
Recommended
More Related Content
Similar to DisabilityTitle I and Title V of the Americans with Disabilities
Similar to DisabilityTitle I and Title V of the Americans with Disabilities (18)
More from AlyciaGold776
More from AlyciaGold776 (20)
Recently uploaded
Recently uploaded (20)
DisabilityTitle I and Title V of the Americans with Disabilities
- 1. Disability Title I and Title V of the Americans with Disabilities Act of 1990, as amended, protect qualified individuals from discrimination on the basis of disability in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Disability discrimination includes not making reasonable accommodation to the known physical or mental limitations of an otherwise qualified individual with a disability who is an applicant or employee, barring undue hardship. Age The Age Discrimination in Employment Act of 1967, as amended, protects applicants and employees 40 years of age or older from discrimination based on age in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Sex (Wages) In addition to sex discrimination prohibited by Title VII of the Civil Rights Act, as amended, the Equal Pay Act of 1963, as amended, prohibits sex discrimination in the payment of wages to women and men performing substantially equal work, in jobs that require equal skill, effort, and responsibility, under similar working conditions, in the same establishment. Genetics Title II of the Genetic Information Nondiscrimination Act of 2008 protects applicants and employees from discrimination based on genetic information in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. GINA also restricts employers’ acquisition of genetic information and strictly limits disclosure of genetic information. Genetic information includes information about genetic tests of applicants, employees, or their family members; the manifestation of diseases or disorders in family members (family medical history); and requests for or
- 2. receipt of genetic services by applicants, employees, or their family members. Retaliation All of these Federal laws prohibit covered entities from retaliating against a person who files a charge of discrimination, participates in a discrimination proceeding, or otherwise opposes an unlawful employment practice. What to Do If You Believe Discrimination Has Occurred There are strict time limits for filing charges of employment discrimination. To preserve the ability of EEOC to act on your behalf and to protect your right to file a private lawsuit, should you ultimately need to, you should contact EEOC promptly when discrimination is suspected: The U.S. Equal Employment Opportunity Commission (EEOC), 1-800-669-4000 (toll-free) or 1-800-669-6820 (toll-free TTY number for individuals with hearing impairments). EEOC field office information is available at www.eeoc.gov or in most telephone directories in the U.S. Government or Federal Government section. Additional information about EEOC, including information about charge filing, is available at www.eeoc.gov. Employers Holding Federal Contracts or Subcontracts Applicants to and employees of companies with a Federal government contract or subcontract are protected under Federal law from discrimination on the following bases: Race, Color, Religion, Sex, National Origin Executive Order 11246, as amended, prohibits job discrimination on the basis of race, color, religion, sex or national origin, and requires affirmative action to ensure equality of opportunity in all aspects of employment. Individuals with Disabilities Section 503 of the Rehabilitation Act of 1973, as amended, protects qualified individuals from discrimination on the basis of disability in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Disability discrimination includes not making
- 3. reasonable accommodation to the known physical or mental limitations of an otherwise qualified individual with a disability who is an applicant or employee, barring undue hardship. Section 503 also requires that Federal contractors take affirmative action to employ and advance in employment qualified individuals with disabilities at all levels of employment, including the executive level. Disabled, Recently Separated, Other Protected, and Armed Forces Service Medal Veterans The Vietnam Era Veterans’ Readjustment Assistance Act of 1974, as amended, 38 U.S.C. 4212, prohibits job discrimination and requires affirmative action to employ and advance in employment disabled veterans, recently separated veterans (within three years of discharge or release from active duty), other protected veterans (veterans who served during a war or in a campaign or expedition for which a campaign badge has been authorized), and Armed Forces service medal veterans (veterans who, while on active duty, participated in a U.S. military operation for which an Armed Forces service medal was awarded). Retaliation Retaliation is prohibited against a person who files a complaint of discrimination, participates in an OFCCP proceeding, or otherwise opposes discrimination under these Federal laws. Any person who believes a contractor has violated its nondiscrimination or affirmative action obligations under the authorities above should contact immediately: The Office of Federal Contract Compliance Programs (OFCCP), U.S. Department of Labor, 200 Constitution Avenue, N.W., Washington, D.C. 20210, 1-800-397-6251 (toll-free) or (202) 693-1337 (TTY). OFCCP may also be contacted by e-mail at [email protected], or by calling an OFCCP regional or district office, listed in most telephone directories under U.S. Government, Department of Labor. Programs or Activities Receiving Federal Financial Assistance Race, Color, National Origin, Sex
- 4. In addition to the protections of Title VII of the Civil Rights Act of 1964, as amended, Title VI of the Civil Rights Act of 1964, as amended, prohibits discrimination on the basis of race, color or national origin in programs or activities receiving Federal financial assistance. Employment discrimination is covered by Title VI if the primary objective of the financial assistance is provision of employment, or where employment discrimination causes or may cause discrimination in providing services under such programs. Title IX of the Education Amendments of 1972 prohibits employment discrimination on the basis of sex in educational programs or activities which receive Federal financial assistance. EEOC 9/02 and OFCCP 8/08 Versions Useable With 11/09 Supplement Individuals with Disabilities Section 504 of the Rehabilitation Act of 1973, as amended, prohibits employment discrimination on the basis of disability in any program or activity which receives Federal financial assistance. Discrimination is prohibited in all aspects of employment against persons with disabilities who, with or without reasonable accommodation, can perform the essential functions of the job. If you believe you have been discriminated against in a program of any institution which receives Federal financial assistance, you should immediately contact the Federal agency providing such assistance. Disability Title I and Title V of the Americans with Disabilities Act of 1990, as amended, protect qualified individuals from discrimination on the basis of disability in hiring, promotion, discharge, pay, fringe benefits, job training, classification,
- 5. referral, and other aspects of employment. Disability discrimination includes not making reasonable accommodation to the known physical or mental limitations of an otherwise qualified individual with a disability who is an applicant or employee, barring undue hardship. Age The Age Discrimination in Employment Act of 1967, as amended, protects applicants and employees 40 years of age or older from discrimination based on age in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Sex (Wages) In addition to sex discrimination prohibited by Title VII of the Civil Rights Act, as amended, the Equal Pay Act of 1963, as amended, prohibits sex discrimination in the payment of wages to women and men performing substantially equal work, in jobs that require equal skill, effort, and responsibility, under similar working conditions, in the same establishment. Genetics
- 6. Title II of the Genetic Information Nondiscrimination Act of 2008 protects applicants and employe es from discrimination based on genetic information in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. GINA also restricts employers’ acquisition of genetic information and strict ly limits disclosure of genetic information. Genetic information includes information about genetic tests of applicants, employees, or their family members; the manifestation of diseases or disorders in family members (family medical history); and requests for or receipt of genetic services by applicants, employees, or their family members. Retaliation All of these Federal laws prohibit covered entities from retaliating against a person who files a charge of discrimination, participates in a discrimination proceeding, or otherwise opposes an unlawful employment practice. What to Do If You Believe Discrimination Has Occurred There are strict time limits for filing charges of employment discrimination. To preserve the ability of EEOC to act on your behalf and to protect your right to file
- 7. Disability Title I and Title V of the Americans with Disabilities Act of 1990, as amended, protect qualified individuals from discrimination on the basis of disability in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Disability discrimination includes not making reasonable accommodation to the known physical or mental limitations of an otherwise qualified individual with a disability who is an applicant or employee, barring undue hardship. Age The Age Discrimination in Employment Act of 1967, as amended, protects applicants and employees 40 years of age or older from discrimination based on age in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. Sex (Wages) In addition to sex discrimination prohibited by Title VII of the Civil Rights Act, as amended, the Equal Pay Act of 1963, as amended, prohibits sex discrimination in the payment of wages to women and men performing substantially equal work, in jobs that require equal skill, effort, and responsibility, under similar working conditions, in the same establishment. Genetics Title II of the Genetic Information Nondiscrimination Act of 2008 protects applicants and employees from discrimination based on genetic
- 8. information in hiring, promotion, discharge, pay, fringe benefits, job training, classification, referral, and other aspects of employment. GINA also restricts employers’ acquisition of genetic information and strictly limits disclosur e of genetic information. Genetic information includes information about genetic tests of applicants, employees, or their family members; the manifestation of diseases or disorders in family members (family medical history); and requests for or receipt of genetic services by applicants, employees, or their family members. Retaliation All of these Federal laws prohibit covered entities from retaliating against a person who files a charge of discrimination, participates in a discrimination proceeding, or otherwise opposes an unlawful employment practice. What to Do If You Believe Discrimination Has Occurred There are strict time limits for filing charges of employment discrimination. To preserve the ability of EEOC to act on your behalf and to protect your right to file Including Disabled People in Poverty Reduction Work: ‘‘Nothing About Us, Without Us’’ REBECCA YEO Action on Disability and Development, Frome, Somerset, UK
