Scaphoid fractures
•Download as PPTX, PDF•
6 likes•7,079 views

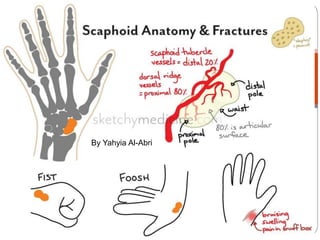
scaphoid anatomy and fractures

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to Scaphoid fractures
Similar to Scaphoid fractures (20)
More from Yahyia Al-abri
Recently uploaded
Recently uploaded (20)
Scaphoid fractures
- 1. Yahyia alabri Junior Scaphoid fractures By Yahyia Al-Abri
- 2. Almost 75% of all carpal fractures. Mechanism is a fall on the hand with wrist extended. The critical movement is probably a combination of dorsiflexion and radial deviation
- 3. Clinical features Tenderness upon palpation at the snuffbox and volar tubercle. Range of motion (ROM) is reduced, but not dramatically. Swelling around the radial and posterior aspects of the wrist is common
- 4. Special test Watson test
- 5. Imaging X-rays most sensitive radiographic evaluation includes 4 views: PA, lateral, pronated oblique (60° pronated oblique), and ulnar deviated oblique (also described as 60° supinated oblique). The fracture may not be seen in the first few days after the injury. Two weeks later, the break is usually much clearer, Due to bone resorption at the fracture site and slight displacement of fragments
- 7. CT scan is more sensitive for diagnosing a scaphoid fracture. MRI is the definitive way to confirm or exclude a diagnosis of scaphoid fracture if the technique is available.
- 8. Treatment If the x-ray looks normal but the clinical features are suggestive of a fracture, the patient must not be discharged. second x-ray 2 weeks later. Meanwhile, the wrist is immobilized in a cast
- 9. Treatment Fracture of the scaphoid tubercle a crepe bandage is applied and movement is encouraged. Undisplaced fractures of the waist can be treated in plaster for 8 weeks; 90% should heal. If the scaphoid is tender, or the fracture still visible on x-ray, when non-operative treatment is chosen, the cast is re-applied and retained for a further 6 weeks.
- 10. Displaced fractures Reduce the fracture and to fix it with a compression screw. Proximal pole fractures a poor rate of healing a long time in plaster (and even then sometimes not heald) a percutaneous screw.
- 11. COMPLICATION NON-UNNION AVASCULAR NECROSIS OSTEOARTHRITIS
Editor's Notes
- Scaphoid fracture is not very likely when tubercle palpation does not provoke pain in the snuffbox.
- Watson (scaphoid shift) testThe patient sits with the forearm pronated. The examiner takes the patient's wrist into full ulnar deviation and extension. The examiner presses the patient's thumb with his/her other hand and then begins radial deviation and flexion of the patient's hand. If the scaphoid and lunate are unstable, the dorsal pole of the scaphoid subluxes over the dorsal rim of the radius and the patient complains of pain, indicating a positive test.
- Fractures of the scaphoid – diagnosis (a) The initial anteroposterior view often fails to show the fracture. The fracture may be (b) through the proximal pole, (c) the waist, or (d) the scaphoid tubercle. (e) A CT scan is useful for showing the fracture (a) configuration.
- CT scan is more sensitive for diagnosing a scaphoid fracture; it is particularly useful in confirming the alignment of the bone fragments if surgery is planned, or to confirm whether the fracture has united or not.
- An alternative is to arrange an MRI scan (or, if not available, a CT scan) which will definitely detect the fracture even if it was not visible on the x-ray.
- usually needs no splintage and should be treated as a wrist sprain;
- Proximal pole fractures have such a poor rate of healing that unless the patient is prepared to spend a long time in plaster (and even then sometimes the fracture does not heal), or unless the techniques are not available, then there is a tendency to fix these with a percutaneous screw. can be manipulated and treated in plaster, but the outcome is less predictable