Cadth 2015 e1 2015 04 cadth v2.0
•Download as PPT, PDF•
0 likes•408 views

CADTH 2015 Symposium

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cadth 2015 e1 2015 04 cadth v2.0
Similar to Cadth 2015 e1 2015 04 cadth v2.0 (20)
More from CADTH Symposium
More from CADTH Symposium (20)
Recently uploaded
Recently uploaded (20)
Cadth 2015 e1 2015 04 cadth v2.0
- 1. PANEL SESSION: INTEGRATING EVIDENCE, VALUES AND ETHICS FROM POLICY TO PRACTICE: A MULTICRITERIA REFLECTION A REFLECTION ON ETHICAL DILEMMAS IN HEALTHCARE DECISOBNAKING AND THE ETHICAL FOUNDATIONS OF MCDA April 14tH 2015 CADTH Symposium , Saskatoon Mireille Goetghebeur MEng PhD Global Scientist, LASER Analytica Associate Professor, School of Public health, University of Montreal President EVIDEM Collaboration
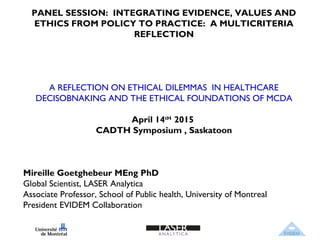
- 2. Efficacy Safety Cost Ethics Quality of evidence Population Priorities Affordability Disease severity Unmet needs Historical context System capacity Expert opinion Patient-reported outcomes Individual perspective www Relying on evidence Relying on social values* Substantive values (CRITERIA - what & why) Procedural values (PROCESS - who & how) Fair and accountable decisionmaking processes** (A4R) Ethical dilemmas Feasibility 2 THE ART OF DECISION MAKING IN HEALTHCARE *Clark and Weale. J Health Org Manag 2012; 26:293; NICE Social Value Judgments 2nd Ed **Daniels and Sabin. Philos Pub Health 1997; 26:305 (4 conditions: Relevance, publicity, revision, leadership). Social valuesCADTH 2015: Suzanne McGurn “Decisions are made with head heart, and hands”
- 3. 3 MCDA - A DEFINITION Definition: Multicriteria decision analysis (MCDA) is an application of analytical methods to explicitly consider multiple criteria
- 4. 4 MCDA – SUPPORTING THE ART OF DECISION MAKING METHODOLOGY 1st STEP OF MCDA – DEFINING OBJECTIVE MCDA mapping EVIDEM Collaboration, a not-for-profit organization developing collaboratively an open source multipurpose MCDA-based approach translated in 10 languages and used throughout the world www.evidem.orgg
- 5. 5 MCDA – STEP 1 - DEFINING OBJECTIVES Common goal: develop & promote interventions that optimize health of patients and populations as well as equitable, sustainable and efficient health care systems Goodness in it widest sense (axiology)
- 6. 6 MCDA – DEFINING SUBSTANTIVE VALUES SUBSTANTIVE VALUES WHAT & WHY
- 7. Ethical dilemmas 7 MCDA – SUBSTANTIVE VALUES Imperative to help - beneficence, non- maleficence (deontology) Greatest good for greatest number (utilitarianism) Prioritizing those who are worst off (fairness, theory of justice); e.g. rare diseases Practical wisdom & goodness (virtue ethics) CADTH 2015: Eduard Hendricks: “Doing what is best”
- 8. Ethical dilemmas 8 Revealed by a holistic perspective Select criteria to encompass all ethical aspects to tackle these dilemmas MCDA – SUBSTANTIVE VALUES
- 9. 9 MCDA – SUBSTANTIVE VALUES Qualitative criteria Disease severity etc DECISION CRITERIA Quantitative criteria Efficacy/effectiveness Safety Etc 2- CRITERIA SELECTION What? Identify all criteria (quantitative and qualitative) that contributes to evaluation of an intervention Why? Realize ethical and methodological implications of criteria selection (signals ) With the goal in mind! METHODOLOGY
- 10. Criteria: Maximize efficacy/effectiveness Maximize safety Maximize patient reported outcomes Type of therapeutic benefit (cure vs symptom relief) Type of preventive benefit - Public health (eradication vs risk reduction) Imperative to help - beneficence, non-maleficence 10 Hippocratic Oath: “I will prescribe for the good of my patients according to my ability and my judgment and never do harm to anyone.” MCDA – SUBSTANTIVE VALUES -CRITERIA Extent of help Type of help Extent of help
- 11. Imperative to help - beneficence, non-maleficence (deontology) 11 Criteria: Alignment with mandate/scope of healthcare system Environmental sustainability MCDA – SUBSTANTIVE VALUES - CRITERIA
- 12. Greatest good for greatest number (utilitarianism) 12 Criteria: Size of population (greatest number) Maximize resources (see Practical wisdom) Opportunity cost and affordability MCDA – SUBSTANTIVE VALUES - CRITERIA