- 9. and KAREN MOORE * University of Manchester, UK Summary. — This article argues that the exclusion of disabled people from international development organizations and research reflects and reinforces the disproportionately high repre- sentation of disabled people among the poorest of the poor. The paper commences with a brief exploration of the links between impairment, disability, poverty, and chronic poverty, followed by a discussion of ways in which disability is excluded from development policy. Evidence of the incidence and distribution of disability is then presented. In the final section, the ways in which different institutions challenge poverty and exclusion among disabled people is reviewed. Survey evidence of the limited inclusion of disabled people within development institutions and policies is presented. � 2003 Elsevier Science Ltd. All rights reserved. Key words — poverty, disability, discrimination, developing countries, international organizations, development institutions Because disability and poverty are inextricably linked, poverty can never be eradicated until disabled people enjoy equal rights with nondisabled people. (Lee, 1999, p. 13)
- 10. 1. INTRODUCTION This article argues that there is widespread exclusion of disabled people 1 from interna- tional development organizations and research. This reinforces the disproportionately high representation of disabled people among the poorest of the poor. Such exclusion reflects the wider social, economic and political exclusion of disabled people within household, commu- nity and state. It is unlikely that the millennium development goals (MDGs) will be met unless disabled people are included in every aspect of international development work. Furthermore, an emphasis on these targets may lead to an increased focus on the transient poor. Those living in chronic poverty, among whom evi- dence suggests disabled people are dispropor- tionately represented, may become even further excluded. In the first section of the paper, the links between impairment, disability, poverty and chronic poverty are reviewed. The second part of the paper discusses the ways in which dis- abled people are routinely excluded from in- ternational development policy, practice and research. Existing evidence of the incidence and distribution of disability is then presented, within the context of these limitations. The final section examines the different ways in which
- 11. poverty and exclusion among disabled people are challenged by a range of institutions: gov- ernment; private sector; disabled people�s or- ganizations; international organizatio ns; and World Development Vol. 31, No. 3, pp. 571–590, 2003 � 2003 Elsevier Science Ltd. All rights reserved Printed in Great Britain 0305-750X/03/$ - see front matter doi:10.1016/S0305-750X(02)00218-8 www.elsevier.com/locate/worlddev *The authors would like to thank two anonymous re- viewers and several of the staff and trustees of Action on Disability and Development and the Chronic Poverty Research Centre for helpful comments on an earlier version. 571 nongovernment organizations (NGOs) and donor agencies. Survey evidence of the limited inclusion of disability and disabled people within development institutions and policies is presented. This article supports a right-based, social model approach to disability. This defines dis- ability as the loss or limitation of opportunities
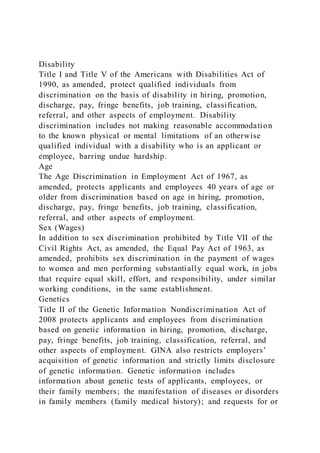
- 12. to take part in the everyday life of the com- munity on an equal level with others due to physical and social barriers. An impairment is a functional limitation within the individual caused by physical, mental or sensory impair- ment (Barnes, 1991). Impairments need not lead to exclusion and inequality if inclusive policies are implemented. 2 In contrast to this, tradi- tional medical and charitable approaches to disability focus on the disabled individual, rather than on the need for societal change. Disability is defined as loss or reduction of functional ability, and disabled people are de- fined by their impairments. Medical or techni- cal interventions may be offered by ‘‘experts’’ to alleviate some impairments. In this model, disabled people are to be pitied and helped, but issues of the right to full inclusion and partici- pation are not addressed. 2. THE VICIOUS CIRCLE OF POVERTY AND DISABILITY Figure 1 illustrates the reasons why disabled people experience disproportionately high rates of poverty, and Figure 2 displays the ways in which being poor dramatically increases the likelihood of getting an impairment, and be- coming disabled. (a) High rates of poverty among disabled people
- 13. (i) Forms of discrimination Disabled people have a higher likelihood of experiencing poverty because of the institu- tional, environmental and attitudinal discrimi- nation faced, from birth or the moment of disablement onward. Institutional discrimination is the process by which disabled people are systematically marginalized by established laws, customs or practices. Discrimination against disabled peo- ple is rooted in widely shared attitudes, values and beliefs. Discrimination can occur, however, irrespective of the intent of the individuals who carry out the activities of the institution. Insti- tutional discrimination exists in many different guises, for example: many NGOs make no at- tempts to include disabled people in their work; in many countries disabled children are not required to go to school and there is no special provision for their needs if they do enroll; banks often do not accept disabled customers; employers often do not consider the needs of disabled applicants. In most countries the physical environment also excludes disabled people. This has been referred to as ‘‘apartheid by design’’ (Imrie, 1996). Buildings with steps and narrow en- trances, inaccessible ‘‘public’’ transport, edu- formal/informal education and employment
- 14. Limited social contacts Fewer skills Low expectations from community and of self Low self esteem Income opportunities further reduced Impairment Discrimination & Disability Excluded from political/legal processes Excluded from even basic healthcare Lack of ability to assert rights High risk of illness, injury and Impairment (see figure 2) Lowest priority for any limited resources e.g. food/clean water/ inheritance/land Lack of support for high costs directly associated with impairment
- 15. Further Poor health/ physically weak Chronic Income Poverty Exclusion Poverty generating Excluded from Figure 1. Disability/poverty cycle. WORLD DEVELOPMENT572 cation and health facilities, a scarcity of infor- mation transcribed into Braille or available on audio tape, and a lack of Sign-Language translators all serve to keep disabled people out, pushed to the margins and without the information they need to participate equally. Prevailing attitudes are the third aspect of disablement. People rationalize the exclusion and ostracism of disabled people and their families in many different ways. Beliefs that disability is associated with evil, witchcraft, bad omens or infidelity persist in many parts of the world (see Lwanga Ntale, Ndaziboneye, & Nalugo, 2002, pp. 7–8 for a Ugandan example).
- 16. Disabled people also often experience suffo- cating overprotection and exclusion from everyday challenges. Low expectations of dis- abled people are often held by wider society as well as by themselves. Russell and Malhotra (2002) have criticized approaches to disability that focus exclusively on attitudinal change. They argue that chang- ing attitudes alone cannot lead to equality. Disability, as they see it, is ‘‘a product of the exploitative economic structure of capitalist society: one which creates (and then oppresses) the so-called �disabled� body as one of the conditions that allow the capitalist class to ac- cumulate wealth.’’ (ii) Poverty implications of disability in childhood and throughout the life-cycle The birth of a disabled child, or the impair- ment of a previously nondisabled child, is often considered a tragedy. The child needs more care and may not be considered to have the poten- tial to support him or herself in the future. Where there are limited resources it may be seen as economically irresponsible to give an equal share to a disabled child who is perceived as un- likely to be able to provide for the family in the future. ‘‘Early lack of investment in disabled children is not just a reflection of ignorance. In situations of poverty this is a desperate but rational decision’’ (Ashton, 1999, p. 1). Thus, disabled children often get last access
- 17. to food and other basic resources. When dis- abled children become ill they are often not given any treatment. In households or com- munities already living in poverty, this exclu- sion is frequently a life or death situation. Erb and Harriss-White (2001, pp. 14, 36 fn10) found that in their focus villages in Tamil Nadu ‘‘disabled children were very rare,’’ and suggest that this is because they are either not disabled or they do not survive. Early and preventable death is the most extreme symptom of poverty; thus, disability must be a central concern of those committed to poverty reduction. Disabled children are less likely to be sent to school (even if physically possible), for fear that: they will not cope; that their disclosure will stigmatize the family (see, for example Hunt, 1966) and affect the marriage prospects of siblings; that they are not a worthwhile investment and others should get priority. UNESCO studies (Hegarty, 1988, 1995, cited by IDDC, 1999) estimate that 98% of ‘‘special to education and employment Forced to accept hazardous working conditions Limited access to land and shelter Unhygienic, overcrowded living conditions
- 18. Poor sanitation Higher risk of illness accident and impairment Chronic Poverty Exclusion Excluded from political/legal processes Lack of ability to assert rights Limited access to healthcare Malnutrition, poor health and physically weak Insufficient or unhealthy food Discrimination & Disability Further Exclusion Income Exclusion and loss of income (See figure 1) Limited access Poverty
- 19. Figure 2. Poverty/disability cycle. DISABLED PEOPLE IN POVERTY REDUCTION WORK 573 needs’’ children in developing countries are de- niedanyformaleducation. 3 InTanzania,recent work suggests that less than 10% of disabled children are enrolled in schools (Rajani, Bang- ser, Lund-Sorensen, & Leach, 2001). But with twice as many disabled boys as girls enrolled, it is likely that the proportion of disabled girls enrolled is less than 5%. In Uganda, according to the 1991 Population and Housing National Census (cited in Okidi & Mugambe, 2002), at least 50% of disabled people had never been to school, only 4.6% had received secondary and tertiary education, and 3.8% had received vo- cational training, which compares poorly with population averages, and even averages for the bottom income quintile of the population. 4 Those children who do get education often receive inferior treatment, have low expecta- tions of themselves and from others and do not get the support they need to participate equally. In Tanzania, it is reported that ‘‘regular’’ schools (i.e., those not specifically designed for
- 20. disabled children) lack the appropriate trans- port, equipment, materials and teachers to meet the needs of disabled students, while the ‘‘few schools set up specifically for children with disabilities lack capacity and resources to meet even basic needs’’ (ADD, 1998, p. 48). Disabled children often have fewer demands placed on them, and therefore may learn less than non- disabled siblings even in an informal setting. Disabled children tend to be excluded from many of the day-to-day interactions that non- disabled children take for granted, limiting ac- quisition of basic social and life skills. Those disabled children that survive early and persistent discrimination are at a huge disadvantage as they grow up having been ex- cluded from formal and informal education. A study in Bahrain in 1981 found that 27% of the population over 10 years of age were illiterate compared with 77% of disabled people (Elwan, 1999, p. 12 citing DISTAT, 1990, Table 6). This has an impact not only on qualifications and experience, but also on levels of confidence and self-esteem. If, during childhood, disabled chil- dren are not included in the community, then as they grow up, their nondisabled peers may not be aware of their existence, let alone their value and rights as equal citizens. As adults, disabled people have restricted employment and income-earning opportunities. This is due to early (in the case of childhood disability) and/or on-going discrimination, re- sulting in lack of education, job opportunities, work experience and confidence. The Uganda
