
Recommended
More Related Content
Similar to Locke intro ekg
Similar to Locke intro ekg (20)
More from Brian Locke
More from Brian Locke (18)
Recently uploaded
Recently uploaded (20)
Locke intro ekg
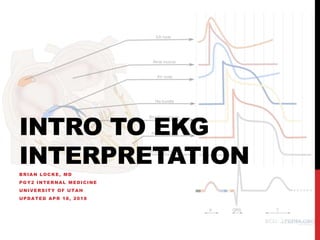
- 1. INTRO TO EKG INTERPRETATION BRIAN LOCKE, MD PGY2 INTERNAL MEDICINE UNIVERSITY OF UTAH UPDATED APR 18, 2018
- 2. OBJECTIVES Understand why ‘the rules’ are what they are. 1. Label the components of an EKG waveform 2. Understand the spatial representation of the different leads 3. Be able to eyeball an estimate of ventricular rate 4. Determine sinus vs. not sinus 5. Determine RBBB vs LBBB vs Neither 6. Identify the morphology of ischemia and infarction
- 3. SOURCES Images from: ecg.utah.edu En.ecgpedia.org https://lifeinthefastlane.com/ecg-library/basics/
- 5. SINGLE LEAD Name the waves:
- 7. APPROACH TO INTERP Methodological approach, every time Numerous variations 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 8. RATE 300 / # big boxes If Irregular: #QRS in 10 seconds (=the strip) * 6 Eg. 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 9. RATE 300 / # small boxes If Irregular: #QRS in 10 seconds (=the strip) * 6 Eg. 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 10. RATE 300 / # small boxes If Irregular: #QRS in 10 seconds (=the strip) * 6 Eg. 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 11. RATE 300 / # small boxes If Irregular: #QRS in 10 seconds (=the strip) * 6 Closer than 3 boxes = tachycardia. Spaced more than 5 boxes = bradycardia 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 12. RHYTHM P-waves? Regular? P QRS? Every QRS preceded by P? *P wave upright in II Eg 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 13. RHYTHM P-waves? Regular? P QRS? Every QRS preceded by P? *P wave upright in II Eg 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 14. RHYTHM P-waves? Regular? P QRS? Every QRS preceded by P? *P wave upright in II Eg 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 15. RHYTHM P-waves? Regular*? P QRS? Every QRS preceded by P? *P wave upright in II Eg 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 16. RHYTHM P-waves? Regular? P QRS? Every QRS preceded by P? *P wave upright in II Eg 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 17. RHYTHM P-waves? Regular? P QRS? Every QRS preceded by P? *P wave upright in II Eg 2 Note: If it’s not sinus, what is it? Another talk: Arrhythmias 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 18. AXIS Recall limb leads: 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 19. LIMB LEADS Limb lead I: + = an impulse moving R to L - = an impulse moving L to R How will a vertical impulse look?
- 20. LIMB LEADS Limb leads I, II, and III:
- 21. LIMB LEADS Augmented limb leads:
- 22. PRECORDIAL LEADS V1 = points toward RV V6 points toward lateral wall
- 23. PRECORDIAL LEADS
- 24. AXIS Definition of Normal Axis : 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 25. AXIS Definition of Normal Axis : 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 26. AXIS E.g. 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 27. AXIS E.g. 1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 28. AXIS E.g. 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 29. AXIS E.g. 2 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 30. AXIS E.g. 3 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 31. AXIS E.g. 3 LAD 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 32. AXIS What situation would have a NW / extreme right / “no-man’s land” axis? 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 33. AXIS What situation would have a NW / extreme right / “no-man’s land” axis? 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 34. CONDUCTION 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology Check intervals PR (?AV Block) QRS duration (?BBB) QTc
- 35. CONDUCTION AV Block 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology 1st Degree Prolonged PR 2nd Degree Type 1 (Wenkebock) PR lengthens, until a QRS is not conducted 2nd Degree Type 2 No PR lengthening prior to non conducted QRS High Degree So many non-conducted QRS that you can’t tell (<2:1) 3rd Degree No conducted QRS complexes (both P-P and QRS-QRS are regular and different)
- 36. CONDUCTION AV Block: At or below the level of the AV-node = risk of becoming complete heart block 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology 1st Degree Prolonged PR 2nd Degree Type 1 (Wenkebock) PR lengthens, until a QRS is not conducted 2nd Degree Type 2 No PR lengthening prior to non conducted QRS High Degree So many non-conducted QRS that you can’t tell (<2:1) 3rd Degree No conducted QRS complexes (both P-P and QRS-QRS are regular and different)
