, ed 2, Baltimore, 1999, Williams & Wilkins.)
- 24. Turner’s hypoplasia. Extensive enamel hypoplasia of mandibular first bicuspid secondary to previous inflammatory process associated with overlying first deciduous molar. (From Halstead CL, Blozis CG, Drinnan AJ, et al: Physical evaluation ofthe dental patient, St Louis, 1982, Mosbyt)
- 25. F ure 2-6 - Turner's hypopla 3. Extensive corona! hypopfasia of permanent maxillary left (entral incisor secondary to previous trauma to deciduous ce (ral incisor,
- 26. Figure 2A8 Dental fluorosis. Dentition exhibiting lusterless, white, and opaque enamel.
- 27. Figure 2-9 ' Dental fluoros White opaque alteration of the bicuspids and second molars in a patient who also exhibits discoloration of the teeth secondary to (etracycline use. Patient moved to area of endemic fluorosis at 3 years of age.
- 28. Figure 2-10 ~ Attrition. Extensive loss of coronal tooth height WIthout pulp exposure in patient with anterior edge-to-edge occlusionv
- 29. Figure 2-11 * Abrasion Horizontal cervical nokhes on the anterior mandibular dentition
- 30. Figure 2-12 Abrasion. Extensive recession and loss of buccal radlculardentin. Note visible pulp Canals that have been filled wllh lertiary dentin.
- 31. Abrasion. Notching of the right central incisor caused by improper use of bobby pins. The patient aiso exhibits environmental enamel hypopiasia of the anterior dentition. (Courtesy of Dr. Robert]. Corlin.)
- 32. Figure 2 14 Abra on. Notching ofthe ante or dentition on the right side caused by long-term use of tobacco pipe.
- 33. Erosion Extensive loss of buccal and occlusalh 'rnz tooth structure. Note that the amalgam margins are above the surface of the dentin.
- 34. mum Figure 2716 Erosion. Occlusal surface of the mandibular dentition exhibiting concave dentin depressions surrounded by eievated rims of enamel.
- 35. Erosion. Extensive loss of enamel and dentin on the buccal surface of the maxillary bicuspids. The patient had sucked chronically on tamarinds (an acidic fruit).
- 36. Figure 2-18 Erosion. Palatal surfaces of the maxillary dentition in which the exposed dentin exhibits a concave surface and a peripheral white line ofenamel. The patient suffered from bulimia
- 37. Figure 2-19 Abfraction. Deep and rrow enamel cervncal defects on the facial surface of the mandibular dentition (From Neville BW. Damm DD. White DK: Coloratlus of clinical om‘l pathology. ed 2, Baltimore, 1999, Williams & Wilkinsl)
- 38. m m» , Internal resorption (pink tooth of Mummery). Pmk disrolomh'on of H19 maxillary (Pntml indsor,
- 39. Exgm'e 1 21 Internal resorption. Same patient as depicted in Figure 2-21‘ Note extensive resorption of both maxil|ary central incisors,
- 40. Internal resorption. Balloonlike enlargement of the root canal,
- 41. Flgure 2-24 0 External resorption. Extensive Irregular destruc— tion of both roots of1he mandibular second molar associated wixh chronic periodontitis. (Courtesy of Dr. Tommy Shimer)
- 42. w Figure 2<25 ‘ External resorp Ion. “Motheaten” radiolucent alteration of the maxillary left central incisor The tooth had been reimplanted after traumatic avulsion. (Courtesy of Dr‘ Harry Meyers)
- 43. Figure 227 ~ External resorption. Diffuse external resorption of radicular dentin of maxillary dentition. This prOCESS arose after initiation of orthodontics.
- 44. Figure 2-40 Hypodont . MultIple developmentally mlssmgpel manent teeth and several retained deciduous teeth in a female adult
- 45. Figure 2742 Hypodontia, Developmentally missing maxillary lateral incisors. Radiographs revealed no underlying teeth, and there was no history of trauma or extraction.
- 46. Figure 2-43 * Hyperdon a (mesiodens). Erupted superr numerary, rudl'memary tooth of the anterior maxilla
- 47. Figure 2-44 Hyperdon a (mesiodens). U teral :uper- numerary tooth of the anterior maxilla, which has altered the eruption path of the maxil|ary right permanent central incisor.
- 48. supernumerary teeth of the anterior maxilla. Figure 2—45 % Hyperdontia (meslodens). Bulateral Inverted
- 49. Figure 2—46 '-» Hyperdontia. Right mandibular dentition exhibiting four erupted bicuspids.
- 50. Figure 2—47 v> Paramolar. Rudimentary tooth situated palatal to a maxiilary meter in a patient who also exhibits hypodontia.
- 51. Figure 2-48 + Paramolar. Radiograph of the same patient depicted in Figure 2-4.7 Note the fully formed tooth overlying crown of the adjacent molar.
- 52. Flgure 2749 Natal teeth. Mandihu|ar rentral I'n(i<ors (hat were erupted at birth.