- 21. Participatory Poverty Assessment Process (in Lwanga Ntale et al., 2002, p. 7), based on the voices of disabled and impoverished Ugandans, supports this picture of a ‘‘vicious circle’’ of disability and poverty: Access to work was often denied �on account of inabil- ity to perform physical tasks� and women with minor disabilities were hurriedly married off so that they could eke a living from some household. Those with more severe disability on the other hand were stigma- tized and often denied access to resources of even their families. Disabledpeoplewhosufferdiscriminationand marginalization based on multiple characteris- tics (for example, gender, caste, ethnicity or re- moteness; see Hulme, Moore,& Shepherd,2001) in addition to disability can find it impossible to break out of poverty. Lwanga Ntale et al. (2002) notes that not only are disabled women doubly discriminated against, but that some women become disabled due to rights abuses. 5 Age-related health problems affecting sight, hearing, mobility and mental functioning mean that older people are particularly vulnerable to the poverty-related effects of disability, espe- cially if they are already in a marginal position within the household and community, as is very often the case (see Barrientos, Gorman, & He- slop (this issue)). Mehta and Shah (2001), citing 1991 National Sample Survey data in India,
- 22. report disability levels of about 35% among older males and 40% among older females. Disabled people also often have to face high financial costs resulting both directly and indi- rectly from their impairment(s). Based on a village-level survey in South India, Erb and Harriss-White (2001) found that the direct cost of treatment and equipment for disabled people varied from the equivalent of three days� to two years� income, averaging three months� income; this does not include the indirect costs to fam- ilies and carers, or the opportunity costs of income foregone. Excluded from mainstream social, economic and political opportunities throughout their lives and facing significant financial costs re- lated to their impairments, disabled people and their households are frequently dragged further and further into poverty. As noted by Dennis (1997), many of the children who work on the streets in Tamale, Ghana support disabled adults at home. Disablement, particularly of the main breadwinner in a vulnerable house- hold with limited savings and assets, often WORLD DEVELOPMENT574 initiates an impoverishing cycle of asset liqui- dation and debt, increasing the risk of long- term and intergenerational (i.e., chronic) poverty (Hulme et al., 2001). A study of urban Dhaka found that households with an inca-
- 23. pacitated earner is 2.5 times as likely to have a severely malnourished child than those without (National Institute of Urban Affairs, 1989 cited in (Sinha, Lipton, & Yaqub, 2001)). If, from birth onward, disabled people are not given the resources and access they need to participate, then, ‘‘to assume that this group is a drain on society becomes a self-fulfilling prophecy’’ (Groce, Chamie, & Me, 2000). The full inclusion of disabled people could con- tribute to poverty reduction within households, and entire communities. Yet even many orga- nizations claiming commitment to poverty al- leviation frequently exclude disabled people (see Section 4). (b) High rates of impairment and disablement among the poorest By definition, those living in poverty often have limited access to adequate health care, food, education, shelter, and employment, often enduring hazardous working conditions. All these factors increase the risk of illness, injury and impairment. In many cases, impair- ment then leads to marginalization and exclu- sion, resulting in disability, more exclusion, loss of income, further poverty––many elements of this cycle are certainly interlinked. It is estimated that 100 million people worldwide have impairments caused by mal- nutrition and poor sanitation (Lee, 1999). UNICEF (2002) estimates that
- 24. one child in ten is born with or acquires a physical, mental, sensory, intellectual or psychological disabil - ity due to a preventable disease, congenital causes, malnutrition, micronutrient deficiencies, accidents and injuries, armed conflict and landmines. 6 Most of these factors relate directly to pov- erty. In 1992, the WHO (cited in Lee, 1999) estimated that up to 70% of childhood blindness and 50% of hearing impairment in Africa and Asia are preventable or treatable. Lathyrism, a motor-neuron disease that affects mobility and coordination, is caused by toxins in the cheapest forms of lentils. In Bangladesh, almost everyone who eats these lentils is aware of the risk, but has no alternative (ADD, 1997). In Cambodia, it is estimated that over 70% of recent landmine survivors had been farming or foraging with the full knowledge that they were doing so in areas infested with landmines (ADD, 1997). The need for impairment prevention is evident. Interventions in multiple sectors are required––poverty reduction, immunization, occupational and public safety, education, conflict resolution––and international organi- zations including UNICEF, WHO, ILO and UNDP as well as many donor agencies and NGOs are involved in important and often successful work in these fields. But many im- pairments are not preventable or treatable. Further, medical intervention should not be seen as an alternative to building an inclusive
- 25. environment. It is not inevitable that impair- ment, illness or injury lead to discrimination and disability. It is at this point that the cycle of disability and poverty can be broken, and on this relationship that there has been insufficient focus by development institutions. 3. DISABILITY IN POVERTY RESEARCH Despite the obvious relationships between impairment, disability and poverty, there is little internationally comparable statistical data on the incidence, trends and distribution of impairment and disability, and much national- level data, particularly in the developing world, is unreliable and out-of-date (Erb & Harriss- White, 2001; Yeo, 2001). Neither the UNDP Human Development Report nor the World Bank�s World Development Report include any mention of disability in their regular indices of development. Major international development journals around the world were searched for disability, impairment, handicap and related words (Table 1). Of the 44 journals searched, article titles, keywords and abstracts of 31 journals had no mention of any of these words over the period. In the remaining 13 journals, the words were mentioned in only 24 articles out of all editions of the journals over the five years. The medi- calization of disability issues is common, and one is more likely to find research on disability in developing countries in journals dedicated primarily to health issues rather than poverty issues. Seven of these 24 articles appear in two
- 26. journals that focus on themes of population, psychology and health. This dearth of scholarship on disability and poverty seems to be both a cause and effect of the exclusion of disabled people and disability DISABLED PEOPLE IN POVERTY REDUCTION WORK 575 issues from development policy and practice, as well as an aspect of the very exclusion that defines disability. There are two main reasons for this lack of information: problems of marginalization (including issues of represen- tation), and problems of definition. (a) Problems of marginalization Disability is a socially constructed phenom- enon, largely constructed by nondisabled peo- ple. Extending structural dependency theories, as developed by Galtung (1971) among others, Table 1. Inclusion of impair�, disab� or handicap� in titles, keywords and abstracts of development journals, 1997–2002a Journal Number of articles Bangladesh Development Studies 0 Community Development Journal 2 Developing Economies 0
- 27. Development 3 Development and Socio-Economic Progress 0 Development and Change 0 Development Anthropologist 1 Development in Practice 0 Economic and Political Weekly 4 Economic Development and Cultural Change 0 Economic Development Quarterly 0 Entrepreneurship and regional development 0 European Journal of Development Research 0 Finance and Development 0 Forum for Development Studies 0 Gender and Development 0 Gender, Technology and Development 0 IDS Bulletin-Institute of Development Studies 0 International Development Review 0 International Social Development Review 0 Journal of Developing Areas 0
- 28. Journal of Developing Societies 0 Journal of Development Economics 1 Journal of Development Studies 1 Journal of Human Development 0 Journal of International Relations and Development 0 Journal of International Trade and Economic Development 0 Journal of Rural Development 0 Journal of Rural Economics and Development 0 Journal of Social Development in Africa 2 Oxford Development Studies 0 Population and Development Review 5 Psychology and Developing Societies 2 Public Administration and Development 0 Review of Urban and Regional Development Studies 0 Revue Canadienne D�Etudes Du Developpement––Canadian Journal of Development Studies 1 Savings and Development 0
- 29. Small Enterprise Development 0 Studies in Comparative International Development 0 Sustainable Development 0 Technology and Development 1 Third World Quarterly 0 World Development 1 Total 24 a Searches conducted in February 2002 using several academic search engines including the International Bibliog- raphy of the Social Sciences (�2001 British Library of Political & Economic Science). Full text not searched. WORLD DEVELOPMENT576 from poor (periphery)––rich (center) people and places, can afford a useful means of con- ceptualizing relations between disabled and nondisabled people. Neither poverty nor dis- ability are isolated phenomena. Those living in chronic poverty, among whom disabled people are disproportionately represented, can be con- sidered at the extreme edge of the periphery at community, state and global level. If power were distributed differently, and people with impairments determined the nature
- 30. of the physical environment, for instance, the world could be very different. In the video ‘‘Dreams are the worst,’’ Jupp (1984) describes a physical environment constructed by wheel- chair users. Buildings are created with low ceilings. Those who stand upright, stoop and develop back problems. They are considered incapable of participating fully, are provided with ‘‘special aids’’ and carry collecting tins asking for donations from wheelchair users. Generally excluded from all manner of so- cial, economic and political institutions and interactions, disabled people lack the power to exert an influence on policy-makers and re- searchers. Gathering reliable data on disability therefore has rarely been considered a high priority among those in positions of power. Marginalization of disabled people from re- search manifests itself in several ways. Who undertakes, analyses and writes up the re- search? Where and how is the research under- taken and published? Traditional development research often in- volves nonpoor, nondisabled outsiders ques- tioning people about their lives. The very marginalization that disabled people face can make it difficult and time-consuming for out- side researchers to find and communicate with them. There are several reasons for this. In areas where stigma is attached to having a disabled person in the family, other members of the family may deny the existence of their rel- ative. Disabled people may not physically be able to get to community-meeting places. They
