1. INTRODUCTION
DISCUSSION
Neuroplastic Changes after Auditory Working Memory Training in A Patient Surviving Multiple Strokes
Benson
P.
S.
Ng1,
Xianzhi
Chen1,
Carmen
Tuchak3,
Masako
Miyazaki3,
Darcy
BuBerworth3,
Joanne
Martens3,
Rhondda
Jones3,
Ada
W.
S.
Leung1,2,3
1Department
of
OccupaMonal
Therapy,
University
of
Alberta,
Canada;
2Centre
for
Neuroscience,
University
of
Alberta;
3Glenrose
RehabilitaMon
Hospital,
Edmonton,
Alberta,
Canada.
Stroke
paMents
exhibit
a
wide
range
of
cogniMve
deficits
including
working
memory
(van
Geldorp
et
al.,
2013).
Working
memory
refers
to
the
ability
to
maintain
and
manipulate
a
limited
amount
of
informaMon
for
goal-‐directed
acMon
(Baddeley,
1986).
Previous
studies
have
shown
that
working
memory
ability
measured
at
the
early
phase
of
cogniMve
rehabilitaMon
is
predicMve
of
funcMonal
gains
a^er
stroke
(Leung
et
al.,
2010).
However,
it
is
unclear
how
working
memory
training
induces
neuroplasMc
changes
in
paMents
surviving
a
stroke.
Understanding
the
underlying
neural
mechanisms
associated
with
working
memory
training
will
provide
insights
into
training
regimens,
transfer
effects
and
potenMal
benefits
for
stroke
paMents.
Case
History
–
The
paMent,
KB,
was
a
39
year-‐old
right-‐handed
male
who
suffered
an
acute
right
subdural
hematoma,
involving
frontal
and
parietal
lobes,
as
well
as
the
ipsilateral
tentorium
cerebelli.
During
the
operaMon,
KB
suffered
mulMple
cerebrovascular
accidents
(CVAs)
in
the
bilateral
posterior
cerebral
artery
(PCA)
and
bilateral
anterior
cerebral
artery
(ACA)
territories.
The
paMent
had
corMcal
blindness
and
le^
hemiparesis,
but
did
not
demonstrate
significant
aphasia
and
did
not
suffer
from
other
neurological
or
psychiatric
diseases.
At
the
Mme
of
the
study,
KB
was
two
years
post-‐stroke
and
demonstrated
short-‐term
memory
impairment
as
well
as
persistent
working
memory
and
execuMve
dysfuncMon
problems.
This
single
case
report
explored
the
neuroplasMc
changes
associated
with
auditory
working
memory
training
for
seven
consecuMve
weeks.
We
found
that
KB
showed
improved
task
performance
throughout
training
and
demonstrated
improvement
on
cogniMve
abiliMes
including
aBenMon,
working
memory
and
short-‐term
memory
a^er
the
training.
Pre-‐
and
Post-‐Training
Assessment
–
Neuropsychological
assessments
included
subtests
from
the
Wechsler
Memory
Scale-‐
Third
EdiMon:
Digit
span
forward
and
digit
span
backward.
Two
subtests
from
the
Test
of
Everyday
ABenMon
(TEA)
were
also
administered:
The
Elevator
CounMng
with
DistracMon
(ECD)
and
the
Elevator
CounMng
with
Reversal
(ECR).
N-‐BACK
TASKS
PERFORMANCE
METHOD
REFERENCES
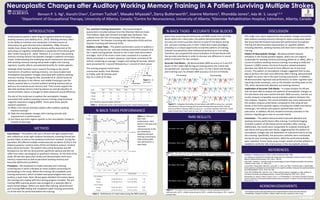
Figure
2
-‐
Plot
of
n-‐
back
task
performance.
Data
points
in
the
grey
area
represent
measurements
at
the
pre-‐training
(ie.
baseline)
and
post
training
assessments.
Only
training
data
was
obtained
for
3-‐
back
tasks.
N-‐BACK
TASKS
-‐
ACCURATE
TASK
BLOCKS
Baddeley A. Working memory. Oxford: Oxford University Press; 1986.
van Geldorp B, Kessels RP, Hendriks MP. Single-item and associative working memory in stroke
patients. Behavioral Neurology. 2013; 26(3): 199-201.
Kelly AMC, Garaven H. Human functional neuroimaging of brain changes associated with practice.
Cerebral Cortex. 2005; 15: 1089-1102.
