
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cleft lip and palate.ppt
Similar to Cleft lip and palate.ppt (20)
More from Amina Rajah
Recently uploaded
Recently uploaded (20)
Cleft lip and palate.ppt
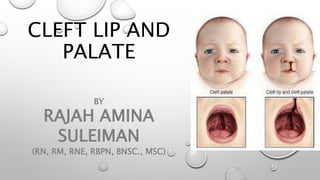
- 1. CLEFT LIP AND PALATE BY RAJAH AMINA SULEIMAN (RN, RM, RNE, RBPN, BNSC., MSC)
- 2. INTRODUCTION • Craniofacial birth defects are the fourth most common congenital anomaly in newborns. • Cleft lip and palate together represent the most common congenital deformity of the head and the neck.
- 3. EMBRYOLOGY OF THE FACE • The external human face develops between the 4th and 6th week of embryonic development. • There are two important tissue structures involved in development of the face and its structures – the pharyngeal arches and neural crest cells. • Six pharyngeal arches arise in the fourth week of development as out-pocketings of mesoderm on both sides of the pharynx.
- 4. EMBRYOLOGY OF THE FACE • The lips and palate originate from three areas of the baby’s developing face: • Central or frontal nasal prominence: normally grows to become the forehead, nose, middle portion of the upper lip (philtrum or cupid’s bow) and the primary palate (part of the upper jaw that holds the middle four teeth) • Left and right maxillary prominences: grow and become the lower face, lower lip and jaw, all but the middle portion of upper lip and jaw, and the secondary palate (behind the four upper middle teeth to back of mouth.
- 5. EMBRYOLOGY OF THE PALATE • Between the 6th and 8th week, the palate begins to develop. • Prior to palate formation, the tongue is high and in the area of the nasal cavity. The palatal shelves are vertical and positioned on each side of the tongue. • Around the seventh or eighth week of gestation, the tongue begins to gradually drop down. When this occurs, the palatal shelves move slowly from a vertical to a horizontal position and fuse, first with the premaxilla at the incisive foramen, and then with each other.
- 6. EMBRYOLOGY OF THE LIPS • The lips forms from initially freely projecting maxillary, medial nasal, and lateral nasal prominences at the rostral and lateral boundaries of the primitive oral cavity. • Initial fusion is between lateral and medial nasal processes and is followed by fusion between maxillary and medial nasal processes.
- 7. ANATOMY OF THE LIP
- 8. ANATOMY OF THE PALATE
- 9. DEFINITION OF TERMS • Cleft: A cleft is any opening or division in some part of the anatomy that is not normally open or divided. • Cleft lip – cleft lip is defined as a gap between the philtrum and the lateral upper lip which occurs when the medial nasal prominence and maxillary prominence fail to fuse. • Cleft palate – is defined as a gap in the palate due to partial or total lack of fusion of palatal shelves as a result of defective growth of palatal shelves, failure of the shelves to attain a horizontal position, lack of contact between shelves or rupture after fusion of shelves.
- 10. EPIDEMIOLOGY • Worldwide, oral clefts in any form (i.E., Cleft lip, cleft lip and palate, or isolated cleft palate) occur in about one in every 700 live births (world health organization [WHO], 2011). • International estimates that are limited to cleft lip with or without cleft palate range from 7.94 to 9.92 per 10,000 live births.
- 11. ETIOLOGY • There is no one cause of cleft lip and palate. However, most cases are thought to result from multifactorial inheritance—an interaction between the person's genes (genetic predisposition) and specific environmental factors. Risk factors that increase the likelihood of cleft lip and palate include the following: • Strong family history of cleft lip and palate • Race—cleft lip and palate are more common in asians and native americans than in african americans. • Sex—males are more likely to have cleft lip with or without cleft palate; females are more likely to have cleft palate without cleft
- 12. ETIOLOGY • Exposure to certain environmental substances, such as tobacco and alcohol, prescription drugs, and illegal drugs • Diabetes mellitus • Obesity • Lack of folic acid supplementation • Medications taking during pregnancy such as anti- seizure/anticonvulsant drugs, acne drugs containing accutane, and methotrexate, a drug commonly used for treating cancer, arthritis, and psoriasis. • Advanced parental age • Maternal viral infections
- 13. CLASSIFICATION OF CLEFT LIP • Forme fruste unilateral cleft lip (microform). A subtle cleft on one side of the upper lip, which may appear as a small indentation. • Incomplete unilateral cleft lip. • Complete unilateral cleft lip. • Incomplete bilateral cleft lip. • Complete bilateral cleft lip.