- 31. may also be socially excluded from these places. Research methods often exclude people with impairments. Written surveys are generally in- appropriate for those disabled people who have been excluded from education, or even for ed- ucated people with visual impairments unless the surveys are produced in Braille. Many participatory methods are visually based, hence excluding people with visual impairments; oral discussions are inappropriate for deaf people unless interpretation is provided. It has been suggested that in cases where disabled people are involved in research, their role is often to add token legitimacy to the work. Results of research without real partici- pation of disabled people can often misrepre- sent disabled people�s concerns (Stubbs, 1999; Yeo, 2001). There are several well-worn arguments for the inclusion of disabled people in all aspects of life, including as representatives in the aca- demic as well as political, economic and social spheres. These arguments are similar to those made regarding inclusion of other ‘‘under- represented and vulnerable groups’’––women, people from certain religions, ethnic groups, castes or tribes. Three arguments are fairly uncontroversial. –– There is a prima facie case for interven- tion when the standards of justice and egali- tarianism are undermined by discrimination. Disabled people have a right to be included as equal citizens. If we accept the WHO esti-
- 32. mate that approximately 10% of any popula- tion is disabled, then it must be recognized that a group without a significant proportion of disabled people does not reflect the demo- graphic make-up of the broader community. ––The exclusion of the knowledge and talents of a significant proportion of the population is an inefficient use of human re- sources. ––The increased visibility of disabled people has the potential to provide a positive role model for others, and help overcome nega- tive societal perceptions of disablement. A fourth issue may be more contentious, divid- ing the development community and the dis- ability movement (Lang, 1998). ––Only disabled people can provide the ade- quate and legitimate representation of the interests of other disabled people. Here the assumptions are that disabled peo- ple as a group have a set of common and distinct interests, which are inevitably inade- quately addressed by nondisabled people, but represented by disabled people. These assump- tions are questioned by some: first, disability is crosscut both by other social differences and by differences within the category, based on impairment type and the varied ways societies respond to impairments. Representation of common interests across these divisions may not always be straightforward, whoever is doing the representation. Second, a key question to ask of any interlocutor is what is the social and political basis of their role? While nondisabled
- 33. DISABLED PEOPLE IN POVERTY REDUCTION WORK 577 interlocutors do currently act on behalf of dis- abled people––some more capably and effec- tively than others––the extent to which they have been selected to play this role by disabled people themselves is of central importance. In- terlocutors frequently claim to represent the needs of marginalized people; the legitimacy of this role has to be continually assessed and reassessed (Stiefel & Wolfe, 1994). While all people have the right to choose their own rep- resentatives, the question of who is a legitimate representative remains a common and fraught issue across the range of groups affected by poverty and exclusion. 7 Third, disabled people should be able to represent the interests of any other group, if chosen to do so. While other ‘‘social allegiances’’ may over- ride any affinity a disabled person has for dis- abled people as a category, there are inevitably some experiences that disabled people are better placed to understand than nondisabled people. The involvement of disabled people is abso- lutely crucial when the aim of the group in- volves considering disability issues. Phillips (1998) notes that the ‘‘interests’’ argument de- mands only that there is a threshold presence of
- 34. each group in order to ensure that their con- cerns are adequately addressed. But how many is enough? It is clear, however, that together with the arguments based on justice and egali- tarianism, efficiency, and the importance of role models, this minimum of shared experience is sufficient to support arguments for increasing the inclusion of disabled people in all spheres of public life, including development research and policy. (b) Problems of definition and the limitations of current statistics The UN Disability Statistic�s Compendium (DISTAT; see UNSO, 1990) was created in 1990 in order to gather national disability sta- tistics to make global comparisons. According to the DISTAT database, in 1990 the propor- tion of disabled people varied between less than 1% in Peru and 21% in Austria. DISTAT itself recognizes, however, that the information on disability that does exist is not comparable between countries and regions because of dif- ferences in survey design, definitions, concepts and methods. Definitional changes also mean that there is no reliable panel data on disability. Definitions of disability and impairment are particularly inconsistent across studies with significant differences in what is included as a disability. Erb and Harriss-White (2001) note that even within one country, definitions vary significantly: in India, the 1981 census and the 1981 National Sample Survey used different
- 35. definitions and subdivisions of disability, and neither included many significant impairments such as leprosy. Furthermore, there are cultural variations on what types of impairment lead to marginalization and exclusion. As discussed above, not all impairments cause disability––in societies where glasses are easily available and socially acceptable, being short-sighted need not lead to exclusion and therefore not to dis- ability. Similarly, the level of exclusion and poverty relating to an acquired physical im- pairment is likely to be very different for a corporate executive and a subsistence farmer dependent on their own labor for survival (Elwan, 1999; Erb & Harriss-White, 2001). Mindful of the significant limitations on the amount and comparability of data, this section presents the existing evidence relating to pov- erty and disability. In 1981, UN/WHO studies estimated that on average 10% of any popula- tion is disabled. In 1992, Helander suggested the figure should be modified to 4% for devel- oping countries and 7% for industrialized countries (Metts, 2000). The UNDP estimates a global average of 5% (Coleridge, 1993). There is no consensus as to which figures to use: UN documents and resolutions as well as USAID use 10%, DFID use 4–7%. It is extremely difficult to get accurate or comparable statistics on disability in isolation from changing the attitudes of policy-makers or the wider community. Gathering accurate and comparable statistics on disability issues cannot be separated from tackling the exclusion that
- 36. causes disability and poverty. In India, progress has recently been made in gathering data. The disability movement successfully lobbied for two questions regarding disability to be in- cluded in the 2001 census. The very fact of including these questions is a step toward re- ducing the marginalization that disabled people experience. (c) Existing evidence relating to poverty and disability Helander�s figures suggest that there is a higher proportion of disabled people in richer, more industrialized countries than in poorer WORLD DEVELOPMENT578 countries. This relationship is also likely to hold when one compares urban, rural and re- mote rural areas in poorer countries (Bird, Hulme, Moore, & Shepherd, 2002). There are several probable reasons for this. In more in- dustrialized countries/regions, there are greater detection rates and therefore more accurate statistics. Medical treatment is better, leading to higher survival rates of disabled people as well as longer life expectancies with associated age-related impairments. In more rural-based economies, it may be easier for disabled people to stay hidden from the view of outsiders. This means that their numbers may be underesti- mated. Both Helander�s and UNDP figures have
- 37. been criticized for largely excluding people with ‘‘invisible’’ impairments, including people with HIV/AIDS, learning difficulties or mental health problems. 8 People with invisible im- pairments often face significant discrimination and require considerable support, however, because the impairment may not be immedi- ately obvious upon meeting someone, such people are often excluded from surveys. In general, people will not define themselves as disabled to outside researchers unless there is some advantage in doing so. It is therefore often only visibly impaired people who are included as ‘‘disabled’’ in surveys. In richer industrialized countries where some social security benefits are available, there is some advantage, to balance against the stigma of identifying oneself as a disabled person. Existing information also points to a dis- proportionate number of disabled people in all countries living in extreme poverty. Recent World Bank estimates suggest that disabled people account for as many as one in five of the world�s poorest (Elwan, 1999 cited by Depart- ment for International Development, 2000a, p. 1). This is considerably higher than estimated figures for the proportion of disabled people in society as a whole. In Sri Lanka, approximately 8% of the population are classified as disabled (Department of Social Services, 2000, cited in
- 38. Tudawe, 2001), and about 90% of these dis- abled people are unemployed and dependent on their families. Tanzanian survey data (Chaw- ata, 1992, cited in Lwanga Ntale et al., 2002, p. 4) suggests that households with a disabled member have a mean consumption of less than 60% of the average and a poverty head count 20% greater than average. Crossnational sur- veys have shown that common mental disor- ders are about twice as frequent among the poor as among the rich in Brazil, Chile, India and Zimbabwe (Patel et al., 1999, cited in WHO, 2001), and for many mental illnesses this skewed prevalence also exists in rich countries (WHO, 2001). Aliber (2001) estimates the numbers of indi- viduals and/or households in South Africa within each category of vulnerability 9 that experience chronic poverty on the basis of that characteristic. As expected, Aliber finds that deprivation in terms of hunger is signifi- cantly higher among the 4.6% of households headed by disabled people as compared to households with nondisabled heads. Contrary to evidence from other countries, Aliber finds that unemployment rates are not very much higher among disabled people than the popu- lation as a whole, particularly among black South Africans. There is no significant differ- ence between occupational profiles either. He