Leung AWS, Cheng SKW, Mak AKY, Leung KK, Li LSW, Lee TMC. Functional gain in hemorrhagic
stroke patients is predicted by functional level and cognitive abilities measured at hospital admission.
NeuroRehabilitation. 2010; 27(4): 351-358.
Owen AM, McMillan KM, Laird AR, et al. N-back working memory paradigm: a meta- analysis of
normative functional neuroimaging studies. Human Brain Mapping. 2005; 25(1): 46-59.
Schneiders JA, Opitz B, Tang H, Deng Y, Xie C, Li H, Mecklinger A. The impact of auditory working
memory training on the fronto-parietal working memory network. Frontiers in Human Neuroscience.
2012; 6(173): 1-14.
ACKNOWLEDGEMENTS
This research project was supported by the Clinical Research Grants from the Glenrose
Rehabilitation Hospital Foundation, Alberta Health Services, awarded to Ada Leung.
Figure
1
-‐
N-‐
back
task.
Although
there
has
been
much
research
focusing
on
the
neural
mechanisms
of
auditory
working
memory,
not
many
studies
have
invesMgated
neuroplasMc
changes
associated
with
auditory
working
memory
training.
Among
the
few,
Schneider
et
al.
(2012)
found
an
acMvaMon
decrease
in
the
inferior
and
middle
frontal
gyri
and
the
inferior
parietal
lobe
in
a
trained
auditory
working
memory
task
as
well
as
a
non-‐trained
visual
memory
task.
Their
results
support
the
idea
that
working
memory
training
induces
an
overall
reducMon
of
neural
acMviMes,
which
is
thought
to
index
enhanced
neural
efficiency.
The
aim
of
this
study
was
to
explore
the
neuroplasMc
changes
associated
with
auditory
working
memory
training
using
funcMonal
magneMc
resonance
imaging
(fMRI).
There
were
three
specific
research
quesMons:
(1) What
is
the
neural
acMvaMon
paBern
a^er
auditory
working
memory
training?
(2) Does
the
neuroplasMc
changes
with
training
coincide
with
improvement
in
performance?
(3) Are
there
any
brain
regions
specific
to
the
neuroplasMc
change
or
transfer
of
learning?
Auditory
n-‐back
Tasks
–
The
paMent
performed
a
series
of
auditory
n-‐
back
tasks
during
the
pre-‐
and
post-‐training
assessment
sessions
and
the
7-‐week
training
period.
SMmuli
for
the
n-‐back
tasks
were
leBers
and
digits.
Each
of
the
three
n-‐back
tasks
consisted
of
a
number
of
blocks
presented
in
a
random
sequence.
Each
block
consisted
of
30
sMmuli,
containing
on
average
7
targets
and
lasMng
60
seconds.
SMmuli
were
presented
for
1
second
followed
by
a
1
second
of
silent
pause.
The
training
program
lasted
seven
consecuMve
weeks,
from
Monday
to
Friday,
with
30
minutes
each
day,
for
a
total
of
35
days.
Table
1
-‐
Distribu@on
of
the
n-‐back
tasks
during
the
7-‐week
training
period.
Figure
4
-‐
Pair-‐wise
t-‐test
on
all
task
blocks
the
pre-‐training
and
the
post-‐training
scans.
IFG
=
inferior
frontal
gyrus;
IPL
=
inferior
parietal
lobe;
SPL
=
superior
parietal
lobe.
Figure
5
-‐
Pair-‐wise
t-‐test
on
accurate
task
blocks
in
the
pre-‐training
and
the
post-‐
training
scans.
MTG
=
middle
temporal
gyrus;
MFG
=
middle
frontal
gyrus;
SPL
=
superior
parietal
lobe.
Table
2
-‐
Performance of n-back tasks during the fMRI scanning.
Pa8ern
of
Neuroplas=c
Change
–
KB
demonstrated
reduced
acMvaMon
in
the
frontal-‐parietal
regions,
which
are
core
regions
responsible
for
working
memory
processing
(Owen
et
al,
2005),
a^er
a
course
of
auditory
working
memory
training.
According
to
Kelly
and
Garavan’s
(2005)
review,
this
kind
of
pracMce-‐related
acMvaMon
decrease
was
likely
the
result
of
more
efficient
use
of
neuronal
circuits.
