
Recommended
More Related Content
What's hot
What's hot (20)
Similar to TU Research Day Brandi Poster 2015.03.31
Similar to TU Research Day Brandi Poster 2015.03.31 (20)
TU Research Day Brandi Poster 2015.03.31
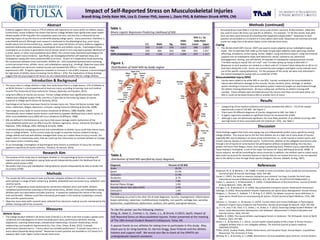
- 1. Measures Methods Ribs 2.4% Fingers 2.4% Hip 2.4% Ankle 16.1% Foot 2.4% Knee 13.7% Thigh 19.4% Lower Leg 3.2% Shoulder 17.7% Cervical Spine 7.3% Thoracic Spine 7.3% Lumbar Spine 3.2% Nose 0.8% Lower Back 1.6% Elbow 0.8% Wrist 2.4% Upper Arm 0.8% Figure 1. Distribution of total MSI by body region Methods (continued) Introduction & Background Abstract Impact of Self-Reported Stress on Musculoskeletal Injuries Brandi Krieg, Emily Kaier MA, Lisa D. Cromer PhD, Joanne L. Davis PhD, & Kathleen Strunk APRN, CNS Research Aim A special thanks to our athletes for taking time to participate in this study. Also, thank you to Dr. Greg Gardner, Dr. Derrick Gragg, Dave Polanski and the athletic trainers and support staff. We would also like to thank all the SPARTA lab undergraduate research assistants. Results Discussion References Table 1. Binary Logistic Regression Predicting Likelihood of MSI To cite this poster use the following citation: Krieg, B., Kaier, E., Cromer, L. D., Davis, J. L., & Strunk, K (2015, April). Impact of Self-Reported Stress on Musculoskeletal Injuries. Poster presented at the meeting of The 18th Annual Student Research Colloquium, Tulsa, OK. • Categorizing of the medical conditions and injuries revealed that 29% (n = 72) of the sample experienced a total of 126 MSI. See Figure 1. • There were 20 different diagnoses of injuries categorized as MSI. See Table 2. • A logistic regression revealed no significant factors for increased risk of MSI. • Although it was not statistically significant, the most likely predictor of an athlete incurring a MSI was high levels of stress associated with the CSALSS (p= .076). See Table 1. • The purpose of this study was to investigate whether or not psychological factors including self- reported stress and maladaptive coping styles would independently predict the likelihood that an athlete would sustain a MSI. • We predict that stress and maladaptive coping behavior would independently be able to predict the occurrence of MSI. These findings suggest that stress and coping may not independently predict injury specificity among college athletes. This may be due to the fact that athletes are at a high risk of many kinds of injuries, especially MSI, due to playing in an injury-prone environment, i.e., acute trauma in contact sports and chronic overuse injuries in noncontact sports. Furthermore, athletes at the collegiate level tend to play through a lot of injuries or come back to full participation without complete healing; this may be a greater risk factor than fatigue, stress, and coping in predicting injury. Previous injury, especially when tissue healing is incomplete, is one of the major risk factors for injury (Whiting & Zernicke, 2008). In future research, we will be controlling for injury chronicity. In addition, the method used to collect injury data could not account for transient injuries or injuries that do not involve time loss or are not reported due to the ability to train through these injuries (Hodgson, Gissane, Gabbett, & King, 2007). Anderson, M. B., & Williams, J. M. (1988). A model of stress and athletic injury: prediction and prevention. Journal of Sport & Exercise Psychology, 10(3), 294-306. Carver, C. (1997). You want to measure coping but your protocol’ too long: Consider the brief cope. International Journal of Behavioral Medicine, 4(1), 92-100. doi: 10.1207/s15327558ijbm0401_6 Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A Global Measure of Perceived Stress. Journal of Health & Social Behavior, 24(4), 385-396. Corrigan, A. B., & Maitland, G. D. (1994). Musculoskeletal and Sports Injuries: Butterworth-Heinemann. Delforge, G. (2002). Musculoskeletal Trauma: Implications for Sports Injury Management: Human Kinetics. Hodgson, L., Gissane, C., Gabbett, T. J., & King, D. A. (2007). For debate: consensus injury definitions in team sports should focus on encompassing all injuries. Clinical Journal of Sport Medicine, 17(3), 188- 191. Johnson, U., Tranaeus, U., & Ivarsson, A. (2014). Current Status and Future Challenges in Psychological Research of Sport Injury Prediction and Prevention. Revista de psicología de deporte, 23(2), 401-409. Lu, F. J.