Myeloproliferative Disorders Other Than CML
•Download as PPT, PDF•
9 likes•3,774 views

Hematology/Oncology

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Myeloproliferative Disorders Other Than CML
Similar to Myeloproliferative Disorders Other Than CML (20)
Recently uploaded
Recently uploaded (20)
Myeloproliferative Disorders Other Than CML
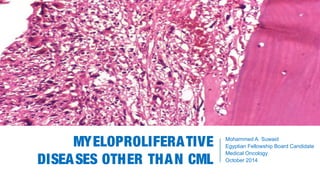
- 1. MYELOPROLIFERATIVE DISEASES OTHER THAN CML Mohammed A. Suwaid Egyptian Fellowship Board Candidate Medical Oncology October 2014
- 2. DEFINITION Myeloproliferative diseases (MPDs) are a heterogenous group of disorders characterized by cellular proliferation of 1 or more hematologic cell lines in the peripheral blood, distinct from acute leukemia. Genetic Mutation
- 3. CLASSFICATION The type of disorder is often based on the predominant cell line that is affected, but because blood counts are often abnormal in more than one cell line, diagnoses based upon blood counts alone may be inaccurate. According to the French-American-British (FAB) classification, chronic myeloproliferative diseases consist of 4 diseases: chronic myelogenous leukemia (CML); polycythemia vera (PV); essential thrombocythemia (ET); and agnogenic myeloid metaplasia (AMM), which is also known as myelofibrosis (MF). In 2002, the World Health Organization (WHO) proposed an alternate classification schema for these diseases, adding chronic neutrophilic leukemia (CNL) and chronic eosinophilic leukemia (CEL)/hypereosinophilic syndrome (HES).
- 4. CLASSFICATION WHO FAB Chronic myelogenous leukemia Chronic myelogenous leukemia Polycythemia vera Polycythemia vera Essential thrombocythemia Essential thrombocythemia Chronic idiopathic myelofibrosis Agnogenic myeloid metaplasia/myelofibrosis Chronic neutrophilic leukemia ... Chronic eosinophilic leukemia/hypereosinophilic syndrome ... Comparison of FAB and WHO Classifications of Chronic Myeloproliferative Diseases.
- 5. OVERVIEW In CML, the predominant feature is a leukocytosis with a left shift. A mild anemia, normal to elevated platelet count, and a peripheral blood basophilia is often seen. In PV, the predominant features are elevated red blood cell indices (RBC count, hemoglobin, and hematocrit). Patients often also have a mild leukocytosis and thrombocytosis. In ET, the predominant feature is an elevated platelet count. Patients also often have a mild leukocytosis and polycythemia. In PMF, the predominant feature is evidence of extramedullary hematopoiesis in the form of hepatomegaly, splenomegaly, and lymphadenopathy. Patients often have a mild anemia, but their WBC and platelet counts can be quite variable. Leukoerythroblastosis (tear drops, nucleated RBCs and early myeloid progenitors [including blasts]) is often seen in the peripheral blood.
- 7. QUESTION #01 A 34 yo woman presents for her annual health visist and a CBC reveals a WBC count of 11.2, Hb of 17.1 and a platelet count of 390,000. Peripheral blood was sent to evaluate for the JAK2 mutation and was negative. What is the most appropriate next step in the evaluation of the patient? A) Repeat CBC in 3 months B) BM biopsy C) Red cell mass assay D) Repeat JAK2 testing to ensure laboratory accuracy E) Referral to hematology Polycythemia Vera
- 8. DEFINITIONS A hematocrit greater than 48% (♀) or 52 % (♂) constitutes polycythemia. Likewise, a hemoglobin of >16.5 g/dL (♀) or >18.5 g/dL (♂) raises the suspicion for polycythemia . Absolute polycythemia is characterized by an increase in red blood cell (RBC) mass. Common causes include: 1) primary polycythemia (polycythemia vera) 2) hypoxia 3) carboxyhemoglobinemia 4) cushing’s syndrome or corticosteroid use 5) erythropoietin-secreting tumors Polycythemia Vera
- 9. DEFINITIONS Relative polycythemia is characterized by a decrease in plasma volume. There are two common causes: 1) Dehydration (e.g., from vomiting, diarrhea, excessive sweating, or diuretics) can deplete plasma volume, leading to a relative polycythemia. 2) Stress erythrocytosis (Gaisböck’s polycythemia) actually results from contraction of the plasma volume and is therefore a misnomer. This benign disorder is seen most often in hypertensive, obese men. Red Blood Cell Mass Assay is used to distinguish an absolute versus a relative polycythemia. Polycythemia Vera