- 39. explains that this anomaly is based on the fact that in South Africa unemployment is not only a key cause of poverty, but that: the incidence of joblessness and poverty are so ex- tremely high, being disabled is in a sense superfluous, though it may well make one�s poverty worse. . . .the number of households that are chronically poor be- cause of the disability of the household head. . . is not at all the same thing as a figure purporting to show how many chronically poor households are headed by a disabled person. (Aliber, 2001, p. 34). Village-level studies also have suggested a high incidence of disability among the poorest, while also revealing a more nuanced social understanding of how disability is perceived by different groups of the poor. Erb and Harriss- White (2001) report the results of a 1993 census of three villages in northern Tamil Nadu: 19% of households declared that at least one mem- ber was chronically sick or disabled. Three more villages in the same area were surveyed in 1995, and 6.5% of individual adults described themselves as disabled or incapacitated. Al- though evenly distributed across gender, the prevalence of disability was significantly biased toward caste Hindus: ‘‘scheduled caste people have to be more severely disabled than inhab- itants of the caste settlement before they will publicly acknowledge their infirmity’’ (Erb & Harriss-White, 2001, p. 16). Lanjouw and Stern (1991, cited in McKay & Lawson, 2002) found that chronic poverty was disproportionately high among disabled people as well as other marginalized groups including scheduled tribes,
- 40. DISABLED PEOPLE IN POVERTY REDUCTION WORK 579 older people, women and groups living in re- mote rural areas. What does this admittedly limited evidence tell us? The poorer the area and social group, the more difficult it is to build up an accurate picture of impairments and disability. The poorest are likely to contain a particularly high proportion of disabled people, but these people are difficult to count and research. Finally, where poverty is widespread and persistent, disability may sometimes be an additional di- mension rather than a fundamental cause. Policy-makers need more. As Lwanga Ntale et al. (2002, p. 6) notes, despite increased dis- cussions in Uganda surrounding the links be- tween poverty and disability, ‘‘the information is neither coherent nor comprehensive, and is as such of limited use to policy influencing.’’ 4. INSTITUTIONAL CHALLENGES TO POVERTY AND EXCLUSION AMONG DISABLED PEOPLE In many respects, the exclusion and dis- crimination faced by disabled people bears many similarities to other forms of oppression (Russell & Malhotra, 2002), for example, rac- ism and sexism. There is, however, one funda-
- 41. mental difference: people with some forms of impairment may experience reduced capabili- ties. This is often used as a justification for exclusion. Unless additional practical needs are met, it is indeed more difficult for some dis- abled people to organize, campaign and to work to reduce their own poverty. Yet many disabled people––even those with only mild and moderate forms of impairment––continue to be excluded from poverty reduction work. During the course of the 20th century many different groups and organizations, in different parts of the world, have claimed to be working on behalf of disabled people. Generally this has been through exclusion, segregation and pa- tronizing welfare programs (the charity model); attempts to ‘‘cure’’ the individual disabled person (the medical model); or, most com- monly, a mixture of the two. There has been little recognition of disabled people having equal rights, or of the barriers that are faced (the social model). Governments, development agencies and service providers have frequently either ignored disabled people or, created ‘‘special’’ programs that effectively contribute to the exclusion of disabled people from mainstream society. These disability-targeted programs are gener- ally very expensive to administer, as they do not enable disabled people to fully participate in society. Further, such programs generally only reach small numbers of disabled people, primarily those based in capital cities rather
- 42. than the vast majority of rural-based disabled people. The WHO estimates that only 5% of disabled children in developing countries have access to any kind of rehabilitation (cited by UNICEF, 2002). As noted, many international organizations are involved in rehabilitation and impairment prevention work, much of which is important and worthwhile. But, many impairments are not preventable or treatable. Furthermore, this ap- proachisfrequentlybasedonnondisabledpeople making value judgements regarding the quality of a disabled person�s life. Focusing on impair- ment prevention and rehabilitation to the detri- mentofissuesofexclusionandtheequalrightsof disabled people easily carries the implicit mes- sage that those who do have impairments are somehowexamplesoffailure,tobepitiedandless worthy of full participation. Disabled people should have the option of medical interven- tion and rehabilitation where appropriate. This shouldbebasedoninformedpersonalchoicenot ‘‘expert’’coercion.Medicalinterventionisnotan alternative to building inclusive societies. The disability rights movement began in the 1960s and this has facilitated gradual im- provements in the realm of disability policy. In a UN survey of 79 member states in 1995–96, 69 countries reported having officially recog- nized disability policies (Metts, 2000). Sign- Language is now an officially recognized language in Uganda and Finland. USAID, SIDA and NORAD all now have disability and development policies. The World Bank, DFID,
- 43. World Vision, Voluntary Service Overseas, Oxfam and Save the Children, among others, now have some form of recommendation for inclusive practice. This shift seems to have been largely rhe- torical, however, with limited effects on the poverty experienced by disabled people. Par- ticipants at a regional seminar of the Economic and Social Commission for Asia and the Pacific (ESCAP, 1999, p. 6) on poverty alleviation among rural persons with disabilities noted that, in some areas: the number of people living below the poverty line had been halved over the past several years. However, even though rural disabled persons were the poorest WORLD DEVELOPMENT580 among the poor, they had not been included in the mainstream rural poverty alleviation programs in most of the countries. If disabled people were to achieve equal rights and opportunities, this would contribute to poverty reduction for society as a whole. Participation in the economy, in politics, as well as in social interactions including caring for others, would increase. The inclusion of dis- abled people in self-help or savings and credit groups (Bangladesh and Uganda), and the participation of disabled people as election monitors (Bangladesh, Ghana and Zambia),
- 44. provide examples of positive results at the household, community and state levels (ADD, 2002). While recognizing the potential economic gains of inclusion, it is important for any or- ganization (state, NGO, donor or business) to recognize that investment is required. To make inclusion meaningful, all staff need to be trained in disability equality issues. Individual disabled people may have specific access re- quirements that need to be met before full participation is possible. When disabled people become involved in an organization which is unprepared to be fully inclusive, misconcep- tions about disabled people�s lack of abilities can be reinforced. Such token involvement does little to reduce the marginalization experienced by disabled people. There are global similarities in the exclusion faced by disabled people. There is no country in the world where disabled people�s rights are not violated. The discrimination, oppression, violence and abuse faced by disabled peo- ple does not respect national boundaries, national wealth or national poverty (Hurst, 1999, p. 25). There are also many differences in the ways in which disabled people are organizing, and the influence that they have on policy-makers. If disabled people are to be fully included and substantial poverty reduction achieved, change is needed at several levels. An overview of the work of the main stakeholders is examined
- 45. here, followed by a more detailed review of the work of international development agencies. (a) Government During the last decade, many governments introduced some form of legislation against disability discrimination (e.g., United States, 1990; Zimbabwe, 1992; India, 1995; United Kingdom, 1995; Sri Lanka, 1996; South Africa, 1997; Bangladesh, 2001). But the emphasis of most government disability policies is still on the prevention of impairments, rehabilitation and individual support, rather than on a rights- based approach to social, economic and polit- ical inclusion. Further, both implementation and effects of such legislation have been limited. Tudawe (2001) notes, for example, the very limited implementation of the Protection of the Rights of Persons with Disabilities, passed in Sri Lanka in 1996. Russell and Malhotra (2002) state that ‘‘in 2000, 10 years after passage of the Americans with Disabilities Act, despite a na- tional official unemployment rate of 4.2%, the unemployment rate for working-age disabled population has barely budged from its chronic level of 65–71%.’’ While legislative change is important, ‘‘if the game is possessive individu- alism in a competitive and inegalitarian society, impaired people will inevitably be disadvan- taged, no matter how the rules are changed’’ (Oliver, cited in Russell & Malhotra, 2002). The main motivation for governments that do introduce inclusive approaches to working
- 46. with disabled people has generally been eco- nomic. There is growing recognition of the high economic costs of exclusion. If disabled people are unable to contribute to society then they will inevitably be an economic burden on others. Based on their work in Tamil Nadu, Erb and Harriss-White (2001) estimate the cost of disability 10 to a rural economy to be 5.5% calculated as direct, indirect and opportunity costs of disability as a proportion of total vil- lage income. The economic reason to include disabled people is particularly strong in areas of the world where HIV/AIDS is devastat- ing productive sectors of the economy. It is through inclusion that poverty can be ad- dressed. Recently, the British Department for Inter- national Development recognized that, ‘‘dis- ability is a major cause of social exclusion, and is both the cause and consequence of poverty’’ (Department for International Development, 2000b). DFID published an issues paper enti- tled Disability, Poverty and Development (De- partment for International Development, 2000a) calling for a twin-track approach (see Figure 3). This approach recognizes the fact that dis- abled poor people often have specific needs in addition to those of nondisabled poor people. Therefore, there is the need for specific initia-
- 47. tives working with disabled people as well as DISABLED PEOPLE IN POVERTY REDUCTION WORK 581 for disability issues to be included in all areas of work. There is also a recognition that MDGs are unlikely to be met if disabled people con- tinue to be excluded. In her study of social exclusion and depri- vation in Bangladesh, Jenks (2001) provides an example of a ‘‘twin-track approach’’ in action. She compares two types of intervention aimed at overcoming the stigma associated with lep- rosy: health education for society as a whole, and socioeconomic rehabilitation (SER) of people with leprosy, either through leprosy- specific programs or by ensuring people with leprosy enjoy access to existing programs. Jenks found that ‘‘. . .whilst health education alone could remain abstract and SER schemes could promote �positive segregation,� their cu- mulative effects reinforce each other’’ (Jenks, 2001, p. 55). Overcoming the stigma associated with leprosy (and other diseases such as HIV/ AIDS) is both an important ends in itself, and a major means to prevention and, in the case of leprosy, cure: It was found that whilst it is common for these inter- ventions to remain distinct, it is only by coordinating and integrating. . . that deep-seated prejudices can be removed, facilitating early detection and elimination of leprosy (Jenks, 2001, p. 6).