- 13. Prioritizing those who are worst off (fairness, theory of justice) 13 Criteria: Disease severity Unmet needs Established priorities (e.g., vulnerable populations, rare disease) MCDA – SUBSTANTIVE VALUES - CRITERIA
- 14. Virtue ethics &practical wisdom 14 Criteria Relevance and validity of study data Knowledge from experience: clinicians (clinical practice guidelines) & patients Cost of intervention Impact on medical cost Impact on non-medical cost MCDA – SUBSTANTIVE VALUES - CRITERIA Wise use & Devlpt of Knowledge Wise use of resouces & valuing savings
- 15. Virtue ethics & practical wisdom 15 Criteria: awareness of context System capacity and appropriate use of intervention Stakeholders pressures and barriers Political and historical context MCDA – SUBSTANTIVE VALUES - CRITERIA
- 16. 16 MCDA – PROCEDURAL VALUES PRODEDURAL VALUES WHO & HOW Ethics in action
- 17. Developers Align development with systems efficiency, equity and sustainability, and health needs Criteria? Criteria? Criteria? Criteria? Criteria? 17 A COMMON ROAD MAP ACROSS THE DECISION CONTINUUM? Regulators HTA HC Systems Payers Clinicians Patients Who? How? Collaborative development of an holistic criteria set? Unmet needs Perceived health Alleviate sufferingResource allocation Benefit risk Procedural values •Reflective •Systematic •Collaborative •Adaptable to context • Specific goals/mandates • Qualitative/quantitative
- 18. How? Kepner Tregoe (10 pts scale), Point allocation, ranking, Analytical hierarchy process (AHP), Swing Weigths, Discrte choice experiment (DCE) etc Who? Committee members - include the diversity of perspectives 18 MCDA – PROCEDURAL VALUES Procedural values •Participative •Transparent Qualitative criteria Disease severity Etc DECISION CRITERIA Quantitative criteria Relative Weights Efficacy/effectiveness Low High Safety Etc Low High 3-WEIGTHS METHODOLOGY
- 19. DECISION CRITERIA Quantitative criteria Relative Weights Efficacy/effectiveness Low High Safety Etc Low High 19 MCDA – PROCEDURAL VALUES Qualitative criteria Disease severity Turner syndrome: Female specific generic disorder characterized by reduced life expectancy, cardiovascular defects, increased risk of diabetes, absence of puberty, infertility, defects in visuo-spatial organization and non-verbal problem solving, and short stature (details) Etc HIGHLY SYNTHESIZED EVIDENCE How? Evidence modeling, evidence synthesis principles Who? Analysts and communicators 4- EVIDENCE METHODOLOGY Procedural values •Transparent on data •Systematic CADTH 2015, Eduard Hendricks: Address the failure to communicate``
- 20. 20 MCDA – PROCEDURAL VALUES Qualitative criteria Impact Disease severity Turner syndrome: Female specific generic disorder characterized by reduced life expectancy, cardiovascular defects, increased risk of diabetes, absence of puberty, infertility, defects in visuo-spatial organization and non- verbal problem solving, and short stature (details negative neutral positive Etc DECISION CRITERIA Quantitative criteria Relative Weights Efficacy/effectiveness Low High Safety Etc Low High HIGHLY SYNTHESIZED EVIDENCE APPRAISAL Score High Low How? Scoring scales capturing judgment on data (quantum leap) Who? Committee members 5- PERFORMANCE SCORES Sir Rawlins, NICE: “Accept that interpretation of data requires judgement” METHODOLOGY Procedural values •Participatory •Reflective •Transparent on judgment •Systematic
- 21. 21 Max value 1 No value: 0 A B C D Impactofcontext Normative QUANTITATIVE CRITERIA Value *= ∑NWeights x Scores QUALITATIVE CRITERIA High value: Invest Low value: disinvest Feasibility ValueofInterventions A C D B MCDA – PROCEDURAL VALUES CADTH 2015. Jon Witt: “Invest in programs addressing determinants of health” Procedural values •Guide investment/disinvestment based on common goal •Transparent on decision •Holistic
- 22. 22 MULTICRITERIA REFLECTION – FUTURE DIRECTIONS Ethical foundations Methodological foundations Applications & process developments With the goal in mind! Thank you