- 10. Polycythemia vera is a stem cell disorder characterized as a panhyperplastic, malignant, and neoplastic marrow disorder. Its most prominent feature is an elevated absolute red blood cell mass because of uncontrolled red blood cell production. This is accompanied by increased white blood cell (myeloid) and platelet (megakaryocytic) production, which is due to an abnormal clone of the hematopoietic stem cells with increased sensitivity to the different growth factors for maturation. DEFINITIONS Polycythemia Vera
- 11. CLINICAL PRESENTATION Symptoms: ▪ Non-specific complaints: headache, weakness, dizziness, and excessive sweating. ▪ Pruritus, especially following a warm bath or shower. ▪ Erythromelalgia, or burning pain in the feet or hands accompanied by erythema, pallor, or cyanosis. ▪ Symptoms related to either an arterial or venous thrombosis (CVA, MI, DVT, Budd Chiari syndrome or other portal venous thrombosis). Polycythemia Vera
- 12. CLINICAL PRESENTATION Signs: ▪ Facial plethora (ruddy cyanosis) ▪ Splenomegaly ▪ Hepatomegaly ▪ Gouty arthritis and tophi Polycythemia Vera
- 13. DIAGNOSTIC CRITERIA Diagnostic criteria for PV as per the 2008 revised WHO guidelines include both major and minor criteria. Diagnosis requires the presence of both major criteria and one minor criterion or the presence of the first major criterion together with two minor criteria. Major WHO criteria are as follows: 1.Hemoglobin > 18.5g/dL in men and > 16.5g/dL in women, or other evidence of increased red blood cell volume 2.Presence of JAK2617V F or other functionally similar mutation, such as JAK2exon 12 mutation Polycythemia Vera
- 14. DIAGNOSTIC CRITERIA Minor WHO criteria are as follows: 1.Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) with prominent erythroid, granulocytic, and megakaryocytic proliferation 2.Serum erythropoietin level below the reference range for normal 3.Endogenous erythroid colony formation in vitro two major + one minor OR first major + two minor Polycythemia Vera
- 15. JAK2 MUTATIONS AND MPDS Receptor Tyrosine Kinase Maps to chromosome 9p Valine to phenylalanine substitution at amino acid 617 (V617F) in pseudokinase domain of JAK2 allows for the constitutive activation of the receptor Somatic acquired mutation High incidence in PV (~95%) Lower incidence in ET (~50%) and PMF (~50%) Polycythemia Vera
- 16. OUTCOMES AND TREATMENT Survival outcomes in PV are affected by: 1) hyperviscosity and associated ischemic sequelae 2) thromboses independent of hyperviscosity 3) transformation to myelofibrosis or acute myeloid leukemia (~3%-10%) Polycythemia Vera
- 17. OUTCOMES AND TREATMENT Therapeutic Options in PV: 1) Low Risk: phlebotomy (to an Hct of <45 in ♂ and <42 in ♀) + low dose aspirin (81 mg daily) – decreases risk of thrombosis 2) High Risk: phlebotomy + ASA + hydroxyurea. In patients who are refractory to or intolerant of hydroxyurea, interferon-alpha can be used as an alternative. Busulfan is also an option for patients older than 65 years. High Risk for Thrombosis: ▪ age over 60 ▪ prior thrombosis ▪ platelet count >1,500,000/μl ▪ presence of cardiovascular risk factors Polycythemia Vera
- 18. JAK2 INHIBITORS IN MPDS A number of inhibitors of the JAK2 kinase have been developed and inhibit the proliferation and survival of JAK2 V617F transformed cell lines in-vitro Clinical studies have been initiated and demonstrate some symptomatic improvement as well as improvement in splenomegaly in a number of patients, but the percentage of JAK2+ progenitor cells have not been significantly altered. However, a large number of trials continue at this time. Leads to speculation that JAK2 may not be sufficient for the development of MPDs and there may be an earlier genetic mutation that is driving the phenotype. Polycythemia Vera