- 48. South Africa has developed a high profile, crosscutting approach to disability issues. The Office of the Status of Disabled People was established on May 1, 1997 in the Office of the Deputy President. The strategic location of the OSDP in the Presidency has enabled it to access all government departments. This Office now effectively guides the government with respect to inclusion of disability in all legislation, policies, and programs. The South African Parliament now has the highest propor- tion of disabled people of any parliament. A White Paper: An Integrated National Disability Strategy (INDS) was adopted by the Govern- ment on December 3, 1997. It calls for a change in approach to the issues of disabled people–– from a medical model to a human rights/ development model. The Government has adopted a program to ensure that the consti- tutional protection offered to disabled persons in the Bill of Rights becomes a reality. The Ugandan government is widely consid- ered the world leader in terms of political em- powerment of disabled people. More than 47,000 disabled people now work as elected representatives at different levels of govern- ment––but only after the National Union of Disabled People of Uganda (NUDIPU) lob- bied for the inclusive policy. But, even in Uganda disabled people are still severely marginalized and among the very poorest of the poor. As Lwanga Ntale et al. (2002, p. 11) suggests, this limits the effectiveness of inclu-
- 49. sion: Numbers aside, the biggest challenge so far has been that nearly all disabled people elected to these offices are new to politics or even the functioning of organi- Equal rights and opportunities for disabled people Addressing inequalities between disabled and non-disabled persons in all strategic areas of our work Supporting specific initiatives to enhance the empowerment of disabled people Reduced costs of disability for society Contribution of disabled people to poverty reduction enhancement. Figure 3. DFID�s twin track approach to disability, poverty and development. Source: Adapted from DFID (2000a). WORLD DEVELOPMENT582
- 50. zations. They lack skills in advocacy, lobbying, plan- ning, leadership, etc. . . .both the legal and institu- tional framework are fully supportive of disabled people in Uganda. Despite this support the practical application of the letter and spirit of the law is ex- tremely tenuous. This matter becomes particularly ev- ident when one examines the actual programs in place for poverty eradication in Uganda. Disability is not mentioned in Uganda�s Poverty Eradication Action Plan; disabled people remain invisible in the utilization of Poverty Alleviation Funds; and in terms of the 1998 Land Act, ‘‘the prospects for disabled people. . .can at best only be remote’’ (Lwanga Ntale et al., 2002, p. 11-2). Positive shifts in government rhetoric alone are not enough to change the situation. (b) Private sector As the power of the private sector has grown in relation to governments, it has become in- creasingly important to consider how the ac- tions of this sector affect disabled people�s capacity to avoid and escape poverty. There has been a shift of emphasis in many parts of the world toward encouraging ‘‘mainstream’’ businesses to increase the employment of dis- abled people. At the start of the last century, there was a focus on state-run institutions. Over time, this has changed to a preference for sheltered employment schemes. Today, main- stream inclusive employment policies are in- creasingly appearing, at least on paper. These policies do not however generally take
- 51. account of the institutional discrimination in- herent in markets as they now exist. As Harriss- White (1999, p. 137) writes, Market-based provision is largely inappropriate as a response to conditions of disability. This is for three reasons. First, markets respond to purchasing power rather than to need. Second, markets are everywhere deeply embedded in social institutions of prejudice and discrimination. Third, firms comprising markets and competing in them cannot be expected, unaided by the state, voluntarily to add to their cost by adapt- ing workplace sites so as to accommodate disabled workers. Similarly, current strategies for development through increased trade and economic growth will do little for disabled people if the discrim- ination widely excluding disabled people from the labor market is not also addressed. The long-term effects of exclusion mean that many entrepreneurs may not even be aware of the existence of disabled people as potential cus- tomers. The inclusion of disabled people in capitalist employment markets is resisted, as disabled people are perceived as slower, needing more support and therefore leading to increased pro- duction costs (Russell & Malhotra, 2002). Therefore employers frequently choose dis- abled staff only if there is some added incentive, for example, an acceptance of low wages. In many cases, disabled people may be employed
- 52. in menial jobs on low wages. The exploitation and inequality associated with this type of ad- verse incorporation is obscured by the in- creasingly widespread focus on social exclusion (Hickey, 2002). (c) Disabled people’s organizations At the forefront of work to tackle the ex- clusion and poverty widely experienced by disabled people are disabled people�s organi- zations themselves. One of the ways in which disabled people are excluded is that they often have little contact with other disabled people in their own country, let alone in other parts of the world. This leads to isolation and a lack of ability to learn from others� experiences. Indi- vidually, many disabled people do not have the energy or resources to campaign for inclusion. Disabled people have therefore recognized the need to form organizations able to network with each other, and through building a critical mass of opinion, to influence decision-makers. DFID recently recognized a need to support ‘‘initiatives which enhance the skills and ca- pacity of poor people to organize into associ- ations and alliances in order to participate in decision making processes’’ (Department for International Development, 2000c). The number and effectiveness of these orga- nizations varies within and between countries. In some areas these are becoming recog- nized and consulted as legitimate representa- tive bodies. Through these organizations, disabled people have, in some cases, gained
- 53. access to mainstream political process. For ex- ample NUDIPU, in Uganda, successfully lob- bied for political inclusion at all levels. In 1981 an international network of disabled people�s organizations was set up, Disabled People�s International (DPI). This works with orga- nizations in 158 countries around the world, exchanging information and experiences and lobbying for change at the international level. DISABLED PEOPLE IN POVERTY REDUCTION WORK 583 Despite the growth in the numbers, and in- fluence of, disabled people�s organizations worldwide, men with physical impairments still largely dominate these organizations. People with learning difficulties, leprosy, epilepsy, sensory impairments, and mental and emo- tional illness, rarely get equal access to cross- impairment groups. The exclusion and poverty faced by these groups of people (and especially by women) is often even more severe than among other disabled people. This situation is beginning to change as more of the most traditionally marginalized disabled people are increasingly forming their own groups, or pushing to be included in crossimpairment org- anizations. In Uganda, for example, people with mental health problems and epilepsy have been increasingly organizing into their own associations (Uganda Mental Health Associa- tion and the Uganda Association for Epilepsy), as well as pushing for inclusion in NUDIPU.
- 54. People experiencing several different areas of discrimination are frequently marginalized from all groups. For example, women with mental health problems are often marginalized from the disability movement as well as from the women�s movement. In Tanzania, disabled women with HIV/AIDS are extremely iso- lated. 11 Neither women�s organizations, nor disabled people�s organizations, nor organiza- tions of people with HIV/AIDS fully address the crosscutting issues involved. Disabled people�s organizations are working with their allies in international organizations and NGOs to lobby for inclusion in the work of all those involved in poverty reduction. (d) International organizations As described above many international or- ganizations are involved in rehabilitation or prevention work. But, disabled people them- selves are rarely involved in the policy-making of these organizations. This makes it extremely difficult to form effective strategies of full in- clusion. In 1982, the UN introduced a World Pro- gram of Action concerning disabled persons with the aim ‘‘to promote effective measures for prevention of disability, rehabilitation and ‘‘full
- 55. participation’’ of disabled persons’’ (WPA cited by Metts, 2000, p. 15). Then began the Inter- national Decade of Disabled People (1982–91), followed by the Asian and Pacific Decade (1993–2002) and the African Decade (2000–10). These decades undoubtedly serve to raise awareness and focus attention, at least within the UN itself. In 1993, the UN introduced the Standard Rules on the Equalization of Op- portunities for People with Disabilities. These were agreed by all member states of the UN. They are not legally enforceable, but do set an anti-discriminatory and inclusive international standard. Several countries, and organizations within them, have used these Standard Rules to influence their approach to disability. There is currently a campaign led by disabled people�s organizations, to secure a UN Convention on the rights of disabled people. According to Metts (2000), the lack of com- parable information on disability makes it difficult for the World Bank and other inter- national organizations to form cost-effective disability policies or to evaluate different ap- proaches toward tackling poverty and disabil- ity. In 1993, the World Bank developed an international classification system known as Disability Adjusted Life Years (DALY). The stated aim of DALY was to provide interna- tionally comparable data on the global burden of disease and disability in order to prioritize health needs. The assumptions behind DALY are that disabled people inevitably represent a drain on society; that disability can be mea-
- 56. sured in terms of years of burden and loss; and that disability and disease are synonymous. There is no recognition of the discriminatio n and marginalization faced by disabled people, nor consideration of the cultural context of different impairments, nor a recognition of the important contributions disabled people make when fully included. In 1980, the WHO introduced the Interna- tional Classification of Impairment, Disability and Handicap (ICIDH). This defined disability as functional limitations. It did not describe the social impact of having an impairment. In 1997, the ICIDH-2 was developed. This went much further toward recognizing that it is not inevi- table that impairments significantly limit ac- tivities, if exclusion and discrimination are not experienced. In 2001, the International Classi- fication of Functioning, Disability and Health (ICF) was developed. This changed the defini- tion of disability to ‘‘the interaction between the environment and the person with an im- pairment.’’ Environment is classified as atti- tudes, systems, services, legislation as well as the built environment. The ICF in particular goes some way toward providing comparable statistics. But unless the inequalities in power relations, the discrimination and the exclusion WORLD DEVELOPMENT584 faced by disabled people are addressed, these systems will not help tackle poverty. A will-
- 57. ingness to include disabled people in these in- stitutions is needed. (e) NGOs Disability issues are important to all facets of development: equality, empowerment, human rights, poverty and marginalization (Lee, 1999, p. 1). Yet many mainstream development NGOs continue to claim that they are not ‘‘specialists’’ and therefore do not consider disability issues. Specific impairment organiza- tions that work in developing countries include Sound Seekers (working with deaf people in- ternationally), Sightsavers (working with peo- ple with visual impairments), and Handicap International (provision of artificial limbs). These organizations have traditionally worked predominantly on ‘‘cure’’ and prevention of impairment, rather than issues of exclusion and poverty. It may be that this approach provides the means for disabled people to then access mainstream poverty reduction work. This as- sumes, however, that other development orga- nizations are receptive to including disabled people. There are, in any case, several limita- tions in relying on NGOs to meet the needs of disabled people. First, they have relatively small and insecure funding. Second, their pro- vision is unsystematic and discretionary. Third, they are minimally regulated; ‘‘redress by dis- abled people for incompetence is practically impossible to obtain’’ (Harriss-White, 1999, p. 137). Surveys of the work of international devel-
- 58. opment organizations based in the United Kingdom, United States, Australia and Bel- gium have been carried out. It is clear that most mainstream development NGOs still do not fully include disabled people in their work. Many still consider disability a specialist issue that they are not qualified to address. Others claim to work for the whole community, while giving little, or not, consideration to the access requirements of disabled people. In practice, this also excludes disabled people. These ap- proaches are still widely considered acceptable, whereas the open and deliberate exclusion of women from the work of NGOs is no longer considered justifiable by most individuals and organizations in the development field––at least in theory. Table 2 presents the results of a small sur- vey of the members of British Overseas Network for Development (BOND), 12 ad- ministered through a e-mail questionnaire. One-quarter of organizations already special- izing in disability issues responded to the questionnaire, while only about 10% of non- specialist organizations responded; therefore one cannot extrapolate the results to BOND membership as a whole. But the proportion of nonspecialist organizations admitting igno- rance of important UN and DFID disability policies and stating no intentions to increase