- 53. Figure Z~50 ' Diffuse microdontla. Dentition in which the teeth are Smaller than normal and widely spaced within the arch
- 54. Figure 2—51 » Isolated microdon Ia (peg lateral). Small, cone, shaped right maxillary lateral incisor.
- 55. Figure 2-52 ’v Bilateral gemination. Two double teeth, The moth count was normal when each anomalous tooth was counted axone‘
- 56. Figure 2-53 Gemina n. Mandibular bicuspid exhibiting bifid crowni
- 57. Figme 2 SC Fusion. Double tooth in the place of the mandibular right lateral incisor and cuspid.
- 58. Figure 2—57 "v Fusnon. Bilateral double teeth in the place of the mandibular lateral incisors and cuspids.
- 59. Figure 2-59 Concrescence. Union by cementum of adjacent maxillary molars.
- 60. # Figure 2761 Concrescence. Cross photograph of the same teeth depicted in Figure 260. Histopathologir examination revealed that union occurred in the area of cemental repair previously damaged by a periapical inflammatory lesion.
- 61. Figure 2 3 Talon cusp. Acce ory cusp present on the palatal surface of H19 maxill y loft rpntral incisor: Note the (hreer pronged pattern, which rezemlfie: an eagle talon.
- 62. Figure 2-70 « Coronal den vag atus, type II. Mandibular lateral incisor exhibiting lingual bulbous enlargement at the site of (clonal opening of enamel invagination.
- 63. F gure 2-7] x Coronal dens vag natus, type II. Radiograph of the mandibular lateral incisor depicted in Figure 2-70. Note the radiopaque and enamel-lined invagination extending below the level of the cementoenamel junction.
- 64. Figure 2—72 Coronal dens invaginatus, type M. Cross photo- graph ofa sectioned tooth. Note the dilated invagination with apical accumulation of dystrophic enamel.
- 65. Figure 2773 Coronal dens nva atus, type III. Parulis overr lying vital maxillary cuspid and lateral incisor. The Luspld contained a dens Invaginatus that perforated t mesidl >urlace ofits root.
- 66. Figure 2-74 Coronal dens invaginatus, type III. Maxillary cuspid exhibiting an enamel invagination that parallels the pulp canal and perforates the lateral root surface (Courlesy of Dr. Brian Blocher.)
- 67. Figure 2—76 ' Enamel pearl. Mass of ectopic enamel located in the furcation area ofa molar tooth. (Courtesy of Dr‘ Joseph Beard.)
- 68. m ‘«w §§ Fegure 2779 Taurodontism. Mandibular molar teeth exhibiting increased pulpal apicoocclusal height With apically positioned pulpal floor and bifurcation. (Courtesy of Dr. Michael Kahn,)
- 69. Figure 2-81 O Hypercemento Mandibular first molar exhibiting thickening and blunting of the roots.
- 70. Figure 2-83 Ilacerahon. Maxlllary molar exhlbltlng sharp angulation of the roots‘ Note the interradicular bone.
- 71. Figure 2-87 v Supernumerary root. A, Cross photograph exhibiting a maxillary molar with a small supernumerary root. B, MeSIal-to-distal radiographic view exhibiting the a(cessory root with central pulp canal. lfa buccalitoJingual mdiographic view had been taken (as would be necessary in patient (are), the additional root would not have been evident.
- 72. Figure 2789 Hypoplastic amelogenesu Imperfecta, general- ized pitted pattern. Note the numerous pinpoint pits scattered across the surface of the teeth. The enamel between the pits is of normal thickness. hardness. and coloration, (From Stewart RE. Prescott CH: Oml facial genetics, St Louis, 1976, Mosby.)
- 73. Figure 2 95 Hypomaluration amelogenesis imperfecta. Denlition thibiting mottled, opaque white enamel with scattered areas 0{ brown discoloration.
- 74. Figure 2 ~96 Hypomaturation amelogenesis imperfecta, snowcapped pattern. Dentition exhibiting zone of white opaque enamei in the incisal and occlusal one fourth of the enamel surface. (Courtesy of DL‘ Heddie O. Sedano.)
- 75. Fugure 2-97 ' Hypocalcified amelogenesis imperfecta. Denti» lion exhibiting diffuse yellow-brown discoloration, Note numerous teeth wifll loss of coronaI enamel except for the cervical portion.
- 76. figure 2-101 Dentinogenesis imperfecta. Dentition exhib diffuse brownish discoloration and slight translucence.
- 77. Figure Z-IOZ ~’ Dentinogenesis imperfecta. Dentition exhibiting grayish discoloration with Significant enamel loss and attrition.
- 78. Flgul‘e 3-1 Chm Ic hyperplastlc pulpltls. Erythematous granulation tissue extruding from the pulp chamber of the mandibular first molar:
- 79. Figure 3716 Periapical granuloma. WEN-defined radiolucency associated with the apex of the maxillary first bicuspid, (Courizsy of Dr‘ Frank Beylot‘tel)
- 80. Figure 3-] er plcal granuloma. Large, well-defined radiolui cency associated with the apices of the mandibular first molar‘ (Courtesy of Dr‘ Robert E. Loy.)