- 19. QUESTION #01 A 34 yo woman presents for her annual health visist and a CBC reveals a WBC count of 11.2, Hb of 17.1 and a platelet count of 390,000. Peripheral blood was sent to evaluate for the JAK2 mutation and was negative. What is the most appropriate next step in the evaluation of the patient? A) Repeat CBC in 3 months B) BM biopsy C) Red cell mass assay D) Repeat JAK2 testing to ensure laboratory accuracy E) Referral to hematology Polycythemia Vera
- 20. QUESTION #01 A 34 yo woman presents for her annual health visist and a CBC reveals a WBC count of 11.2, Hb of 17.1 and a platelet count of 390,000. Peripheral blood was sent to evaluate for the JAK2 mutation and was negative. What is the most appropriate next step in the evaluation of the patient? A) Repeat CBC in 3 months B) BM biopsy C) Red cell mass assay D) Repeat JAK2 testing to ensure laboratory accuracy E) Referral to hematology Polycythemia Vera
- 22. DEFINITION Thrombocytosis is defined as a platelet count > 450,000 cells/μL Etiology of Thrombocytosis Primary - if the thrombocytosis is caused by a myeloproliferative neoplasm, the platelets are frequently abnormal and the patient may be prone to both bleeding and clotting events. Secondary - if thrombocytosis is secondary to another disorder (reactive), even patients with extremely high platelet counts (e.g., > 1,000,000 cells/μl) are usually asymptomatic. Essential Thrombocythemia
- 23. DIFFERENTIAL DIAGNOSIS Differential Diagnosis of secondary thrombocytosis: 1. Malignancies 2. Infections and inflammatory disorders (e.g., Crohn’s disease) 3. Post surgical status 4. Connective tissue disorders 5. Iron deficiency anemia 6. Splenectomy 7. Recovery of the bone marrow from a stress (chemotherapy or alcohol) 8. Essential Thrombocythemia Essential Thrombocythemia
- 24. CLINICAL PRESENTATION Asymptomatic (~ 30-50%) Vasomotor symptoms including headache, syncope, atypical chest pain, acral paresthesia, livedo reticularis, and erythromelalgia Thrombosis and hemorrhage occur to various degrees in 5%-25% of patients Early satiety and abdominal bloating due to splenomegaly Essential Thrombocythemia
- 25. DIAGNOSTIC CRITERIA 2008 WHO Diagnostic Criteria for Essential Thrombocytosis 1. Platelet count > 450,000 2. Megakaryocytic proliferation with large, mature morphology and with little granulocytic or erythroid expansion 3. Not meeting WHO criteria for CML, PV, PMF, MDS or other myeloid neoplasm 4. Demonstration of the JAK2V617F or other clonal marker or lack of evidence of a secondary (reactive thrombocytosis) Diagnosis of ET requires the presence of all four major criteria Essential Thrombocythemia
- 26. OUTCOMES Most patients with ET enjoy a normal life expectancy Like PV, the major risks are secondary to thrombosis and disease transformation: 15-year cumulative risks: thrombosis - 17% risk clonal evolution into either myelofibrosis (4%) or AML (2%) High risk for thrombosis: age ≥ 60 prior thrombosis long-term exposure to a plt count of > 1,000,000/μl Essential Thrombocythemia
- 27. TREATMENT Low Risk: ▪ Age <60 years ▪ No previous history of thrombosis ▪ Platelet count <1 million/μl → aspirin (81 mg daily) if vasomotor Sx or other medical need for ASA → if otherwise low risk and plt >1.5 X 106 , screen for an acquired von Willebrand disease before instituting ASA Essential Thrombocythemia
- 28. TREATMENT High Risk: ▪ Age ≥60 years ▪ A previous history of thrombosis → hydroxyurea + aspirin (81 mg daily) → if plt >1.5 X 106 , screen for an acquired von Willebrand disease before instituting ASA → anagrelide is an option, but when combined with hydroxyurea, it was associated with an increased risk of arterial thrombosis, venous thrombosis, serious hemorrhage, or death from vascular causes Essential Thrombocythemia
- 30. QUESTION #02 A 62-year-old man undergoes a routine examination. He notes increasing fatigue of 8 months’ duration but states he can perform his usual daily activities. He has no fever, night sweats, anorexia, or weight loss. The medical history is noncontributory, and he takes no medications. On physical examination, vital signs are normal. The spleen is palpable three finger breadths below the left midcostal margin. There is no lymphadenopathy or hepatomegaly. Laboratory studies indicate a hemoglobin level of 12.5, WBC of 14,400 and a platelet count of 148,000. Primary Myelofibrosis