- 59. the inclusion of disabled people in their work, may be indicative of a startling trend. Lack of funding was the most commonly cited reason for not including disabled people (23%). Inaccessible offices and a lack of facili- ties to accommodate people with impairments affecting mobility were cited by 13%. Other answers given by respondents when asked to identify the main barriers to including disabled people included: ––‘‘there are no barriers’’ . . . ‘‘none as such’’ . . . ‘‘none to seriously consider’’ ––‘‘have not had to deal with the issue’’ Table 2. Results of survey of BOND Of 250 BOND members: 24 (9%) have disability as a primary focus. Of 30 questionnaire responses (12% response rate): 6 (20%) have disability as a primary focus. Of the remaining 24 (80%) questionnaire responses from organizations without disability as a primary focus: 14 (58%) Had never heard of the UN Standard Rules on Equalization of Opportunities for Disabled People or DFID�s ‘‘Disability, poverty and development’’ paper 12 (50%) Stated they carry out some work specifically
- 60. targeting disabled people 5 (20%) Stated that they aim to include disabled people in all their work 9 (38%) Have no plans to increase the inclusion of disabled people in their work Survey undertaken by Yeo (2001,p. 2). DISABLED PEOPLE IN POVERTY REDUCTION WORK 585 ––‘‘these will only be external to the organi- zation’’ . . . ‘‘societal attitudes’’ . . . ‘‘igno- rance and hostile/negative attitudes on the part of the communities we are trying to reach’’ ––‘‘working with the poorest communities is challenging enough without ensuring the in- volvement of people with disabilities’’ . . . ‘‘difficult to reach the most vulnerable peo- ple’’ ––‘‘do not have the capacity’’ . . . ‘‘do not have staff expertise in disablement’’ –– ‘‘up to our partners overseas’’ . . . ‘‘coun- try programs �mainstream� issues they con- sider most pressing’’ . . . ‘‘work with governments, NGOs and CBOs in a broad way, according to their demands and needs, which have not highlighted disabled peo- ple.’’ As discussed below, many of these answers
- 61. imply a lack of awareness of how disabled people can be included. Mobility International USA (MIUSA) car- ried out a survey among InterAction members (a coalition of over 160 US-based development, relief, refugee and policy orientated agencies) (Singleton, Breslin, Lewis, & Metts, 2001). The results are presented in Table 3. While the methodology and amount of resources used to undertake this survey differ from those used in the BOND survey, the relatively large response rate could also suggest a higher degree of will- ingness among these organizations to at least consider including disability issues. In the United States there are significant national laws and organizational policies re- garding the inclusion of disabled people. The Americans with Disabilities Act was passed in 1990 and was then the most comprehensive disability rights legislation in the world. The United States Agency for International Devel- opment (USAID) also has a disability policy. This states that organizations should ‘‘avoid discrimination against people with disabilities in programs which USAID funds’’ (USAID, 1997, section I). ‘‘Each USAID bureau. . . must determine the best ways to consult with the disabled and with those who advocate on be- half of, or provide services for individuals with disabilities’’ (Section IV, a). InterAction (2001, revised) have also pro-
- 62. duced standards for including disabled people in international development work: disability inclusion strategies will be integrated into each stage of the program process. . . agencies will strive to increase the number of people with disabili- ties. . . each agency will develop a written policy which affirms its commitment to the inclusion of people with disabilities. . . goods and services will be accessible to disabled men, women and children. Despite these policies and the domestic leg- islation, the survey results in Table 3 show high levels of exclusion of disabled people from in- ternational development work by US-based NGOs. Indeed, over half of the respondents did not know what challenges their organizations faced in terms of disability inclusion. This sug- gests that not much consideration has been given to the issue. There is a lack of awareness that inclusion can be achieved even with scarce resources and difficult working conditions. Ac- cording to MIUSA, there is a need for devel- opment organizations to change their thinking, from considering what problems they might face to aiming to include all eligible people and addressing the access issues that really exist: ‘‘Exclusion should never be an acceptable so- lution’’ (Singleton et al., 2001, p. 58). Broadly similar results were obtained from research carried out in Belgium by PHOS (a Table 3. Results of survey of InterAction Of 104 responses (60% response rate; include 75 written
- 63. questionnaires, 77 interviews with chief executives, three in-depth agency assessments) 8(8%) Have policies that address inclusion of disabled people in programme design, implementation, evaluation and partnerships 48 (46%) Have equal opportunity policies that specifically refer to the needs of disabled people Of 48 responses which have equal opportunity policies: 39 (82%) Report no problems implementing such policies <1% Of staff, board members and consultants of these organizations are disabled people Survey undertaken by Mobility International USA. InterAction is a coalition of US-based development, relief, refugee and policy-oriented agencies. WORLD DEVELOPMENT586 platform for work on disability and develop- ment cooperation (PHOS, 2000)) and by the Australian Council For Overseas Aid (see
- 64. Culnane, 2001). The main barriers expressed for not including disabled people were similar in all these surveys: ––Funding and time constraints. ––Some respondents claim they do not want to impose their own views on disability in- clusion on their partner organizations. ––Many organizations did not acknowledge the presence or needs of disabled people within their target groups even though dis- abled people are generally among the poor- est and most discriminated against. ––There is widespread belief that disabled people would not be able to serve under the difficult conditions in developing coun- tries in which organizations work. ––There is a shortage of trained disabled people in the development sector. This may be true but is a self-perpetuating problem. A shortage of trained disabled people could be tackled with fellowships, paid or unpaid internships, and volunteer opportunities. Some mainstream organizations, however, are working to become more inclusive. For example there has been a shift within World Vision, PLAN International and Save the Children Fund (SCF) toward seeing disability as a development issue involving the whole community rather than an individual rehabili- tation issue. SCF aims to support specific dis- ability programs as well as to include a disability perspective in all its work. 5. CONCLUSION
- 65. Despite an increasing awareness within the development field that disabled people are among the poorest, research on poverty and disability is rare and there is widespread ex- clusion of disabled people within development and research organizations. Internationally comparable statistics relating to disabled peo- ple and poverty are lacking. A World Bank report states that, ‘‘most nations are now hampered by a paucity of data and information on disability’’ (Metts, 2000, p. xiii). This is itself a result of the exclusion and poverty faced by disabled people. Most research that does exist has not been undertaken by disabled people themselves, nor has it included disabled people in forming the agenda. Yet, The real repositories of local knowledge on disability in particular countries are the disabled people that live there, and the most efficient way to tap into their local knowledge is to provide them with mechanisms for making their needs known (Metts, 2000, p. xv). As the USAID policy states, regular consul- tation with disabled people�s organizations should be an integral part of all poverty re- duction work. In the words of the international disability movement, ‘‘nothing about us, with- out us.’’ Reliable statistics relating to the numbers of disabled people living in poverty can go a long way to motivate policy-makers to take action. Depending on how the research is carried out, it could also help to change the power relations that exclude disabled people. An investment of
- 66. time and financial resources is required before many disabled people will be able to effectively conduct research themselves. One of the main hurdles to full inclusion cited by policy-makers is financial cost. It is suggested that research is needed on the long- term costs of excluding disabled people to set against the purely economic costs of inclu- sion––there are large financial and social costs of excluding disabled people from economic activity, as well as opportunity costs of exclu- sion from community life as a whole. There is also a need to highlight further the ways in which disabled people are currently excluded even from the work of those devel- opment organizations claiming to work on poverty issues. This involves assessing the ex- tent to which disabled people are included in policy-making, consultation and implementa- tion of poverty reduction work. The budgetary proportion of development organizations work that is spent on disabled people could be compared with the proportion of disabled people living in poverty. In order to improve the situation, it would be useful to gather information on the most ef- fective policies, laws and regulations that can be undertaken in order to include disabled people in poverty reduction work. It is recom- mended that a twin track approach is adopted. This means that, in addition to the specific work suggested above, disability issues should be included as a crosscutting theme in all pov-
- 67. erty reduction work and research. As long as disability is treated solely as a specialist issue and not included in mainstream work, the ex- clusion and hence the poverty that disabled people face will not be addressed. 13 DISABLED PEOPLE IN POVERTY REDUCTION WORK 587 The most important element of any research is that it is not undertaken as an alternative to tackling the exclusion and poverty faced by disabled people. The research itself should challenge power relations. As Stubbs (1999, p. 276) writes, ‘‘don�t get stuck on details that do not make a difference to people�s lives, this is a great academic distraction!’’ Until the barriers that disabled people face are recognized and addressed, there can be no substantive or sus- tainable change in the marginalization and poverty experienced. NOTES 1. The chosen terminology of the disability movement varies between cultures and languages. Although in some countries the disability movement prefers ‘‘people with disabilities,’’ in this article ‘‘disabled people’’ is
- 68. used, as this is favored in the United Kingdom. Individ- ual disabled people both inside and outside the disability movement may prefer to use other terms. 2. Myopia, for instance, is an impairment that only becomes a disability if a short-sighted individual cannot access adequate lenses. 3. Obviously, definitions of ‘‘special needs’’ are prob- lematical. Moreover, the study only refers to ‘‘formal provision’’ and therefore does not take account non/ informal systems or children who are ‘‘casually inte- grated’’ without being labeled. But, the review covered 58 countries and was the first such review to have been conducted. 4. Uganda now has a policy of free primary education for four children in any family. Disabled children and girls are theoretically given priority. There are however frequent media reports of husbands beating wives for registering disabled children. ADD staff also recount
- 69. many examples of finding parents hiding their disabled children and giving priority to siblings (ADD, 1998). 5. ‘‘It is estimated that over 100 million girls and women in more than 28 cities in Africa alone are disabled as a result of female genital mutilation. These result into physical and psychological consequences that range from morbidity differences, impaired sexual func- tion and infertility because of infection to an increased risk of HIV infection’’ (Lwanga Ntale et al., 2002, p. 4). 6. See Goodhand (2001) for a discussion of the interrelationship between poverty, chronic poverty, conflict and disability. Not only does conflict lead to impairments, but it also undermines health care and other basic services, exacerbating disability. Often dis- abled people are also least able to flee violent conflict. 7. This article is in no way intended to represent the interests of disabled people or any other group. It is written to highlight the need to consult with, and
- 70. include, disabled people in poverty reduction work. Neither of the authors has been chosen as a represen- tative and do not claim to take that role. 8. Personal communication (Rachel Hurst, Disability Awareness in Action, 2002). 9. The rural poor; households with AIDS orphans and AIDS sufferers; the street homeless; crossborder mi- grants; and households headed by women, disabled people, older people, and entrenched farm workers. 10. Where disability directly affects 8% of adult men and 10% of adult women, and indirectly affects one-third of all households. 11. Personal observation by Kevan Moll (Action on Disability and Development, 2000). 12. A network of 260þUK-based voluntary organi- zations working in international development and development education. 13. The Chronic Poverty Research Center (CPRC) is currently involved in specific research in Bangladesh and
- 71. Uganda looking at the extent of chronic poverty among disabled people. The CPRC also aims to ensure that disability issues are included in all its country-specific and thematic work. REFERENCES Action on Disability and Development (1997). Tour report of visit to Cambodia. Frome: ADD (unpub- lished). Action on Disability and Development (1998). ADD Uganda annual report. Kampala: ADD. WORLD DEVELOPMENT588 Action on Disability and Development (2002). Annual report. Frome: ADD. Aliber, M. (2001). Study of the incidence and nature of chronic poverty and development policy in South Africa: an overview. Chronic Poverty Research Centre Working Paper 3. Manchester: Institute of Development Policy and Management/CPRC. Ashton, B. (1999). Promoting the rights of disabled children globally disabled children become adults: some implications. Frome: ADD.