-H., Hsu, Y.-W., Chan, Y.-S., Cheen, J.-R., & Kao, K.-T. (2012). Assessing College Student-Athletes' Life Stress: Initial Measurement Development and Validation. Measurement in Physical Education and Exercise Science, 16(4), 254-267. Nideffer, R. (1983). The injured athlete: psychological factors in treatment. The Orthopedic clinics of North America, 14(2), 373-385. Simon, J. E., & Docherty, C. L. (2013). Current health-related quality of life is lower in former Division I collegiate athletes than in non–collegiate athletes. The American journal of sports medicine, 0363546513510393. TITAN. (2012). Student Health, Athletic Performance, and Education Study: Annual Report. Unpublished Manuscript. The University of Tulsa. Whiting, W. C., & Zernicke, R. F. (2008). Biomechanics of musculoskeletal injury (2nd ed.): Human Kinetics. • The injury rates in college athletes is high. One study found that in a single season, 57% of athletes at an NCAA Division 1 school experienced at least one injury, according to training room and medical records (The University of Tulsa Institute for Trauma, Adversity, and Injustice, 2012). • Long-term effects of injuries are serious. Former college athletes have significantly lower health- related post-collegiate quality of life, and this is in part due to the enduring impact of injuries sustained in college sports (Simon & Docherty, 2013). • Psychological risk factors have been found to increase injury risk. These risk factors include: high stress, inattention, fatigue, depression, and poor coping resources (Whiting & Zernicke, 2008). • Psychological stress leads to muscle tension (Anderson & Williams, 1988; Nideffer, 1983). Theoretically, stress-related muscle tension could lead to a greater likelihood that a strain, sprain, or other musculoskeletal injury (MSI) will occur (Anderson & Williams, 1988). • MSI are defined in the literature as any injury that causes damage and/or dysfunction of the musculoskeletal system and can affect muscles, tendons, ligaments, nerves, and bones (Corrigan & Maitland, 1994; Delforge, 2002; Whiting & Zernicke, 2008). • Understanding and managing precursors and vulnerabilities to athletic injury could help reduce injury rates in college athletes. In the current study, we sought to examine stresses related to being a college athlete and how well athletes managed their stress as it relates these to injury records. Our hope is that if a relationship exists, that we could use this information to motivate athletes to manage and reduce stress in healthy ways. • To our knowledge, investigation of psychological stress factors as predictors of injury has not been applied to specificity of injuries (Johnson, Tranaeus, & Ivarsson, 2014). • Perceived Stress Scale (PSS) is a 10-item stress scale (Cohen, Kamarck, & Mermelstein, 1983) that was used to assess life stress non-specific to athletics. For example, “In the last month, how often have you been upset because of something that happened unexpectedly?” Responses to each question are provided on a 0 (never) to 4 (very often) Likert scale. Responses are summed and total scores can range from 0-40 where higher scores indicate more stress. Coping • The 28-item Brief COPE (Carver, 1997) was used to assess adaptive versus maladaptive coping styles. The 14 subscales that make up the styles include eight adaptive styles (planning, positive reframing, acceptance, active coping, humor, religion, using emotional support, using instrumental support) and six maladaptive styles (self-distraction, denial, substance use, behavioral disengagement, venting, and self-blame). An example of maladaptive coping questions include: “I’ve been saying to myself ‘this isn’t real’” and “I’ve been giving up trying to deal with it.” Responses to each question are ranked on a Likert scale of 1 (I haven’t been doing this at all) to 4 (I have been doing this a lot). Scores are summed by each category and higher scores indicate more use of the specific coping behavior(s). For the purposes of this study, we were only interested in the overall maladaptive coping style as a predictor of MSI. Musculoskeletal Injury (MSI) • Injuries were coded to be either MSI or non-MSI. Injuries considered to be musculoskeletal in nature