- 31. QUESTION #02 The bone marrow cannot be aspirated, but the bone marrow biopsy reveals a hypercellular marrow with extensive fibrosis and abnormal-appearing megakaryocytes. Results of conventional cytogenetic testing are normal. The JAK2mutation assay is positive. Fluorescence in situ hybridization of the bone marrow for the (9;22) translocation is negative. Which of the following is the most appropriate management of this patient now? A) Allogeneic hematopoietic stem cell transplantation B) Danazol C) Hydroxyurea D) Imatinib E) Observation Primary Myelofibrosis
- 32. DEFINITION Myelofibrosis is a rare bone marrow disease in which the proliferation of an abnormal clone of hematopoietic progenitor cells in the bone marrow and other sites results in fibrosis, or the replacement of the marrow with collagenous connective tissue fibers. The term myelofibrosis alone usually refers to primary myelofibrosis (PMF) or chronic idiopathic myelofibrosis (cIMF). Agnogenic myeloid metaplasia and myelofibrosis with myeloid metaplasia (MMM) also overlap on the same spectrum. Primary Myelofibrosis
- 33. CLINICAL PRESENTATION Signs and Symptoms: ▪ asymptomatic (15% - 30%) ▪ severe fatigue ▪ splenomegaly ▪ hepatomegaly ▪ fever and night sweats ▪ signs or symptoms of anemia or thrombocytopenia ▪ foci of extramedullary hematopoiesis may occur in almost any organ ▪ bone or joint involvement Primary Myelofibrosis
- 34. DIAGNOSIS CBC Findings: anemia (Hb<10 in 50% of pts); anisocytosis, poikilocytosis, teardrop- shaped red blood cells (dacrocytes), and nucleated red blood cells leukoerythroblastosis (increased presence of immature myeloid cells and nucleated erythrocytes in the circulating blood WBC and Plt counts are variable (ranging from low to high) with increased circulating CD34+ precursor cells BM Biopsy shows increased fibrosis (reticulin fibers or mature collagen) Primary Myelofibrosis
- 35. DIAGNOSIS Imaging Studies Skeletal radiographs show increased bone density and a prominence of bony trabeculae. Increased bone density may be patchy, resulting in a mottled appearance. MRI may help to assess the severity and progression of the disese. Marrow patterns observed on an MRI examination of the proximal femur appear to correlate with clinical severity. Liver and splenic enlargement is observed on ultrasonograms and computed tomography (CT) scans. Primary Myelofibrosis
- 36. DIAGNOSIS Genetic Testing Cytogenetic studies of bone marrow are helpful in excluding CML, MDS, or other chronic myeloid disorders. However, these may be difficult to obtain due to "dry tap" on bone marrow aspirates in over 50% of patients. FISH studies or PCR assay testing for bcr:abl may be helpful in excluding CML (this may also be performed on peripheral blood). FISH studies for abnormalities associated with MDS, such as del 7, 7q-, and 5q-, may also be helpful. Primary Myelofibrosis
- 37. DIAGNOSTIC CRITERIA 2008 WHO Diagnostic Criteria for Primary Myelofibrosis Major: 1. Megakaryocytic proliferation and atypia with either: reticulin or collagen fibrosis or If no fibrosis, megakaryocytic expansion must be associated with increased BM cellularity 2. Does not meet WHO criteria for CML, PV, MDS, or other myeloid neoplasm 3. Demonstration of the JAK2 V617F mutation or other clonal marker OR no other evidence of a reactive marrow fibrosis Primary Myelofibrosis
- 38. DIAGNOSTIC CRITERIA Minor: 1. Leukoerythroblastosis (immature RBCs and WBCs in the PB) 2. Increased LDH 3. Anemia 4. Palpable splenomegaly Diagnosis PMF requires the presence of all three major criteria and two minor criteria Primary Myelofibrosis
- 39. OUTCOMES As fibrosis progresses, cytopenias worsen leading to a transfusion dependency Symptoms related to extrmedullary hematopoiesis may increase (worsening splenomegaly and ‘B’ symptoms) Rarely patients may transform to acute leukemia (~ 4%) ▪ clonal evolution was common in these patients ▪ some evidence that in all MPDs, cases of JAK2- acute leukemia arise out of a JAK2+ MPD, causing speculation that there are additional genetic changes that either initiate and/or propagate these diseases Despite the lack of transformation to leukemia, three-year survival rate is approximately 52% Primary Myelofibrosis
