
More Related Content
What's hot
More from primary
More from primary (20)
Recently uploaded
Recently uploaded (20)
Diabetes Flowsheet
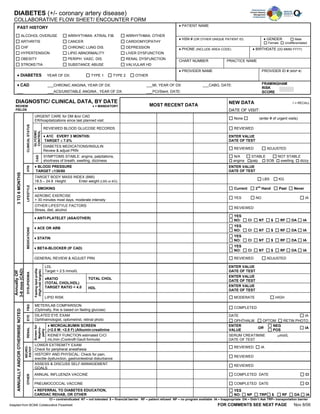
- 1. DIABETES (+/- coronary artery disease) COLLABORATIVE FLOW SHEET/ ENCOUNTER FORM ♦ PATIENT NAME PAST HISTORY ALCOHOL OVERUSE ARRHYTHMIA: ATRIAL FIB ARRHYTHMIA: OTHER ♦ HSN # (OR OTHER UNIQUE PATIENT ID) ♦ GENDER Male ARTHRITIS CANCER CARDIOMYOPATHY Female Undifferentiated CHF CHRONIC LUNG DIS. DEPRESSION ♦ PHONE (INCLUDE AREA CODE) ♦ BIRTHDATE (DD-MMM-YYYY) HYPERTENSION LIPID ABNORMALITY LIVER DYSFUNCTION OBESITY PERIPH. VASC. DIS. RENAL DYSFUNCTION CHART NUMBER PRACTICE NAME STROKE/TIA SUBSTANCE ABUSE VALVULAR HD ♦ PROVIDER NAME PROVIDER ID # (MSP #) ♦ DIABETES YEAR OF DX: TYPE 1 TYPE 2 OTHER ♦ CAD ___CHRONIC ANGINA, YEAR OF DX: ___MI, YEAR OF DX: ___CABG, DATE: FRAMINGHAM RISK ___ ___ACS/UNSTABLE ANGINA , YEAR OF DX: ___PCI/Stent. DATE: SCORE DIAGNOSTIC/ CLINICAL DATA, BY DATE NEW DATA √ = RECALL REVIEW ♦ = MANDATORY MOST RECENT DATA FIELDS DATE OF VISIT: URGENT CARE for DM &/or CAD None (enter # of urgent visits) ER/hospitalizations since last planned visit CLINICAL STATUS REVIEWED BLOOD GLUCOSE RECORDS REVIEWED GLYCEMIC CONTROL ♦ A1C EVERY 3 MONTHS: ENTER VALUE TARGET ≤ 7.0% DATE OF TEST DIABETES MEDICATIONS/INSULIN REVIEWED ADJUSTED Review & adjust PRN SYMPTOMS STABLE: angina, palpitations, N/A STABLE NOT STABLE CAD shortness of breath, swelling, dizziness angina palp. SOB swelling dizzy ♦ BLOOD PRESSURE ENTER VALUE HTN TARGET ≤130/80 DATE OF TEST 3 TO 6 MONTHS TARGET BODY MASS INDEX (BMI) LBS KG 18.5 – 24.9 Height: Enter weight (LBS or KG) LIFESTYLE nd ♦ SMOKING Current 2 Hand Past Never AEROBIC EXERCISE YES NO IA > 30 minutes most days, moderate intensity OTHER LIFESTYLE FACTORS REVIEWED Stress, diet, alcohol YES ♦ ANTI-PLATELET (ASA/OTHER) NO: CI NT $ RF DA IA YES ♦ ACE OR ARB MEDICATIONS NO: CI NT $ RF DA IA YES ♦ STATIN NO: CI NT $ RF DA IA YES ♦ BETA-BLOCKER (IF CAD) NO: CI NT $ RF DA IA GENERAL REVIEW & ADJUST PRN REVIEWED ADJUSTED LDL ENTER VALUE Fasting lipid profile 3-6 mos (CAD) Target < 2.5 mmol/L DATE OF TEST (High-risk targets) Annually OR DYSLIPIDEMIA ENTER VALUE ♦RATIO TOTAL CHOL DATE OF TEST (TOTAL CHOL/HDL) TARGET RATIO < 4.0 ENTER VALUE HDL DATE OF TEST LIPID RISK MODERATE HIGH METER/LAB COMPARISON FBG COMPLETED (Optimally, this is based on fasting glucose) ANNUALLY AND/OR OTHERWISE NOTED DILATED EYE EXAM DATE IA EYE Ophthalmologist, optometrist, retinal photo OPHTHALM OPTOM RETIN PHOTO ♦ MICROALBUMIN SCREEN ENTER NEG Screen for OR IA Nephro- RENAL (<2.0 M: <2.8 F) (Albumin:creatinine VALUE POS pathy KIDNEY FUNCTION estimated CrCl SERUM CREATININE μmol/L mL/min (Cockroft-Gault formula) DATE OF TEST LOWER EXTREMITY EXAM REVIEWED IA NEURO- PATHY Check for peripheral anesthesia HISTORY AND PHYSICAL: Check for pain, REVIEWED erectile dysfunction, gastrointestinal disturbance ASSESS & DISCUSS SELF-MANAGEMENT REVIEWED GOALS ANNUAL INFLUENZA VACCINE COMPLETED DATE CI OTHER PNEUMOCOCCAL VACCINE COMPLETED DATE CI ♦ REFERRAL TO DIABETES EDUCATION, YES CARDIAC REHAB, OR OTHER NO: NP TRP $ RF DA IA CI – contraindicated NT – not tolerated $ – financial barrier RF – patient refused NP – no program available IA – Inappropriate DA – Didn’t Ask TRP– transportation barrier Adapted from BCMA Collaborative Flowsheet FOR COMMENTS SEE NEXT PAGE Nov 8/06
- 2. DIABETES (+/- coronary artery disease) COLLABORATIVE FLOW SHEET/ ENCOUNTER FORM ♦ PATIENT NAME ♦ HSN # (OR OTHER UNIQUE PATIENT ID) ♦ GENDER Male Female Undifferentiated ♦ PHONE (INCLUDE AREA CODE) ♦ BIRTHDATE (DD-MMM-YYYY) CHART NUMBER PRACTICE NAME ♦ PROVIDER NAME PROVIDER ID # (MSP #) COMMENTS Adapted from BCMA Collaborative Flowsheet Nov 8/06