This
paBern
of
neuroplasMc
changes
suggested
that
he
was
able
to
perform
the
task
more
efficiently
a^er
training,
demonstrated
by
higher
accuracy
rate
in
the
post-‐training
assessment.
In
addiMon,
KB
demonstrated
improved
task
performance
on
other
cogniMve
tasks
requiring
similar
processes,
such
as
the
elevator
counMng
tasks
on
the
TEA,
which
demand
both
aBenMon
and
working
memory.
Implica=on
of
Accurate
Task
Blocks
–
A
unique
analysis
for
KB
was
that
we
were
able
to
analyze
the
paBerns
of
neuroplasMc
changes
on
the
task
blocks
that
were
performed
with
100%
accuracy.
Overall,
our
results
showed
comparable
neural
acMvaMon
paBerns
between
the
two
analyses.
However,
the
neural
acMvaMon
was
more
extensive
for
the
analysis
using
accurate
blocks
compared
to
that
using
all
task
blocks
in
the
fronto-‐parietal
regions
including
the
middle
and
inferior
frontal
gyri,
the
inferior
and
superior
parietal
lobes
and
the
precuneus.
In
addiMon,
KB
also
showed
increased
acMvaMon
in
the
anterior
cingulate
gyrus
only
on
accurate
blocks.
Conclusion
–
The
paMent
demonstrated
improved
aBenMon
and
working
memory
performance
a^er
training.
FuncMonal
imaging
revealed
a
paBern
of
decreased
neural
acMvaMon
a^er
training.
AddiMonally,
the
results
were
comparable
for
analyses
involving
all
task
blocks
and
accurate
task
blocks,
suggesMng
that
the
paBern
of
neuroplasMc
changes
was
not
dependent
on
task
performance
during
the
scanning.
Specifically,
the
precuneus
acMviMes
were
maintained
during
the
post-‐training
assessment,
albeit
the
prefrontal
acMviMes
were
subsided.
Future
study
using
a
larger
sample
of
stroke
paMents
is
needed
to
verify
the
role
of
precuneus
in
the
neuroplasMc
process.
Procedure
–
KB
completed
an
intake
interview
and
a
hearing
screening
test
in
which
indicated
an
intact
auditory
processing
for
parMcipaMng
in
the
study.
Before
the
training,
KB
completed
a
pre-‐
training
assessment,
which
included
neuropsychological
tests
and
auditory
n-‐back
tasks.
Next,
KB
was
given
detailed
informaMon
about
the
training
and
a
laptop
with
the
training
program
installed.
The
pre-‐
training
fMRI
scanning
session
was
arranged
on
a
separate
date
to
avoid
mental
faMgue.
Within
one
week
a^er
training,
KB
performed
post-‐training
fMRI
tesMng
and
completed
a
post-‐training
assessment
on
all
the
tests
he
performed
before
the
training.
Figure
3
-‐
A
diagram
illustra@ng
the
task
blocks
with
100%
accuracy
(i.e.,
accurate
task
blocks)
on
the
pre-‐training
and
the
post-‐training
scanning
sessions.
Colored
blocks
are
blocks
showing
100%
accuracy
(i.e.,
no
misses
and
false
alarm)
for
1-‐back
tasks
(in
blue)
and
2-‐back
tasks
(in
red);
1B
=
1-‐back
task;
2B
=
2-‐back
task.
Apart
from
examining
the
behavioral
and
fMRI
results
from
all
of
the
blocks
within
the
n-‐back
tasks,
the
paMent
demonstrated
100%
accuracy
(no
misses
and
false
alarms)
in
some
of
the
blocks
during
pre-‐
and
post-‐training
scans
in
both
1-‐back
and
2-‐back
paradigms,
providing
us
a
unique
opportunity
to
examine
paBerns
of
training-‐
induced
neuroplasMcity
when
behavioral
performance
is
at
ceiling.
Therefore,
we
compared
the
neural
acMvaMon
of
all
task
blocks
with
the
accurate
task
blocks
in
order
to
discover
any
difference
in
neural
paBerns
between
the
two
analyses.
fMRI
RESULTS
Accurate
Task
Blocks
–
KB
demonstrated
100%
accuracy
on
5
out
of
9
blocks
in
the
1-‐back
task
during
pre-‐training
and
in
the
2-‐back
task
during
both
pre-‐
and
post-‐training
scans.
For
the
1
block
task
during
post-‐training
scan,
he
showed
100%
accuracy
on
6
out
of
9
blocks.