- 72. Barnes, C. (1991). Disabled people in Britain and discrimination: A case for anti-discrimination legisla- tion. London: Hurst and Co./BCODP. Barrientos, A., Gorman, M., & Heslop, M. (this issue). Old age poverty in developing countries: reconstruct- ing dependence in later life. World Development, 31(3), 555–570 . Bird, K., Hulme, D., Moore, K., & Shepherd, A. (2002). Chronic poverty and remote rural areas. Chronic Poverty Research Centre Working Paper 13. Man- chester: Institute of Development Policy and Man- agement/CPRC. Coleridge, P. (1993). Disability, liberation and develop- ment. Oxford: Oxfam. Culnane, T. (2001). Research on disability inclusion for Australian Council for Overseas Aid (ACFOA). Melbourne: Culnane Consulting International. Dennis, C. (1997). Truck Pushers, Grain Pickers and Grandmothers: ‘Street Children’ and Some Gender and Age Aspects of Vulnerability in Tamale, Northern Ghana. Gender Aspects of Aging, GAINS, IN- STRAW. Department for International Development (2000a). Disability, poverty and development. London/East Kilbride: DFID. Department for International Development (2000b). Achieving sustainability––poverty elimination and the environment. London/East Kilbride: DFID.
- 73. Department for International Development (2000c). Realising human rights for poor people. London/East Kilbride: DFID. Economic and Social Commission for Asia and the Pacific (1999). Report on ‘Field Study-cum-Regional Seminar on Poverty Alleviation among Rural Persons with Disabilities’ (December 6–15, Hyderabad). ES- CAP/Ministry of Rural Development, Government of India. Elwan, A. (1999). Poverty and disability: A review of the literature. Background Paper for the World Devel- opment Report 2000/2001. Washington, DC: World Bank. Erb, S., & Harriss-White, B. (2001). The economic impact and developmental implications of disability and incapacity in adulthood a village study from S. India. Paper to the workshop Welfare, demography and development, September 11–12, Downing Col- lege, Cambridge. Galtung, J. (1971). A structural theory of imperialism. Journal of Peace Research, 8, 81–117. Goodhand, J. (2001). Violent conflict, poverty and chronic poverty. Chronic Poverty Research Centre Working Paper 6. Manchester: Institute of Develop- ment Policy and Management/CPRC. Groce, N., Chamie, M., & Me, A. (2000). Measuring the quality of life: rethinking the World Bank�s disability adjusted life years. Disability World (on-line serial), 3. www.disabilityworld.org/June-July2000/Interna- tional/DALY.html.
- 74. Harriss-White, B. (1999). Onto a loser: disability in India. In B. Harriss-White, & S. Subramanian (Eds.), Ill fare in India: essays on India�s social sector in honor of S. Guhan (pp. 135–158). New Delhi: Sage Publi- cations. Hegarty, S. (1995). Review of the present situation in special needs education. Paris: UNESCO. http:// www.unesco.org/education/pdf/281_79.pdf. Hegarty, S. (1988). Review of the present situation of special education. Paris: UNESCO. Hickey, S. (2002). Introductory paper for CPRC theory workshop on inequality. (Unpublished) Manchester: Institute of Development Policy and Management/ CPRC. Hulme, D., Moore, K., & Shepherd, A. (2001). Chronic poverty: meanings and analytical frameworks. Chronic Poverty Research Centre Working Paper 2. Manchester: Institute of Development Policy and Management/CPRC. Hunt, P. (Ed.). (1966). Stigma; the experience of disabil - ity. London: Geoffrey Chapman. Hurst, R. (1999). Disabled people�s organizations and development: strategies for change. In E. Stone (Ed.), Disability and development (pp. 25–35). Leeds: Disability Press. Imrie, R. (1996). Disability and the city: international perspectives. London: Chapman Publishers.
- 75. InterAction (2001). Approved disability amendments with revisions. Available at: http://www.miusa.org/intldev/ usaid/index.html#standards. International Disability and Development Consortium (1999). Report of a one day seminar Seen and Heard: Promoting the rights of disabled children globally (October 5). Brighton: IDDC. Jenks, S. (2001). In combating social exclusion in what way are interventions on the ‘excluded’ related to interventions in the ‘excluding society? Overcoming the social stigma associated with leprosy: rehabilitation and prevention in Bangladesh. Unpublished Masters of Science dissertation, International Development Department, University of Birmingham, Birming- ham. Jupp, K. (1984). Dreams are the worst. London: Healthcare productions Ltd. Lang, R. (1998). A critique of the disability movement. Asia Pacific Disability Rehabilitation Journal, 9(1), 4– 8. Lee, H. (1999). Discussion paper for Oxfam: disability as a development issue and how to integrate a disability perspective into the SCO. Oxford: Oxfam. Lwanga Ntale, C., Ndaziboneye, B., & Nalugo, J. (2002). Chronic poverty and disability in Uganda. Forthcoming Chronic Poverty Research Centre Working Paper. Manchester: Institute of Develop- ment Policy and Management/CPRC. McKay, A., & Lawson, D. (2002). Chronic poverty:
- 76. A review of current quantitative evidence. Chronic Poverty Research Centre Working Paper DISABLED PEOPLE IN POVERTY REDUCTION WORK 589 http://www.disabilityworld.org/June- July2000/International/DALY.html http://www.disabilityworld.org/June- July2000/International/DALY.html http://www.unesco.org/education/pdf/281_79.pdf http://www.unesco.org/education/pdf/281_79.pdf http://www.miusa.org/intldev/usaid/index.html#standards http://www.miusa.org/intldev/usaid/index.html#standards 15. Manchester: Institute of Development Policy and Management/CPRC. Mehta, A. K., & Shah, A. (2001). Chronic poverty in India: Overview study. Chronic Poverty Research Centre Working Paper 7. Manchester: Institute of Development Policy and Management/CPRC. Metts, R. (2000). Disability issues, trends and recommen- dations for the World Bank. Washington, DC: World Bank. Okidi, J. A., & Mugambe, G. K. (2002). An overview of chronic poverty and development policy in Uganda. Chronic Poverty Research Centre Working Paper 11. Manchester: Institute of Development Policy and Management/CPRC. Phillips, A. (1998). Democracy and representation: or, why should it matter who our representatives are? In A. Phillips (Ed.), Feminism and politics (pp. 226–
- 77. 238). Oxford: Oxford University Press. PHOS (Platform Handicap En Ontwikkelingssamenwer- king/Platform disability and development coopera- tion) (2000). Available at: www.phos.be. Rajani, R., Bangser, M., Lund-Sorensen, U., & Leach, V. (2001). Situation analysis of children in Tanzania. Dar es Salaam: Government of Tanzania and UNICEF Tanzania. Russell, M., & Malhotra, R. (2002). The political economy of disablement: advances and contradic- tions. In L. Panitch & C. Leys (Eds.), Socialist Register 2002: a world of contradictions. (http:// www.yorku.ca/socreg/RusMal.htm). Singleton, T. L., Breslin, M. L., Lewis, C., & Metts, R. L. (2001). Gender and disability: a survey of InterAc- tion member agencies. findings and recommenda tions of inclusion of women and men with disabilities in international development programmes. Eugene, OR: Mobility International USA (MIUSA). Sinha, S., Lipton, M., & Yaqub, S. (2001). Poverty and �damaging fluctuations�: how do they re- late? Journal of Asian and African Studies, 37(2). Stiefel, M., & Wolfe, M. (1994). A voice for the excluded: Popular participation in development: Utopia or necessity. London: UNRISD and Zed Press. Stubbs, S. (1999). Engaging with difference: soul-search- ing for a methodology in disability and develop- ment research. In E. Stone (Ed.), Disability and
- 78. Development (pp. 257–259). Leeds: Disability Press. Tudawe, I. (2001). Chronic poverty and development policy in Sri Lanka: overview study. Chronic Poverty Research Centre Working Paper 9. Manchester: Institute of Development Policy and Management/ CPRC. UNICEF (2002). Child Protection. Child Disabilities website. www.unicef.org/programme/cprotection/ focus/disabilities/facts.htm, accessed September 5, 2002. UNSO (1990). Disability statistics compendium statistics on special population groups (DISTAT). (Series Y, No. 4). New York: UN. World Health Organization (2001). The World Health Report 2001 mental health: new understanding, new hope. Geneva: WHO. Yeo, R. (2001). Chronic poverty and disability. Chronic Poverty Research Centre Working Paper 4. Man- chester: Institute of Development Policy and Man- agement/CPRC. USAID (1997). USAID disability policy paper USAID/ General Notice Policy Paper 09/12/97. Washington DC: Bureau for Policy & Program Coordination. (Available at: http://www.usaid.gov/about/disability/ disabpol.fin.html). WORLD DEVELOPMENT590 http://www.phos.be