- 37. CONDUCTION Bundle Branch (and fascicle) Blocks – wide QRS (120+ms) Remember the precordial leads V1 = toward RV, V6 = Toward lateral wall 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 38. CONDUCTION Bundle Branch (and fascicle) Blocks RBBB = delayed positive deflection in V1 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 39. CONDUCTION Bundle Branch (and fascicle) Blocks LBBB = Positive Deflection in V6 (Remember, LV size > RV size) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 40. CONDUCTION Bundle Branch (and fascicle) Blocks Meets neither criteria? IVCD (Intraventricular conduction delay) Ventricular Ectopic Beat (e.g. PVC, VT) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 41. MORPHOLOGY Check for: LAA, RAA, RVH / Strain Pattern, LVH, Hypo/hyperkalemia and ischemia 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 42. MORPHOLOGY STEMI = Transmural ischemia from occlusion NSTEMI = Subendocardial ischemia (further from the blood vessel 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 43. MORPHOLOGY An Evolving Infarct 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 44. MORPHOLOGY Ischemia: ST deviation, T-wave inversion Infarct: q-waves (ST Elevation will be) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 45. MORPHOLOGY Ischemia: ST deviation, T-wave inversion Infarct: q-waves (ST Elevation will be) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 46. MORPHOLOGY Ischemia: ST deviation, T-wave inversion Infarct: q-waves (ST Elevation will be) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 47. MORPHOLOGY Ischemia: ST deviation, T-wave inversion Infarct: q-waves (ST Elevation will be) 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology
- 48. EXAMPLE
- 49. EXAMPLE
- 50. EXAMPLE
- 51. MORPHOLOGY A note about LBBB 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology 6. Check Prior
- 52. MORPHOLOGY A note about LBBB: Always have STE – when is it pathologic? Sgarbossa 1. Rate 2. Rhythm 3. Axis 4. Conduction 5. Morphology 6. Check Prior
- 53. PRACTICE
- 54. PRACTICE
- 55. PRACTICE
- 56. PRACTICE
- 57. OBJECTIVES Understand why ‘the rules’ are what they are. 1. Label the components of an EKG waveform 2. Understand the spatial representation of the different leads 3. Be able to eyeball an estimate of ventricular rate 4. Determine sinus vs. not sinus 5. Determine RBBB vs LBBB vs Neither 6. Identify the morphology of ischemia and infarction
- 58. NEXT STEPS Arrythmias ACS management Heart Failure
- 59. RESOURCES Tutorials • http://en.ecgpedia.org • https://lifeinthefastlane.com/ecg-library/basics/ • Also with links to many resources Practice EKGs • https://ecg.bidmc.harvard.edu/ • https://ecg.utah.edu/ • Questions? Brian.locke@hsc.utah.edu
Editor's Notes
- 4 boxes = 75
- 14*6 = 84
- HR 70, normal sinus, LAD (from LAFB), otherwise normal conduction, no signs of ischemia
- *small variation w/ breath
- Aflutter w/ 2:1, 3:1 block
- Einthoven
- Bipolar limb leads (frontal plane): Lead I: RA (-) to LA (+) (Right Left, or lateral) Lead II: RA (-) to LL (+) (Superior Inferior) Lead III: LA (-) to LL (+) (Superior Inferior)
- Augmented unipolar limb leads (frontal plane): Lead aVR: RA (+) to [LA & LL] (-) (Rightward) Lead aVL: LA (+) to [RA & LL] (-) (Leftward) Lead aVF: LL (+) to [RA & LA] (-) (Inferior)
- Unipolar (+) chest leads (horizontal plane): Leads V1, V2, V3: (Posterior Anterior) Leads V4, V5, V6:(Right Left, or lateral)
- Unipolar (+) chest leads (horizontal plane): Leads V1, V2, V3: (Posterior Anterior) Leads V4, V5, V6:(Right Left, or lateral)
- Hint: up in both = normal. If Down in I and Up in II => Reaching towards eachother = RAD. Up in I and down in II = leaving = LAD
- Normal Axis
- Normal Axis
- Rightward axis
- Rightward axis
- Left axis
- Left axis
- Normal Axis
- Normal Axis
- Note: structural abnormality detection is not very sensitive or specific – echo is definitive
- ST depression can be either upsloping, downsloping, or horizontal (see diagram below). Horizontal or downsloping ST depression ≥ 0.5 mm at the J-point in ≥ 2 contiguous leads indicates myocardial ischaemia (according to the 2007 Task Force Criteria). ST depression ≥ 1 mm is more specific and conveys a worse prognosis. ST depression ≥ 2 mm in ≥ 3 leads is associated with a high probability of NSTEMI and predicts significant mortality (35% mortality at 30 days). Upsloping ST depression is non-specific for myocardial ischaemia
- ST elevation is maximal in the anteroseptal leads (V1-4). Q waves are present in the septal leads (V1-2). There is also some subtle STE in I, aVL and V5, with reciprocal ST depression in lead III. There are hyperacute (peaked ) T waves in V2-4. These features indicate a hyperacute anteroseptal STEMI
- Same patient 45 minutes later
- Culprit lesion: RCA sinus bradycardia about 55/min normal conduction intermediate (normal) axis normal p wave morphology tall R in V2, otherwise normal QRS morphology ST elevation in II, III, AVF (in III > II). Depression in I, AVL, V2. Conclusion: Inferoposterior MI caused by a RCA occlusion Arguments in favor of RCA occlusion (instead of RCX): ST depression in I, AVL bradycardia ST elevation in III > II ('the highest ST elevation points at the culprit lesion')
- 75, Normal sinus, normal axis, normal intervals, no ischemia
- LBBB, does not meet sgarbossa
- Diffuse subendocardial ischemia (ST-depression
- RBBB