were defined as damage to the muscles, nerves, tendons, joints, cartilage, or skeletal system resulting in time loss from participation and/or treatment sought out and treated through the athletic training department. All injury coding was verified by an athletic training staff member. Eleven athletes were excluded because the injuries that they incurred were either not MSI or could not be determined as MSI or another form of injury. Evidence suggests that as many as 57% of athletes will experience an injury within an athletic season. Furthermore, recent evidence has shown that former college athletes have significantly lower health- related quality of life long after the competition years are over, and that this is influenced by the enduring impact of injuries that occurred while playing college sports. Injury prevention, therefore, is a worthwhile pursuit. Although most research is dedicated to the physiological (e.g., prior injury, health status) and environmental (e.g., weather, sport type) risk factors of injury, evidence suggests a potential relationship exists between psychological stress and athletic injuries. Psychological stress could lead to an increase in generalized muscle tension which in turn may lead to greater likelihood of a strain, sprain, or other musculoskeletal injury (MSI). The current study examined psychological risk factors for sport injury incidence. Specifically, we investigated whether self-reported stress and maladaptive coping with stress predicted MSI occurrence. As part of a longitudinal study examining the connections between stress and health, athletes (N = 245) completed questionnaires assessing current perceived stress, athletic stress, and maladaptive coping (e.g., drinking). Objective injury data were collected from electronic medical records and revealed that 29% (n = 72) of the sample experienced a MSI. A logistic regression revealed no increase in risk of MSI; however, a trend emerged for high levels of athletic stress increasing risk for MSI (p = .076). The implications of these findings suggest that the psychological risk factors do not independently predict MSI for college athletes. • The sample (N=245) consisted of male and female collegiate athletes of a Division I university participating in a range of both contact (e.g. football, basketball) and noncontact (e.g. volleyball, cross country) sports. • As part of a longitudinal study examining the connections between stress and health, athletes completed questionnaires assessing current perceived stress, athletic stress, and maladaptive coping. Athletes were recruited before and after practices. A researcher explained the nature of the study, risks and benefits. Athletes could then voluntarily participate in the study by completing a consent form and the questionnaires. • Objective injury data (with consent) were collected from electronic medical records maintained by the athletic training staff of the university. S.E. Wald Sig. Odds Ratio 95% C.I. for Odds Ratio Lower Upper CSALSS .010 3.159 .076 1.017 .998 1.057 PSS .029 .004 .952 .998 .943 1.057 COPE (maladaptive) .035 1.526 .217 1.044 .975 1.117 Table 2. Distribution of total MSI specified by injury diagnosis Athletic Stress • The College Student Athlete’s Life Stress Scale (CSALSS) is a 24-item scale that includes a global score comprised of 8 subcategories of stress including sport injury, performance demand, training adaptations, coaching relationships, interpersonal relationships, romantic relationships, family relationships, and academic requirements (Lu, Hsu, Chan, Cheen, & Kao, 2012). A sample performance demand item is: “I worry about my unstable performance.” A sample injury item is: “I worry about frequently being injured.” Responses to each question are provided on a 0 (never) to 5 (always) Likert scale; higher scores indicate more stress. Diagnosis Percent of All MSI Strain 26.2% Sprain 25.4% Contusion 11.9% Tendonitis 8.7% Spasm(s) 7.9% Brachial Plexus Stinger 5.6% Glenoid Labrum Tear (Non-SLAP) 2.4% Dislocation 1.6% Fracture 1.6% The following occurred in less than 1% of total diagnoses: bursitis, impingement, inflammation (lower extremity), labral tear, multidirectional instability, non-specific cartilage tear, sacroiliac dysfunction, scaplothoracic dysfunction, scoliosis, shin splints, and spinal stenosis.