- 40. RISK ASSESSMENT Mayo Scoring System (pts age < 60) Score Median Survival 0 173 mo 1 61 mo ≥ 2 26 mo Transplant Scoring System (pts age < 55) Score Median Survival 0 or 1 15 yrs ≥ 2 3 yrs Risk Factors: •Hemoglobin <10 g/dL •White blood cell count <4000/μl or >30,000/ μl •Absolute monocyte count >1000 μL •Platelet count <100,000/ μL Risk factors: •Hemoglobin <10 g/dL •‘B’ symptoms present (eg, fever, NS, weight loss) •Circulating blasts >1 percent Primary Myelofibrosis
- 41. TREATMENT Risk stratification is critical in deciding on therapeutic options ‘Low Risk’ without symptoms – expectant management ‘Low Risk’ with symptoms – hydroxyurea androgens and corticosteroids splenectomy if adequate BM hematopoiesis splenic irradiation thalidomide or lenalidomide ‘High Risk’ and age < 55(?) – ruxolitinib (Jakafi) (JAK1/JAK2 inhibitor) reduced intensity allogeneic BMT Primary Myelofibrosis
- 42. QUESTION #02 A 62-year-old man undergoes a routine examination. He notes increasing fatigue of 8 months’ duration but states he can perform his usual daily activities. He has no fever, night sweats, anorexia, or weight loss. The medical history is noncontributory, and he takes no medications. On physical examination, vital signs are normal. The spleen is palpable three finger breadths below the left midcostal margin. There is no lymphadenopathy or hepatomegaly. Laboratory studies indicate a hemoglobin level of 12.5, WBC of 14,400 and a platelet count of 148,000. Primary Myelofibrosis
- 43. QUESTION #02 The bone marrow cannot be aspirated, but the bone marrow biopsy reveals a hypercellular marrow with extensive fibrosis and abnormal-appearing megakaryocytes. Results of conventional cytogenetic testing are normal. The JAK2mutation assay is positive. Fluorescence in situ hybridization of the bone marrow for the (9;22) translocation is negative. Which of the following is the most appropriate management of this patient now? A) Allogeneic hematopoietic stem cell transplantation B) Danazol C) Hydroxyurea D) Imatinib E) Observation Primary Myelofibrosis
- 44. QUESTION #02 The bone marrow cannot be aspirated, but the bone marrow biopsy reveals a hypercellular marrow with extensive fibrosis and abnormal-appearing megakaryocytes. Results of conventional cytogenetic testing are normal. The JAK2mutation assay is positive. Fluorescence in situ hybridization of the bone marrow for the (9;22) translocation is negative. Which of the following is the most appropriate management of this patient now? A) Allogeneic hematopoietic stem cell transplantation B) Danazol C) Hydroxyurea D) Imatinib E) Observation Primary Myelofibrosis
- 45. THANK YOU
Editor's Notes
- Chronic idiopathic myelofibrosis, late phase. Hypocellular marrow, fibrosis and osteosclerosis.
- Left shift: there are more immature precursors present than you would normally see.
- Livedo reticularis is a common skin finding consisting of a mottled reticulated vascular pattern that appears as a lace-like purplish discoloration of the skin.[1]The discoloration is caused by swelling of the venules owing to obstruction of capillaries by thrombi. It can be caused by any condition that makes venules swell. Erythromelalgia is a rare neurovascular peripheral pain disorder in which blood vessels, usually in the lower extremities or hands, are episodically blocked (frequently on and off daily), then become hyperemic and inflamed. There is severe burning pain (in the small fiber sensory nerves) and skin redness. The attacks are periodic and are commonly triggered by heat, pressure, mild activity, exertion, insomnia or stress.
- Anagrelide works by inhibiting the maturation of platelets from megakaryocytes.[6] The exact mechanism of action is unclear, although it is known to be a phosphodiesterase inhibitor.[7] It is a potent inhibitor of phosphodiesterase-II. It inhibits PDE-3 and phospholipase A2.