1. Univariate analysis results of early and delayed postoperative complications and mortality stratified by body mass index
(BMI) status
Surgical complication(s)
Normal weight
BMI 18.5-24.99
N=28, N (%)
Overweight
BMI 25-29.99
N=56, N (%)
Obese
BMI ≥ 30
N=45, N (%)
p Value
Wound infection 0(0) 0(0) 1(1.2) 0.390
Anastomotic leak 0(0) 1(1.8) 4(8.9) 0.090
Pulmonary Embolism/DVT*
0(0) 2(3.6) 0(0) 0.266
Pneumonia 0(0) 2(3.6) 4(8.9) 0.189
Cardiovascular 3(10.7) 9(16.1) 7(15.6) 0.793
Any complication(s)†
3(10.3) 12(41.4) 14(48.3) 0.123
30 days Mortality 1(3.6) 0(0) 1(2.2) 0.414
*
Deep Venous Thrombosis; †
Defined as the presence of one or more of the complications listed above in a single patient.
Effect of Body Mass Index on Operative Outcome after Robotic-Assisted
Ivor-Lewis Esophagectomy (RAIL): Retrospective Analysis of 129 Cases
at a Single High-Volume Tertiary Care Center
Ahmed I. Salem, M.D., Matthew R Thau, M.S., Tobin Joel Crill Strom, M.D., AM Abbott M.D., M.S.c, Nadia Saeed Khaldoun Almhanna,
M.D., M.S.c., Sarah E Hoffe, M.D., Ravi Shridhar, M.D., PhD, Richard C. Karl, M.D., Kenneth L. Meredith, M.D., FACS
Section of Surgical Oncology – Division of General Surgery University of Wisconsin School of Medicine and Public Health
Introduction:
The impact of body weight on outcomes after robotic-
assisted esophageal surgery for cancer has not been
studied. We examined the short-term operative outcomes
in patients according to their body mass index (BMI)
following robotic-assisted Ivor-Lewis esophagectomy
(RAIL) at a high-volume tertiary-care referral cancer
center and evaluated the safety of robotic surgery in
patients with an elevated BMI.
Methods:
A retrospective review of all patients who underwent
RAIL for pathologically confirmed distal esophageal
cancer was conducted. Patient demographics,
clinicopathologic data, and operative outcomes were
collected. We stratified BMI according to WHO criteria;
normal range is defined as a BMI range of 18.5 to 24.9
kg/m². Overweight is defined as a BMI range of 25.0 to
29.9 kg/m² and obesity is defined as a BMI of 30 kg/m²
and above. Statistics were calculated using Wilcoxon
Rank-Sum and Spearman Coefficient tests with a p-value
of 0.05 for significance.
Results:
129 patients (103 men, 26 women) with median age of 67
(30-84) years were included. The majority of patients,
76% (N=98) received neoadjuvant therapy. When
stratified by BMI twenty-eight (22%) were normal
weight, fifty-six (43%) were overweight and forty-five
(35%) were obese. All patients had R0 resection. Median
operating room (OR) time was 407 (239-694) minutes.
When stratified by BMI, medians of OR time across the
normal weight, overweight and obese groups were 387
(254-660) minutes, 395 (310-645) minutes and 445 (239-
694) minutes respectively. Median estimated blood loss
(EBL) was 150 (25-600) cc. When stratified by BMI,
medians of EBL across the normal weight, overweight
and obese groups were 100 (50-500) cc, 150 (25-600) cc
and 150 (25-600) cc respectively. Obesity significantly
correlated with longer OR time (p=0.05) but without
significant increased EBL (p=0.348). Among the three
BMI groups there was no difference in postoperative
complications including thrombotic events (pulmonary
embolism and deep venous thrombosis) (p=0.266),
pneumonia (p=0.189), anastomotic leak (p=0.090),
wound infection (p=0.390), any cardiac events (p=0.793)
or 30 days mortality (p=0.414).
Conclusion:
Our data study demonstrates that patients with esophageal cancer and an elevated BMI
undergoing RAIL have increased operative times but no significantly increased EBL during the
procedure. Other potential morbidities did not differ with the robotic approach.
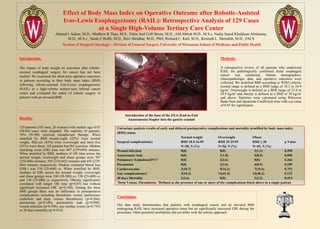
Introduction of the base of the EEA (End-to-End
Anastomosis) Stapler into the gastric conduit