- 16. CLASSIFICATION OF CLEFT PALATE
- 17. SYNDROMES ASSOCIATED WITH CLEFT LIP AND PALATE • Common syndromes involving cleft palate are apert syndrome, stickler syndrome and treacher-collins syndrome. Van der woude and waardenburg syndromes are examples of syndromes with cleft lip with or without cleft palate.
- 18. PROBLEMS ASSOCIATED CLEFT LIP AND PALATE • Psychosocial • Feeding • Airway infection • Middle ear infection • Speech problem • Dental anomalies
- 19. SURGICAL MANAGEMENT • The first procedure that cleft patients receive is surgical closure of the lip. • Following the “rule of 10s,” a patient admitted for lip closure should be 10 weeks of age, weigh at least 10 pounds (4.5 kg), have a hemoglobin ≥10mg/dl, and have WBC count >10,000cu/mm in order to withstand surgery and anesthesia.
- 20. SURGICAL MANAGEMENT • Pre-surgical orthopedics may be used to move cleft segments closer together and into better alignment prior to surgical repair. These include • Lip taping; • Lip adhesion; • Nasoalveolar molding (NAM) appliances; and • Devices attached by pins and screws that force alignment of maxillary segments.
- 22. SURGICAL MANAGEMENT Surgeries can include one or more of the following: • Repair of cleft lip (usually performed within the first 6 months of life) • Repair of cleft palate (usually by 12 months of age in a child with typical development) • Repair of submucous cleft palate • Tonsillectomy and/or adenoidectomy (may be needed prior to pharyngeal flap or other pharyngoplasty) • Secondary surgeries to repair palatal fistulae (if symptomatic) • Alveolar bone grafting (determined by stage of dental development and in collaboration with orthodontist)
- 23. NURSING MANAGEMENT • Nursing management • Maintain adequate nutrition. • Positioning. If the cleft lip is unilateral, the nipple should be aimed at the unaffected side; the infant should be kept in an upright position during feeding. • Tools for feeding. Lamb’s nipples (extra long nipples) and special cleft palate nipples molded to fit into the open palate area to close the gap may be used; promote family coping. • Reduce family anxiety. • Provide family teaching.
- 24. NURSING DIAGNOSIS • Ineffective airway clearance related to tracheobronchial aspiration of feedings evidenced by dyspnea • Imbalanced nutrition: less than body requirements related to difficulty in sucking evidenced by underweight • Compromised family coping related to visible physical defect. • Anxiety of family caregivers related to child’s condition and surgical outcome evidenced by expression of guilt, blame, and helplessness. • Deficient knowledge of family caregivers related to care of child before surgery and the surgical procedure evidenced by request for information about cause of defects, feeding techniques
- 25. NURSING DIAGNOSIS • Post-op • Ineffective breathing pattern related to anatomical changes. • Acute pain related to surgical procedure. • Risk for deficient fluid volume related to npo status after surgery. • Risk for aspiration related to a reduced level of consciousness after surgery.
- 28. NOVEMBER 2017, PAPER I, question 3 Master ifeanyi, a 10-week old boy is admitted into the children’s ward with cleft lip and palate. He is scheduled for cleft lip repair • Describe the pre and post-operative care of master ifeanyi (7 marks) • State six (6) predisposing factors to cleft lip and palate (3 marks) • NOVEMBER, 2018, PAPER II, question 4 Write concisely on the following • Embryology of the face • The problems of a child with cleft palate (4 marks)
- 29. NOVEMBER 2020 PAPER II, question 3 Baby nneka is booked for cleft palate repair in your hospital. • Highlight the necessary investigations needed before and after the surgery (4 marks) • Discuss the importance of mędical photograph in the management of congenital abnormalities (5 marks) • Develop a nursing care plan to solve three (3) nursing diagnoses of baby nkechi (9 marks) • Enumerate four (4) surgical complications of cleft lip repairs (2 marks)