- 81. * Figure 3-24 « Periap al cyst. Wechircumscribed radiolucency intimater associated with the apex of the mandibular central incisor. Note the loss oflamina dura in the area of the lesion
- 82. . . N‘N,§ Figure 3-25 ~ Periapical cyst. Radiolucency associated with the maxillary central incisor, which exhibits significant root resorption.
- 83. Figure 3-36 ' Periapical abscess. Bilateral soft-tissue swelling of the anterior palate.
- 84. figure 3-42 - Parulls. Asymptomatic yellowush nodule of the anurior mandibular alveolar ridge. Adjacent teeth were normal clinically and also asymptomatic
- 85. Figure 3-43 * Periapical abscess. Same patient as depicted in Figure 3742‘ Periapical radiolucency associated with the nonvital mandibular lateral incisor.
- 86. Figure 3 »45 Ludwig's angina. Soft-tissue swelling of the rig?“ submandibular region (Courtesy of Dr‘ Brian Blocher.)
- 87. Figure 3-46 Cellu 5 involving canine space. Erythematous and edematous enlargement of the left side of the face with involvement of the eyelids and conjunctiva. Patients with odonto- genic infections involving the canine space are at risk for cavernous sinus thrombosis. (Courtesy of Dr. Richard Ziegle )
- 88. Figure 348 . Acute osteomyelitis with sequestruml Radior lucency of the right body of the mandible with central radiopaque mass of necrotic bone. (Courtesy of Dr. Michael Meyrowitz.)
- 89. Figure 3-52 t lefuse sclerosmg osteomyelitis. Duffuse area of increased mdiodensity of the right body of the mandible in the tooth-bearing area. No other quadrants were involved (Courtesy of Dr. Louis M. Beta)
- 90. Figure 3753 : Condensing osteitis. Increased areas of radio— density surrounding the apices of the nonvital mandibular first molar.
- 91. Figure 4718 Nifedipine-related gingival hyperp|asia. Diffuse, fibrotic gingival hyperplasia after 1 month ofintensive oral hygiene. Significant erythema, edema, and increased enlargement were present before intervention,
- 92. Figure 4-22 Phenytoin-related ginglval hyperplasia. Significant gingival hyperplasia almost totally covers the crowns of the posterior maxillary dentition (Courtesy of Dr. Ann Drummond and Dr. Timothy Johnson‘)
- 93. 'i-‘gu‘yo 1: 3 , s. Painful erythematous enlargement of the soll tissues overlying the crown of the partially elupted right mandlbular third molar.
- 94. Flgul‘e 5"“ Hutchinson's incisors of congenital syphilis.Den tition exhibiting crowns tapering toward the incisal edges. (me Halstead CL, Blozis CG, Drinnan A], Cier RE: Physicai evaiuntionq' the dental patient. St Louis, 1982, Mosby.)
- 95. Figure 7-31 Mumps. Bilateral parotid enlargement. (From Neville BW. Damm DD, White DK: Color atlas ofclim'ral oml pathology, ed 2, Baltimore, 1999, Williams & Wilkins‘)
- 96. figurafi S Asp rin bur . Extensive area of white epithelial mosisulthe left buccal muwsa caused by aspirin placement in maltempl to alleviate dental pain,
- 97. Figure 8719 Cotton roll burn. Zone ofwhite epithelial ne(rosis and erythema of the maxillary alveolar mucosa.
- 99. F ure 8727 Osteoradionecrosis. Same patient as depicted in Figure 8725. Note fistula formation of the left submandibular area resulting from osteoradionecrosis of the mandibular body.
- 100. K 3'! Amalgam tattoo. Area of mucosal discoloralioml the mandibular alveolar ridge immediately below the bridge politic
- 101. Lg. . 3 Minor aphthous ulcerations. Two ulcerations of different Sizes located on the maxillary labial mucosi
- 102. Figure 9-7 Major aphthous ulcerat on. A, Large ulceration of the left anterior buccal mucosa. B, Same lesion after 5 days of therapy with betamethasone syrup used in a SWIsh—and-swallow method. The patient was free of pain by the second day of therapy. The ulcerahoh healed com- pletely during the foHowmg week‘
- 103. _ Allergic mucosal reaction to systemic drug administration. Large irregular erosion of’tl’le right ventral surr fare of the tongue. The lesion arose secondary to use of oxapmzin, a nonsteroidal antHnflammatory drug.
- 104. Figure 9-33 0 Contact stomatitis from cinnamon flavoring. Oblong area of sensitive erythema with overlying shaggy hyperkeratosis.
- 105. . saw «m %fi¢é’x wa , “a 'r u; n 4: Oral mucosal contact readion to dental amalgam. Radiating pattern of hyperkeratotic striae on the pos- terior buccal mucosa that contacts a large distobuccal amalgam of the permanent mandibular second molar.
- 106. Figure 9740 Angioedema. lefuse upper llp swelling that arose rapidly.